In Vitro Starch and Protein Digestibility of Disease Specific Nutrition Formulations
 , Asna Urooj*
, Asna Urooj* Department of Studies in Food Science and Nutrition, Manasagangotri, University of Mysore, 570006, Mysuru, Karnataka, India.
Corresponding Author Email: asnaurooj@foodsci.uni-mysore.ac.in
DOI : http://dx.doi.org/10.12944/CRNFSJ.7.1.07
Download this article as:
![]()
Nutritional supplements are used in the management of diseases. The composition and form of nutrients in the supplements depend on the altered needs and gastrointestinal function of patients. The nutrition label of the supplements lacks information on the in vitro digestibility of nutrients which ultimately decides the availability of nutrients for absorption. Various factors that influence digestibility and availability include source of the nutrient, gut functionality, processing, physicochemical properties in the food matrix and inter-nutrient interactions. This study aimed at analyzing the in vitro starch and protein digestibility of six commercially available food formulations used in various disease conditions. The starch digestibility index (SDI) ranged from 64.47 ± 1.92 to 82.35 ± 2.71 and rapidly available glucose (RAG) from 26.06 ± 0.61 to 44.23 ± 0.38g per 100g. Dietary fiber content was inversely related with SDI (r - 0.845). The protein digestibility ranged from 41.42 ± 2.67 - 96.84 ± 1.01%. Formulations containing isolated forms of whey, casein and soy protein had a higher digestibility than in combinations. Besides information on the nutrient content, specifying the digestion characteristics of disease specific commercial formulations will help in their judicious use in meeting the nutritional requirements in various disease conditions.
KEYWORDS:Digestibility; Fiber; Maltodextrin; Nutrition Supplements; Protein; Starch Fractions
Introduction
Nutrition is an integral part of health, both in preventing certain diseases or in treating them. Malnutrition is a condition defined as “a state of the body resulting from the lack of intake or uptake of nutrients that leads to altered body composition (decreased fat free mass) and body cell mass, leading to diminished physical and mental function and impaired clinical outcome from a disease”.1 Malnutrition can be induced by a state of starvation, burden of a disease on the body, by the process of ageing or by a combination of these. The malnutrition that develops due to an underlying disease is termed as disease related malnutrition, the etiology of which may or may not include inflammation. Malnutrition is associated with higher morbidity and mortality. The provision of nutritional therapy in the clinical setting and the community involves use of nutrition supplements/formulations in the form of liquids or powders in patients who are fed enterally or in conditions where oral diet alone is insufficient to meet the altered nutritional needs. Research in the field of clinical nutrition supports the use of oral nutrition supplements in treating disease induced malnutrition to induce favorable outcomes in patients.2 The use of oral nutritional supplements with an aim to meet the nutrient needs in patients who are at risk of malnutrition or who are malnourished is recommended.3 The selection of a suitable nutrition supplement or a formulation is based on various factors such as individual nutrient needs of patients as influenced by the disease, gut functionality, mode of enteral access available etc.4 Various commercial disease-specific formulations are available with nutrient profile suitable in managing disease conditions such as diabetes mellitus (to maintain normal blood glucose levels), renal disease (to reduce electrolyte burden and to meet the altered protein needs), hepatic disease (to meet desired protein intake in a state of hepatic encephalopathy), hyper metabolic conditions (to boost the immune function), respiratory distress (to limit carbon dioxide production or to attenuate inflammatory stress), malabsorption (to enhance absorption of nutrients by use of partially hydrolyzed forms) etc.5
Apart from their nutritive value, the functional attributes of these nutrition formulations such as digestibility/accessibility and bioavailability are equally important as they determine the nutritional quality of the formulation. The presence of a nutrient in a certain proportion in a formulation cannot be assumed to be totally utilized by the gut and made available for utilization. The digestibility and bioavailability of nutrients varies on several factors such as the source of the nutrient, dosage and form, type and extent of processing, physicochemical properties in a food matrix and nutrient-nutrient interactions, if any.6 For instance, glucose released from sucrose and starch is readily digestible and absorbable than from starch/maltodextrin hydrolysis.7 The addition of resistant starch or fiber can delay the glucose release, thus modifying the functionality of carbohydrates in the formulation. The selection of protein with high biological value can significantly impact the proportion and type of amino acids available after absorption to the cells of the body for utilization.8 Nutrition labeling in the commercial formulations does not always include information on these aspects. Hence, this study was planned to analyze the in vitro starch and protein digestibility of selected commercial disease specific food formulations and to corroborate its relevance to the disease condition for which they are prescribed.
Materials and Methods
Materials
The commercial formulations were procured from a local pharmacy from Mysuru, India and stored in ambient condition. Digestive enzymes used in the analysis were invertase (Hi- Media, RM 5983), amyloglucosidase (Sigma Aldrich –A9913), α-amylase (A3176), pepsin (Hi-media, rm1250) and pancreatin (Hi-Media, 3867). GODPOD kit (Auto span, 93DP100) was used to analyze the liberated glucose. All the other chemicals used for analyses were of analytical grade.
Selection of Formulations
Six formulations were selected for analysis in this study. Each formulation had a different profile of nutrients as they were intended for use in patients with specific disease conditions, necessitating altered nutrient intake. The ingredients used as sources of macronutrients in the formulations are presented in table no.1. The features of the six formulations along with the disease condition they are formulated are listed below:-
Pulmo-1- High fat-Calorie dense formulation (Pulmonary disorders/ Respiratory distress)
Pulmo-2 – High fat-Calorie dense formulation (Pulmonary disorders/ Respiratory distress)
DM – Low glycemic index formulation (Diabetes management)
Elem – Formulation with macronutrients in the pre-digested form (Malabsorption)
Rene – Calorie dense-high protein-low electrolyte formulation (Renal disease with dialysis therapy)
Can –High protein-Calorie dense formulation (Any hyper-metabolic condition)
Analysis of starch fractions
The free glucose (FG), total glucose (TG), glucose liberated at 20 minutes and 120 minutes of hydrolysis were measured in the samples by the multi enzymatic assay with colorimetric endpoint.9 The samples were subjected to hydrolysis using invertase, amylase and amyloglucosidase. The free glucose in the sample and the glucose liberated from sucrose were measured following the hydrolysis with invertase. The glucose liberated at 20 minutes (G20) and 120 minutes (G120) of digestion with α-amylase were measured. The total glucose in the samples were measured after gelatinizing the starch in boiling water and addition of 7M potassium hydroxide followed by enzymatic hydrolysis with amyloglucosidase. A blank containing buffer and guar gum and glucose standard were also analysed simultaneously. The glucose values and concurrent starch fractions obtained in this assay represent the glucose liberated from maltodextrins present in the formulations.9 The starch fractions were estimated using the following formulae:-
Total Starch (TS)= (TG-FG)*0.9
Rapidly Digestible Starch (RDS) = (G20-FG)*0.9
Slowly Digestible Starch (SDS) = (G120-G20)*0.9
Resistant starch (RS) = TS- (RDS+SDS)
The starch digestibility index (SDI) provides an overview of the rate of starch digestion and rapidly available glucose (RAG) and was calculated using the following formulae :-
Starch Digestibility Index (SDI) = (RDS /TS)*100
Rapidly Available Glucose (RAG) = FG + G20 + Glucose released from sucrose
Additionally, the available carbohydrates for digestion were calculated by adding the free glucose and digestible fractions of starch namely RDS and SDS of each formulation and their proportion out of the total carbohydrate content was calculated and expressed as percentage of available carbohydrates.
In Vitro Protein Digestibility
The in vitro protein digestibility of the formulations was analyzed by the method described by Akeson and Stahmann.10 The samples were taken in quantities equivalent to 100mg of protein for analysis. Casein was used as a reference. The samples were taken in 50ml centrifuge tubes and 15 ml of 0.1 N hydrochloric acid containing 1.5 mg of pepsin was added to all the samples and incubated at 37oC for 3 hours. After 3hours of incubation, 7.5 ml of 0.1 N sodium hydroxide and 7.5 ml of 0.2M phosphate buffer containing 4 mg of pancreatin was added to all the samples and were incubated at 37oC for 24 hours. After 24 hours of incubation 10% trichloroacetic acid was added to stop the reaction and the mixture was allowed to stand for two hours. The samples were then centrifuged at 3000rpm for 15 minutes and the protein content in the supernatant was analyzed by Kjeldahl method. The protein digestibility of casein was used as the reference. The protein digestibility was calculated using the following formula:-
Protein Digestibility (%)=Protein content in the supernatant /Total protein content of the samples*100
Statistical Analysis
The values are presented as mean ± SD. ANOVA was applied to test the difference between the mean values of the samples. Post hoc analysis of inter sample differences was conducted using Tukey’s test. A P-value less than 0.05 was considered to be statistically significant. The analyses were performed using Statistical Package for the Social Sciences (SPSS) version 19.0 software for Windows.
Results
Themacro nutrient composition and food ingredients used as the source of macronutrients of the six commercial formulations (as per the nutrition label on the formulations) are shown in table no.1 and table no.2, respectively. The macronutrient proportion used in the formulations reveals their intended use. Formulation Pulmo-1 (low carbohydrate –high fat formula for respiratory illness) and Elem (pre-digested macronutrients for use in patients with mal-absorption) were intended to be used as a meal replacement or as a supplement to the oral diet. All other formulations indicated its use as a supplement to the oral diet only and each varied in their nutritional composition. Formulation DM is designed for patients with uncontrolled diabetes mellitus and thus has a higher amount of fiber. Formulation Pulmo-2 has lower carbohydrate and higher fat content suitable for patients with respiratory distress. Formulation Rene is designed for patients on dialysis support and Can for patients with hyper metabolic conditions, thus have higher protein content compared to other formulations.
Table No 1: Macronutrient Composition of the Formulations
| Formulation | Pulmo-1 | Pulmo-2 | DM | Elem | Rene | Can |
| Energy (kcals) | 355 | 501 | 450 | 468 | 486 | 450 |
| Carbohydrates (g/100g) | 25 | 48 | 43.8 | 60 | 31 | 44 |
| Protein (g/100g) | 14.8 | 21 | 20.2 | 21 | 41 | 35 |
| Fat (g/100g) | 22.1 | 25 | 20 | 16 | 22 | 15 |
| Dietary Fiber (g/100g) | Nil | 3 | 7.2 | 4 | Nil | 2 |
| Fructo-oligosaccharides as a part of fiber (g/100g) | Nil | Nil | 3.2 | Nil | Nil | 2 |
Table No 2: Food Sources of Macronutrients Used in the Formulations
| Nutrient | Carbohydrate | Protein | Fat |
| Food Sources | Maltodextrin, sugar, Fructo-oligosaccharides, Soya fiber, guar gum fiber, | Whole milk powder, skimmed milk powder, sodium caseinate, whey protein concentrate, soy protein isolate, hydrolyzed whey protein | Oleic sunflower oil powder, vegetable fat powder, Whole milk powder, peanut oil, evening primrose oil powder |
Starch Fractions
The total starch and the starch fractions in the samples are given in table no.3 with all the values expressed as g/100g. The total starch content of the formulations ranged between 26.70-52.56g/100g and was found to be significantly different (p<0.05) except for formulations Pulmo-2 and DM (P=0.838) and; Pulmo-1 and Rene (P=0.229) which had similar total starch values. The total starch was the lowest in Pulmo-1 (26.70g/100g). Although Rene is intended to be a high calorie-high protein formulation, the total starch content (28.48g/100g) was low. The variation observed in the starch content is due to the differences in the proportion of carbohydrate sources used in the formulation, which is based on their intended use in various medical conditions. RDS was found to be highest in the formulation Elem (39.03g/100g) and lower in formulation Pulmo-1 and DM (16.40g and 21.38g/100g respectively) and complimented with the requirements of the respective disease condition. The RDS values of Pulmo-2 and Can did not differ significantly (P=0.156). SDS fraction was significantly higher (p<0.05) in the formulations DM, Elem and Can compared to others. Resistant starch was found to be highest in the low glycemic formulation DM, followed by formulations Elem, Can, Pulmo-2 and Pulmo-1. The glucose content from added sucrose was 3.92 ± 0.02 and 4.29 ± 0.01 g/100g in the formulations Pulmo-1 and Pulmo-2, respectively. Other formulations did not contain added sugar. The starch digestibility index and rapidly available glucose of the formulations are presented in table no.4. The SDI of Pulmo-1 and DM were the lowest whereas; Rene had significantly higher SDI values. The pre-digested formula Elem had a significantly higher TS, RDS, SDS, RS and RAG values (p<0.05) than other formulations.
Table No 3: Total Starch and Starch Fractions of the Formulations
| Formulation | Pulmo-1 | Pulmo-2 | DM | Elem | Rene | Can |
| Total Starch | 26.70a± 0.84 | 35.66b± 0.63 | 34.77b± 1.78 | 52.56d± 0.43 | 28.48a± 0.32 | 40.34c± 0.68 |
| Rapidly digestible Starch | 16.04a± 0.04 | 25.94d± 0.06 | 21.38b± 1.06 | 39.03e± 0.52 | 23.45c± 0.57 | 27.20d± 0.54 |
| Slowly digestible starch | 4.39a ± 0.04 | 3.75a± 1.18 | 6.73b± 0.90 | 7.06b ± 0.63 | 3.30a± 0.77 | 6.88b± 0.31 |
| Resistant Starch | 5.91ab± 0.87 | 5.97ab± 0.88 | 6.67b±1.67 | 6.47ab± 0.71 | 1.73a± 0.07 | 6.26ab± 0.67 |
| The mean values ± SD (n=3) expressed as g/100g with the superscripts a, b, c, d, e differ significantly (p<0.05). | ||||||
Table No 4: Starch Digestibility Index and Rapidly Available Glucose Contents of the Formulations (All values are represented as mean ± SD, g/100g)
| Formulation | A 1 | B 2 | C 6 | D 4 | E 3 | F 5 |
| Pulmo-1 | Pulmo-2 | DM | Elem | Rene | Can | |
| SDI | 61.47a± 1.92 | 72.76c± 1.16 | 61.52a± 2.42 | 74.25c± 0.52 | 82.35d± 2.71 | 67.43b± 0.93 |
| RAG (g) | 26.06b± 0.61 | 37.40d± 0.25 | 24.19a± 1.23 | 44.23e± 0.38 | 26.42b± 0.61 | 30.59c± 0.61 |
| SDI – Starch Digestibility Index; RAG – Rapidly Available GlucoseThe mean values ± SD (n=3) expressed as g/100g with the superscripts a,b,c,d,e differ significantly (p<0.05). | ||||||
The proportion of digestible carbohydrate (FG+RDS+SDS) in the formulations expressed as grams and as percentage of total carbohydrates is shown in figure no.1and 2 respectively. The total digestible carbohydrate content in the formulation Pulmo-1 was found to be 24.71 ± 0.06 g/100g. When expressed as percentage of total carbohydrates, formulations Rene and Pulmo-1 had a higher proportion of available carbohydrates followed by formulation Can, Elem and Pulmo-2 and lowest availability was observed in formulation DM as recommended. The correlation between indicators of carbohydrate digestibility and fiber content is presented in table no.5. The formulations Pulmo-1 and Rene were excluded from the correlation analysis as they were devoid of dietary fiber. A strong positive correlation was observed between dietary fiber and resistant starch content. Similarly, strong negative correlation was found between dietary fiber and SDI.
In Vitro Protein Digestibility
The IVPD of the formulations and their total protein content is presented in figure no.3. The IVPD ranged between 41.42 – 96.84%, formulation Can had the highest protein digestibility followed by DM (93.34%), which was significantly higher (p<0.05) compared to other 4 formulations. All other formulations differed significantly from each other. Formulation Pulmo-1 had the least protein content as well as digestibility. Though, formulation DM had moderate protein content, the digestibility was comparable to formulation Can, which is a high protein supplement.
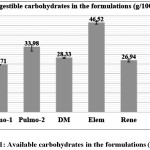 |
Figure 1: Available Carbohydrates in the Formulations (G/100g) Click here to View figure |
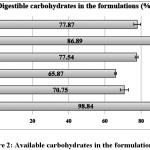 |
Figure 2: Available Carbohydrates in the Formulations (%) Click here to View figure |
Table No 5: Relation Between Dietary Fiber and Carbohydrate Digestibility
| Parameters | Vs Dietary fiber (r-value) |
| % of Digestible carbohydrates | -0.562 |
| SDI | -0.845 |
| RAG | -0.479 |
| RDS | -0.346 |
| SDS | 0.263 |
| RS | 0.750 |
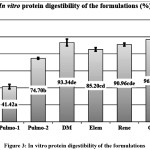 |
Figure 3: In Vitro Protein Digestibility of the Formulations Click here to View figure |
The mean values expressed as g/100g with the superscripts a, b, c, d, e differ significantly (p<0.05)
Discussion
The measurement of starch fractions in vitro provides an overview of the available and resistant carbohydrates and their rate of digestion. The fractions of available carbohydrates and their digestion kinetics are of importance in clinical nutrition and dietetics especially in the practical use of glycemic index.11 The current study provides data on the various starch fractions and their digestibility pattern in selected commercial disease specific supplements.
The results show variations in the total starch and starch fractions. The variation in the total starch content could be due to the different proportion of carbohydrates used in the formulations. From the nutritional labels of the formulations, the sources of carbohydrates used were maltodextrins, fiber from soya and guar gum and fructo-oligosaccharides. Maltodextrin was the most common ingredient used in all the formulations as a source of carbohydrates; fiber was found in formulations Pulmo-2, DM and Elem and; fructo oligosaccharides were found in formulation DM. It is interesting to note that although ‘maltodextrin’ was the common source of available carbohydrates; there were significant variations in the digestibility pattern as observed by changes in the RDS, SDS and RS fractions of the formulations.
Among the two glucose polymers found in starch molecules namely amylose and amylopectin, the latter is known to be more rapidly susceptible to the action of carbohydrate digesting enzymes.12 Dextrose equivalent (DE) of a carbohydrate defines the degree of starch hydrolysis and is an important measure that decides the application of maltodextrins. Maltodextrins are known to have DE below 20.13 Starch granules from various food sources are known to differ in their amylose to amylopectin ratio. This ratio has an impact on the digestibility of maltodextrins obtained from different native starches.7 Information on the source of maltodextrin is not mentioned in the nutrition labeling in all the formulations. Differences in the amylose content, DE and retrogradation susceptibility of maltodextrins obtained from starch of food sources such as potato, corn, wheat and rice starch has been reported.14 Thus, the difference in the digestibility of carbohydrates observed among the formulations could be due to the different source of maltodextrins used in the formulations. Substitution of starch with maltodextrins may lead to an increased glycemic load and consequently postprandial hyperglycemia, which is not desirable in the dietary management of some disease conditions.
The rate and extent of digestion of carbohydrates are also influenced by a number of other factors apart from their physicochemical properties, such as the interaction with other nutrients namely fiber, protein and fat which can impact the diffusion and adsorption of carbohydrate-hydrolyzing enzymes.15,16 The variations in the starch digestibility index values can be related to the differing proportions of fiber, protein and fat content.
RAG is a better indicator of the blood glucose and insulin response than the SDI value and is accepted as an important determinant based on its correlation with glycemic response.8 The formulation DM had the lowest RAG which is in agreement with the recommended use of the product in diabetics. Formulation DM also had the highest dietary fiber and fructooligosaccharide content. Formulation Elem had the highest RAG even with a moderate amount of protein and fat, but in a semi-elemental form. The RAG values can increase with higher processing of starch, but are also affected by the food matrix and nutrient interactions. Apart from formulations Pulmo-2 and Elem, all others had a lower RAG making them suitable for use by diabetics.
The digestibility of protein in foods is an important measure that provides an overview of the proteins available for absorption thus reflecting the protein efficiency.17 The IVPD assay simulates the normal process of digestion by the use of proteolytic enzymes. Among the formulations, Pulmo-1 containing whole and skimmed milk powder as the protein source had the least digestibility and the rest of the formulations exhibited higher digestibility. Though formulation Elem had protein in the pre-digested form, the digestibility was lesser compared to formulations DM and Can. Formulations Rene and Can not only had highest amount of protein (41g/100g and 35g/100g respectively) but also had higher digestibility, suiting their intended use. All other formulations had soy protein isolate, whey protein concentrate, hydrolyzed whey protein or sodium and calcium caseinate in combination as the protein source. Whey protein is widely used commercially owing to its higher digestibility and nutritional value than casein, primarily attributed to the higher branched-chain amino acid content.17,18 Other factors that could have altered the extent of digestibility of the various forms of protein are processing conditions, method of extraction and purification, temperature used during processing.19
The information on the functional properties of food has an important role as part of the product description/labeling by providing knowledge on the quality of the nutrients than nutritional composition alone. Bioaccessibility is defined as the amount of an ingested nutrient that is available for absorption in the gut after digestion. Variations in the accessibility and availability of a nutrient can be seen even when the same food/ingredient is used, which is therefore dependent on several factors such as chemical nature, other nutrients, complexes formed with other nutrients and the matrix of the food that is achieved by processing, which can be favorable or non-favorable.20 The effect of dietary fiber on the carbohydrate digestion and rate of absorption is well documented. Soluble dietary fiber is known to alter the physicochemical properties of the digesta by increasing the viscosity which results in reduced interactions between starch and alpha-amylase because of limited access to the substrate. Whereas, insoluble fiber is known to inhibit enzyme activity by non-specific binding resulting in decreased nutrient bioaccessibility.21 The type and degree of processing are known to significantly modify the structure of carbohydrates leading to alterations in digestibility.
The information on nutritional composition alone will not be sufficient as it does not necessarily define the nutritional attributes of the food product in terms of metabolism in the gut. Alterations in the normal gut functioning due to illness can further modify the food behavior in the gut. Thus, data on the bio-accessibility of macronutrients will be useful for food and nutrition professionals to select appropriate supplements for patients with altered physiological needs or functioning and to promote recovery. Thus, food manufacturers should consider the inclusion of data on the functional attributes of nutrient supplements along with the nutritional and safety aspectsin food labeling.
Conclusion
The results of the current in vitro study indicate variations in the digestibility of carbohydrates and proteins in the selected commercial formulations. The variations are evident even when a common source of nutrient is used as an ingredient in the formulation suggesting the influence of other physico-chemical factors which needs further research to achieve the optimum combination and state of foods used to formulate the nutrition supplements. Knowledge from detailed research can direct the food product manufacturers to design supplement or a formulation with the most suitable form and combination of nutrients to ensure maximum digestibility and overall bioavailability.
Acknowledgements
Authors thank the University Grants Commission – Special Assistance Program- Phase II (Grant no.UGC No. F 640/1/DRS/2013 (SAP-I), dated July 15, 2013) from Department of Science and Technology, Ministry of Science and Technology, New Delhi, India for providing the financial assistance to conduct the study. We also thank Ms.Kaneez Haleema and Ms. Lakshmi S, Technical assistants, UGC DRS II project at the Department for their assistance in conducting the laboratory analyses in the study.
Declaration of Interest: None
Authors Contributions
This work was carried out in collaboration between all authors. Asna Urooj designed the study, wrote the protocol and the manuscript. Chandan Vinay Srigiripura and Namratha Pai Kotebagilu performed the experiments, statistical analysis, managed literature search and wrote the first draft. All authors read and approved the final manuscript.
References
- Sobotka L., Allison S. P., Forbes A., Ljungqvist O., Meier R. F., Pertkiewicz M., and Soeters P. B. Basics in clinical nutrition. 4th. Prague, Czech Republic: Galen: 2012; 11-17.
- Volkert D., Berner Y. N., Berry E., Cederholm T., Bertrand P. C., Milne A., Palmblad J, Sobotka L, Stanga Z, Lenzen-Grossimlinghaus R., Krys U. ESPEN guidelines on enteral nutrition: geriatrics. Clinical nutrition. 2006; 25(2): 330-360.
CrossRef - Stratton R. J., and Elia M. A review of reviews: a new look at the evidence for oral nutritional supplements in clinical practice. Clinical Nutrition Supplements. 2007; 2(1), 5-23.
CrossRef - Nelms M, Sucher KP, Lacey K, Roth SL. 2011. Nutrition therapy and pathophysiology. 2nd Ed. Wadsworth: Cengage Learning; 2011:p-80.
- Cresci G. Nutrition support for the critically ill patient: a guide to practice. Boca Raton FL: CRC Press; 2015: 253-277.
CrossRef - Turgeon S.L., Rioux L.E. Food matrix impact on macronutrients nutritional properties. Food Hydrocolloids. 2011; 25(8):1915–1924.
CrossRef - Hofman D. L., Van Buul V. J., Brouns F. J. Nutrition, health, and regulatory aspects of digestible maltodextrins. Critical reviews in food science and nutrition. 2016: 56(12), 2091-2100.
CrossRef - Millward D. J., Layman D. K., Tomé D., Schaafsma G. Protein quality assessment: impact of expanding understanding of protein and amino acid needs for optimal health–. The American journal of clinical nutrition. 2008: 87(5), 1576S-1581S.
- Englyst H. N., Kingman S. M., Cummings J. H. Classification and measurement of nutritionally important starch fractions. European Journal of Clinical Nutrition. 1992; 46(2): S33-50.
- Akeson W. R., Stahmann M. A Pepsin Pancreatin Digest Index of Protein Quality Evaluation. The Journal of Nutrition. 1964; 83: 257–261.
CrossRef - Englyst K. N., Englyst H. N., Hudson G. J., Cole T. J., Cummings J. H. Rapidly available glucose in foods: An in vitro measurement that reflects the glycemic response. American Journal of Clinical Nutrition.1999; 69(3): 448–454.
CrossRef - Topping D.L., Gooden J.M., Brown I. L., Biebrick D.A., McGrath L., Trimble R.P., Choct M., Illman R. J. A high amylose (amylomaize) starch raises proximal large bowel starch and increases colon length in pigs. Journal of Nutrition. 1997: 127: 615–622.
CrossRef - Sun J., Zhao R., Zeng J., Li G., Li, X. Characterization of dextrins with different dextrose equivalents. Molecules. 2010: 15(8), 5162-5173.
CrossRef - Sobolewska-Zielińska J., Fortuna, T. Retrogradation of starches and maltodextrins of various origin. Acta Scientiarum Polonorum Technologia Alimentaria. 2010; 9(1): 71-81.
- Englyst K. N., Liu S., Englyst H. N. Nutritional characterization and measurement of dietary carbohydrates. European Journal of Clinical Nutrition. 2007; 61: S19–S39.
CrossRef - Salar R. K., Gahlawat S. K., Siwach P., and Duhan J. S. (Eds.). Biotechnology: prospects and applications. New Delhi: Springer; 2013: 39-52.
CrossRef - Almeida C. C., Monteiro M. L. G., Costa-Lima B. R. C. D., Alvares T. S., Conte-Junior C. A. In vitro digestibility of commercial whey protein supplements. LWT – Food Science and Technology. 2015; 61(1): 7-11.
CrossRef - Shrestha A. K. Scientific Background of Dairy Protein Digestibility: A Review. Journal of Food Science and Technology Nepal. 2014; 7: 1-8.
CrossRef - Onwulata C. I., Konstance R. P., Tomasula P. M. Minimizing variations in functionality of whey protein concentrates from different sources. Journal of dairy science. 2004; 87(3): 749-756.
CrossRef - Parada J., Aguilera J. M. Food microstructure affects the bioavailability of several nutrients. Journal of Food Science. 2007; 72(2): R21-R32.
CrossRef - Grundy M. M. L., Edwards C. H., Mackie A. R., Gidley M. J., Butterworth P. J., Ellis P. R. Re-evaluation of the mechanisms of dietary fibre and implications for macronutrient bioaccessibility, digestion and postprandial metabolism. British Journal of Nutrition. 2016; 116(5): 816-833.
CrossRef
Accepted on: 26-01-2019
Second Review by: Dr. Ajay Singh India
Final Approval by: Prof. Min-Hsiung Pan





Web of Science Coverage
Emerging Sources Citation Index (ESCI)
2024 Journal Impact Factor: 1.1
Scopus Journal Metrics
CiteScore 2025: 2.6
CiteScore Details
Sustainable Nutrition: Food Systems, Nutrient Retention, and Public Health Impact
![]()
This journal is a member of, and subscribes to the principles of, the Committee on Publication Ethics (COPE)








