Knowledge and Practices Regarding Infant and Young Child Feeding among Mothers Working in Readymade Garments Sector in Bangladesh: A Cross-Sectional Survey

1International Centre for Diarrheal Disease Research, Dhaka, Bangladesh.
2BRAC James P. Grant School of Public Health, BRAC University, Dhaka, Bangladesh.
Corresponding Author Email: afrin.iqbal@icddrb.org
DOI : http://dx.doi.org/10.12944/CRNFSJ.9.1.19
Download this article as:
![]()
Optimum is. Adequate Infant and young child feeding (IYCF), critical for child’s growth and development, requires a significant amount of time andcan be challenging for working mothers. In Bangladesh, about four million women work long-hours in Readymade Garment (RMG) factories without proper maternity benefits which raises concern regarding optimum IYCF practice. We conducted a descriptive cross-sectional study in Dhaka, Bangladesh to identify the knowledge and common practices of IYCF among mothers working in Readymade Garment sector. Ninety-three women of reproductive age (15-49 years), working in Readymade Garment sector, with children aged 6-23 months, were interviewed. Our study revealed- majority knew about exclusive breast feeding (EBF) (76%), duration to continue breast feeding (73%) and early initiation of breast feeding (53%). The exclusive breast-feeding practice in mothers employed in RMG sector was 44%. Three-fourths of the mothers knew and initiated complementary feeding timely. Both knowledge regarding age-adjusted minimum meal frequency (MMF) (19.4%) and minimum quantity (8.6%) were low; compared to actual practices. Nearly two-fifth of the mothers (40%) had to start working before their child reached six months of age enabling them to provide their baby with breastmilk substitutes. Mothers employed in Readymade Garment sector had better IYCF practice than general population. Proper workplace environment with mandatory breast-feeding corners, daycare facilities and ensuring maternity benefits in these mothers could help achieve an even better IYCF practices for their children.
KEYWORDS:Bangladesh; Child Nutrition; Complementary Feeding; Infant and Young Child Feeding (IYCF); Readymade Garment (RMG); Working Women
Introduction
Appropriate infant and young child feeding (IYCF) is critical for growth, and development, and for early prevention of chronic degenerative diseases (1-4). Children under two years are at risk of nutritional deficiency and growth retardation due to inadequate breast feeding and poor complementary feeding practices (1-4). United Nations Standing Committee on Nutrition estimated that exclusive breast feeding (EBF) for the first six months of life could reduce infant deaths by 13% and adequate nutritious complementary feeding could reduce all under five deaths by 6% (5). Considering the immense importance of IYCF, current recommendation by the World Health Organization (WHO) for IYCF includes exclusive breast feeding of every child below six months of age with initiation of breast feeding within first hour of birth (6). It is also advised for adequate, nutritious, safe complementary food with continuation of breast feeding from six months up to two years of age (7).
South Asian countries including Bangladesh lag behind in the implementation of appropriate IYCF practices specifically complementary feeding (8-14). For both breast feeding and complementary feeding, mother’s knowledge and time investment are crucial. Healthy and adequate complementary feeding, along with quality time spent with mother, leads to positive health outcome of the child (15). With more women entering the job market than ever before (16), concerns arise regarding mother’s time for child care and IYCF. In Bangladesh, the number of working women increased from 1.5 million in 2004 to 4 million in recent years with approximately 40-50% married working mothers; majority working in Readymade Garment (RMG) sectors (17-19). RMG workers with inadequate or lack of on-site feeding locations, short maternity leaves and long working hours may not have the optimum environment for adequate IYCF (20-22).
Several studies have looked at different IYCF indicators in general population. However, very few studies segregated the IYCF knowledge and/ or practice by working/ non-working mother and among the mothers employed in the RMG sectors. Therefore, no information is available on IYCF practices of garment working mothers and reasons behind their practices. This study measures the IYCF related knowledge and practices among mothers working in RMG sector in Dhaka city. In addition, upon identifying poor IYCF practices among the garment working mothers, the study further explores the reasons behind their inadequate practice. The evidence generated from this study is therefore critical to design appropriate interventions for working mothers in relevance to changes in working hours, establishment of quality day care centers and alteration of maternity benefit policies within the RMG factories.
Methods
Study Design
A cross sectional study was conducted to explore the IYCF knowledge and practices among nursing mothers working in RMG factories in Dhaka City, Bangladesh. A preliminary document review of existing garment factories in the city was conducted with information support from Bangladesh Garment Manufacturers and Exporters Association (BGMEA) and 19 factories were selected based on their volume of female workers, geographical location and accessibility and willingness to participate in the study. Three of them were large factories with more than 3000 workers and rest were small factories with less than 1000 workers. The study respondents were female garment workers who were ever married and had a child aged 6 to 23 months during the study period. Any women having a child with a mental or physical illness or disability such as cleft palate, gastrointestinal anomaly etc. which could interfere with normal feeding practices was excluded from the study.
Considering the prevalence of three- recommended IYCF practices (breast milk/milk/milk products, minimum dietary diversity and minimum meal frequency) among women living in urban areas at 28%, we calculated a sample size of 98 women with 5% non-response rate, 0.10 margin of error, 95% confidence interval, and design effect at 1.2. A list of eligible women meeting the selection criteria of the study was difficult to collect from the human resource office or managers of the selected garment factories; hence, the women were interviewed based on ease of access and convenience. In total 93 women were interviewed during the period of November 2013 to January 2014.
Collection of Data
Data collection was carried out by trained interviewers using a standardized pre-tested semi-structured questionnaire in Bangla. The questionnaire was pre-tested in an informal urban settlement (slum) among five garment workers. The consistency of the questionnaire, appropriateness of the language, sequencing of the questions was tested, and necessary modifications were made. The questionnaire was implemented; face-to-face by the research investigator and a trained field research assistant. The questionnaire took approximately 30 to 35 minutes to complete. The interviews were taken in their workplace at their convenient time. Since the study did not provide any compensation to the garment workers for their time spent for interviews, they were interviewed only after receiving permission from their work supervisors after explaining the purpose and nature of data collection. Data were collected on socio-demographic characteristics, knowledge and practice regarding IYCF and reasons behind poor IYCF practices among the women.
The variables included are categorized into four types; child’s characteristics, mothers characteristics, household characteristics, and health care seeking practices. The child’s characteristics include- child’s age (in months), sex, birth order and place of childcare. Birth order of the last-born child was categorized into – ‘first’ and ‘second or more’. Place of childcare was categorized into home and daycare. The mother’s characteristics include- education and working hours. Mother’s education was categorized into no education and some education. Household characteristics included- household savings which was categorized into ‘no savings’ and ‘some savings’. The health care seeking practices include- antenatal care (ANC), delivery place and postnatal care (PNC). Number of ANC visits was recorded as a continuous variable and categorized into ‘no ANC’ ‘less than four’ and ‘four or more’. Delivery place was categorized into- ‘health facility’ or ‘home’. PNC with a health care provider was recoded into two categories- ‘no PNC’ or ‘any PNC’.
IYCF knowledge was measured by seven questions relating to breast feeding and complementary feeding (table 1). Each correct answer was scored as ‘1’ and every incorrect answer was scored ‘0 (zero)’. The total score for knowledge ranged from 0 to 7.
The questions are listed in the table below-
Table 1: Breast Feeding and Complementary Feeding Knowledge Questions.
| Sl. | Knowledge Questions |
| Questions related to breast feeding | |
| 1. | Do you know – when to start breast feeding after birth? |
| 2. | For how long you are supposed to exclusively breast feed your child? |
| 3. | For how many years you can continue breast feeding your child? |
| Questions related to complementary feeding | |
| 4. | Do you know the appropriate age to introduce complementary food? |
| 5. | The minimum number of times your child should be fed in a day (MMF)? |
| 6. | How many food groups your child should eat from (MDD)? Or, what types of food you should give your child? |
| 7. | The minimum amount of food you should give your child in every feed (quantity)? |
To determine the status of IYCF practices, both breast feeding and complementary feeding practices were examined. Five core indicators and one optional indicator were selected out of the eight core indicators and seven optional indicators as suggested by the WHO (23). The indicators were selected based on local context and custom.
Breast feeding practices included: initiation of breast feeding within the first hour of life, duration of exclusive breast feeding; and whether or not the mother was breast feeding at the time of interview. For complementary feeding practices, mothers were inquired about: Initiation of complementary food at appropriate age, being fed from four or more food groups- minimum dietary diversity (MDD), being fed semi-solid/solid foods, a minimum number of times per day according to age- minimum meal frequency (MMF); being fed appropriate quantity at each feed according to age (quantity).
After each practice question, one open ended question was asked to the mothers to find the reasons behind a certain practice that they were not performing at the time of interview.
Data was analyzed using Stata (ver. 13.0). Descriptive statistics was used to analyze the knowledge and practices regarding IYCF. Univariate analysis was carried out using frequencies, percentages, mean and standard deviation. Bivariate analysis was carried out by Chi-square test and Fisher’s exact test to determine statistically significant associations for categorical variables.
Ethical Considerations
The study had ethical approval from the Ethical Review Committee of James P Grant School of Public Health, BRAC University. Informed written consent was obtained from respondents before conducting the interviews after explaining the nature and purpose of the study. Each respondent were made aware of any potential risk and regarding benefits of participating in the study. It was also made clear that study participation is completely voluntary and the participant may wish to withdraw at any moment. Privacy and information confidentiality of the study participants were strictly maintained throughout the study period and no information obtained from the interviews was shared with work supervisors or colleagues of the garment workers.
Results
Background Characteristics
A total of 93 mothers aged 17 to 30 years were interviewed (Table 2). The majority (95%) of mothers were currently married and living with their husbands. The median number of household members was 4 (Interquartile range: 3-5), mothers worked 9 (Interquartile range: 8-11) hours per day and more than half (57%) of them worked more than eight hours per day. More than a third of the mothers had completed primary level education. Most (88%) mothers had at least one ANC visit, one-third delivered their child at home and 68% did not have any PNC. Two thirds of the children were first born and were older than one year of age at the time of interview. While the mothers worked, the children were looked after by their grandmothers (57%), other family members (17%), or maids/ neighbors (26%). Among the 19 garment factories, five of the factories had a full functioning daycare center with two to three caretakers. However, only 13 mothers of the 57 who had access to the daycare center used it for childcare.
Knowledge and Practice Regarding Breast Feeding
Table 3 depicts the knowledge and practices related to breast feeding. More than half (53%; [43.9 to 63.4]) of the mothers were aware that breast feeding should be initiated within an hour of delivery and 56% (46.1 to 66.4) of the mothers did so. Though not statistically significant, with mother’s education and household savings, the knowledge on initiation of breast feeding increased, practice however, though increased with household savings, decreased in educated mothers.
Table 2: Characteristics of Women and their Children.
| Variables | % (n) or Mean ± SD or Median (Interquartile Range) |
| Children (n=93) | |
| Female | 47 (44) |
| Age (months) | 16 ± 5.3 |
| Birth order | |
| 1st born | 73 (68) |
| 2nd or 3rd born | 27 (25) |
| Mother (n=93) | |
| Age (years) (Mean ± SD) | 23 ± 2.8 |
| Education | |
| No education | 14 (15) |
| Primary Incomplete | 12.9 (12) |
| Primary Complete | 39.8 (37) |
| Secondary Incomplete | 24.7 (23) |
| Secondary Complete | 7.5 (7) |
| Mother’s work | |
| Hours per day | 9 (8-11) |
| Days per week | 6 ± 0.2 |
| Income per month (USD) | 67 ±22 |
| Job duration (years) | 4 (1.5-7) |
| Reproductive Health and Delivery Practices | |
| Place of delivery | |
| Home | 62 (58) |
| Healthcare facility | 38 (35) |
| Antenatal care: number of visits | |
| None | 13 (12) |
| 1 to 2 visits | 37 (34) |
| 3 or more visits | 51 (47) |
| Postnatal care: number of visits | |
| None | 68 (63) |
| 1 or more visits | 32 (30) |
| Household Characteristics | |
| Family size | 4 (3-5) |
| HH income/ month (USD) | 160 ±65.4 |
| HH savings/month (USD) | 19.3 ±12.4 |
Table 3: Breastfeeding Knowledge and Practice by Background Characteristics.
| Initiation of BF within the 1st Hour of Life | Duration of EBF for 1st 6 Months of Life | Overall duration of BF for 2years or More | 6-23 M Child (N) | ||||
| Know | Prac | Know | Prac | Know | Prac | ||
| Child age in months | |||||||
| 6-11 | 54.5 | 63.6 | 81.8 | 36.4 | 77.3 | 86.4 | 22 |
| 12-23 | 53.5 | 54.3 | 74.6 | 46.5 | 64.8 | 64.8 | 71 |
| Sex | |||||||
| Female | 54.5 | 50 | 72.7 | 47.7 | 68.2 | 72.7 | 44 |
| Male | 53.1 | 62.5 | 79.6 | 40.8 | 67.3 | 66.7 | 49 |
| Childcare | |||||||
| Daycare | 23 | 53.8 | 76.9 | 61.5 | 61.568.8 (55) | 84.6 | 13 |
| Home | 58.8 | 57 | 76.3 | 41.3 | 68.8 | 67.1 | 80 |
| Birth order | |||||||
| 1st | 54.4 | 55.2 | 76.5 | 39.7 | 67.6 | 68.7 | 68 |
| 2nd or more | 52 | 60 | 76.0 | 56 | 68 | 72 | 25 |
| Mothers education | |||||||
| None | 50 | 71.4 | 78.6 | 42.9 | 64.3* | 78.6 | 14 |
| Some | 54.4 | 53.8 | 75.9 | 44.3 | 68.4 * | 67.9 | 79 |
| Working hours | |||||||
| 8 or less | 57.550.9 (27) | 56.4 | 80 | 57.5 * | 52.5 | 59 * | 40 |
| > 8 | 50.9 | 56.6 | 73.6 | 34 * | 79.2 | 77.4 * | 53 |
| HH savings | |||||||
| No savings | 47.4 | 51.8 | 73.7 | 45.6 | 66.7 | 62.5 * | 57 |
| Some savings | 63.9 | 63.9 | 80.6 | 41.7 | 69.4 | 80.6 * | 36 |
| Delivery place | |||||||
| Home | 55.2 | 60.3 | 74.1 | 41.4 | 56.9 | 58.6 * | 58 |
| Health Facility | 51.4 | 50 | 80 | 48.6 | 85.7 | 88.2 * | 35 |
| ANC visits | |||||||
| No visit | 33.3 | 66.7 | 75 | 41.7 | 41.7 | 50 | 12 |
| <4 | 61.8 | 69.7 | 73.5 | 50 | 67.6 | 78.8 | 34 |
| ≥4 | 53.2 | 44.7 | 78.7 | 40.4 | 74.5 | 68.1 | 47 |
| PNC visits | |||||||
| No visit | 52.4 | 58.1 | 71.4 | 49.2 | 61.9 | 71 | 63 |
| ≥1 | 56.7 | 53.3 | 86.7 | 33.3 | 80 | 66.7 | 30 |
| TOTAL[95% CI] | 53.3*(43.9-63.4) | 56.5(46.1-66.4) | 76.3(66.5-84.0) | 44.1(34.2-54.5) | 67.4*(64.2-82.2) | 73.1*(63.1- 81.3) | 93 |
*<0.05; HH, household; ANC, ante-natal care; PNC, post-natal care; BF, breast feeding; EBF
*Know= Knowledge, Prac= Practice
Approximately 76% (66.5 to 84.0) of the mothers knew that babies should be exclusively breast fed till six months of age with only four out of 10 [44% (34.2 to 54.5]) practicing exclusive breast feeding. More mothers with younger and male child, working less than 8 hours, with some savings, who delivered in a facility and had at least one PNC visit knew about the duration of exclusive breast feeding correctly. More mothers who kept their children in daycare facility, worked less than 8 hours and delivered in a healthcare facility exclusively breast fed their children till 6 months.
More than two-thirds (67%; [64.2 to 82.2]) of the women knew that breast feeding should ideally be continued for two years or more and 73% (63.1 to 81.3) women were still breast feeding their child. There was significant difference (P<0.05) in knowledge of duration of breast feeding between uneducated and educated women with more educated women having proper knowledge. Women having some savings and facility delivery had better practice regarding still breast feeding their child and it was statistically significant (P<0.05).
Knowledge and Practice Regarding Complementary Feeding
The knowledge and practices related to complementary feeding is depicted in table 4. The majority knew the appropriate age of initiation (74%; [64.2 to 82.2]) and diversity required for complementary feeding (87%; [78.5 to 92.6]) (Table 4). However, few women knew the minimum number of meals per day (19%; [12.4 to 28.8]) or the quantity of food according to age of the child (9%; [4.3 to 16.5]) that their child should be fed. Most mothers also practiced appropriate initiation of complementary feeding (73%; [63.0 to 81.3]) and minimum dietary diversity. Contrary to lack of knowledge on meal frequency, more than half (53%; [42.4 to 62.6]) of the mothers had accurate practice. Approximately a quarter (24%; [15.9 to 35.5]) of the children were fed appropriate quantity according to age.
Table 4: Complementary Feeding Knowledge and Practice by Background Characteristics.
| Initiation of CF after the end of the 6th month | Minimum dietary diversity (MDD) | Minimum times or more (MMF) | Minimum quantity to be fed | 6-23 M child (N) | |||||
| Know | Prac | Know | Prac | Know | Prac | Know | Prac | ||
| Child age in months | |||||||||
| 6-11 | 72.7 | 59.1 | 77.3 | 45.5 | 18.2 | 45.5 | 4.5 | 40.9 | 22 |
| 12-23 | 74.6 | 77.5 | 90.1 | 77.5 | 19.7 | 54.9 | 9.9 | 18.3 | 71 |
| Sex | |||||||||
| Female | 70.5 | 72.7 | 88.6 | 68.2 | 18.2 | 50.0 | 4.5 | 29.5 | 44 |
| Male | 77.6 | 73.5 | 85.7 | 71.4 | 20.4 | 55.0 | 12.2 | 18.4 | 49 |
| Childcare | |||||||||
| Daycare | 92.3 | 76.9 | 84.6 | 53.8 | 15.4 | 61.5 | 7.7 | 23.1 | 13 |
| Home | 71.3 | 72.5 | 87.5 | 72.5 | 20 | 51.2 | 8.8 | 23.8 | 73 |
| Birth order | |||||||||
| 1st | 79.4 | 73.5 | 86.8 | 67.6 | 20.6 | 50.0* | 5.9 | 22.1 | 68 |
| 2nd or more | 60.0 | 72.0 | 88.0 | 76.0 | 16.0 | 60.0* | 16 | 28 | 25 |
| Mothers education | |||||||||
| None | 50* | 57.1 | 85.7 | 42.9 | 0.0* | 50 | 14.3 | 35.7 | 14 |
| some | 78.5 * | 75.9 | 87.3 | 74.7 | 22.8 * | 53.2 | 7.6 | 21.5 | 79 |
| Working hours | |||||||||
| 8 or less | 80.0 | 85.0 | 90.0 | 75.0 | 25.0 | 50.0 | 5.0 | 17.5 | 40 |
| > 8 | 69.8 | 64.2 | 84.9 | 66 | 15.1 | 54.7 | 11.3 | 28.3 | 53 |
| HH savings | |||||||||
| No savings | 66.7 | 71.9 | 84.2 | 73.7 | 24.6 (14) | 47.4 | 7.0 | 26.3 (15)* | 57 |
| Some savings | 86.1 | 75 | 91.7 | 63.9 | 11.1 | 61.1 | 11.1 | 19.4 (7)* | 36 |
| Delivery place | |||||||||
| Home | 63.8 | 72.4 | 87.9 | 75.9 | 20.7 (12) | 50 | 8.6 | 29.3 (17) | 58 |
| Health Facility | 91.4 | 74.3 | 85.7 | 60.0 | 17.1 | 57.1 | 8.6 | 14.3 | 35 |
| ANC visits | |||||||||
| No ANC | 33.3* | 50.0 | 75.0 | 58.3 | 25.0 | 50.0 | 0.0 | 8.3 | 12 |
| <4 | 85.3 * | 76.5 | 88.2 | 61.8 | 17.6 | 38.2 | 5.9 | 20.6 | 34 |
| ≥4 | 76.6 * | 76.6 | 89.4 | 78.7 | 19.1 | 63.8 | 12.8 | 29.8 | 47 |
| PNC visits | |||||||||
| No PNC | 71.4 | 77.8 | 84.1 | 68.3 | 20.6 | 52.4 | 9.5 | 20.6 | 63 |
| Any PNC | 80.0 | 63.3 | 93.3 | 73.3 | 16.7 | 53.3 | 6.7 | 30 | 30 |
| TOTAL[95% CI] | 74.2*(64.2-82.2) | 73.1*(63.0- 81.3) | 87.1*(78.5-92.6) | 69.9*(59.7- 78.5) | 19.4(12.4-28.8) | 52.7(42.4- 62.6) | 8.6*(4.3- 16.5) | 23.7 *(15.9-35.5) | 93 |
*<0.05; HH, household; ANC, ante-natal care; PNC, post-natal care; CF, complementary feeding
Mothers with older child, working less than 8 hours, some household savings and more ANC, PNC visits had correct knowledge on dietary diversity. Dietary diversity practice was accurate in educated mothers having older male children, who kept the child at home during work, worked less than eight hours, had more ANC and PNC check-ups. More educated women knew regarding minimum meal frequency and appropriate practice increased with birth order of the child (P<0.05). The practice of appropriate quantity to be fed was higher in women having more ANC, PNC visits.
Overall, practice of feeding from diverse food groups despite knowing about them was low and difference was statistically significant (P<0.005). But more mothers had better practice of minimum quantity of feeding compared to relevant knowledge (P<0.005).
Fig 1 depicts the proportion of IYCF practices among the mothers who had the appropriate knowledge. In contrast to breast feeding practices, 67% of the mothers initiated breast feeding within an hour despite of knowing correct time of initiation (P<0.005). Less than half of the mothers exclusively breast fed their children till six months of age. Regarding complementary feeding, majority but not all had appropriate practice of initiation of complementary feeding at the end of the 6th month, minimum dietary diversity and minimum quantity to be fed (P<0.005). The practice of feeding the child minimum times was low even among the mothers who knew about it.
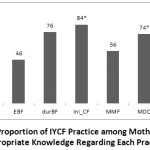 |
Figure 1: Proportion of IYCF Practice among Mothers having Appropriate Knowledge Regarding Each Practice. |
IYCF Practices and Reasons Behind Them
Forty four percent of mothers did not initiate breast feeding within the first hour of delivery; the major reason being that the mother was too unwell to feed. In addition, 37 infants were pre-lacteal fed within the first three days of birth; the reasons given were that the mother was too unwell to breast feed or they perceived that their breast milk was insufficient. The perception of insufficient breast milk was the major cause of early introduction of other liquids and complementary food. Two major reasons of a child not being exclusively breast fed were- mother’s perception of insufficient breast milk and early termination of maternity leave. Approximately half of the mothers perceived that their breast milk was insufficient and approximately 40% of the mothers had to start working before their child reached the age of six months, forcing them to introduce other milk, infant formulae or even solid or semi-solid food.
The major reasons behind not being fed the appropriate quantity according to age and not being fed from diverse food groups were reported to be lack of knowledge, child’s unwillingness to eat and not being able to afford adequately. Approximately 45 % of mothers bottle fed their child the preceding day and 60 % of the babies had snacks in between their meals and these snacks were frequently high fat and high sugar foods like chips, biscuits and candy.
Discussion
This cross sectional study explored the knowledge and practices related to IYCF among women working in RMG sector who had a children aged 6-23 months in Dhaka, Bangladesh. This study revealed that breast feeding knowledge and practices were better than complementary feeding knowledge and practices except exclusive breast feeding practices among the mothers working in RMG sector. Among the seven indicators that were focused in this study, both knowledge and practice regarding age adjusted minimum meal frequency and minimum quantity to be fed were low; knowledge being lower than the actual practices.
Despite socio-economic challenges and work barrier, mothers in RMG industry followed proper feeding practices for their children. In the current study, the knowledge and practice regarding initiation of complementary feeding and minimum dietary diversity were better than national averages. Seventy percent of the children were fed from minimum number of food groups (four or more) which was higher compared to the national coverage of minimum dietary diversity in urban areas (34%) (24). Dietary diversity depends on availability and accessibility of variety of nutritious foods (12, 25). Our study participants, residing in urban setting and being employed, were enabled to avail and access nutritious food for their families and children (21, 26-28). Additionally, greater mobility facilitated them to access information on better nutritional practices (29, 30).
However, the knowledge and practices regarding minimum times to be fed and minimum quantity to be fed in each feed was poor among the study participants. Both practices were related to the age of the child and this could be one area of focus where customization of counseling interventions for mother’s knowledge on age appropriate nutritional need of the child can be introduced. Valid and proven platforms for any counseling interventions are ante natal visits, facility delivery and post-natal visits. During these contact with healthcare providers mothers are usually more receptive towards behavior change communications (31). Surprisingly, the practices of minimum meal frequency and minimum quantity were better than relevant knowledge. This could be due to responsive feeding given to the child whenever the child cried (32). Also, contribution of secondary caregivers in complementary feeding of children of working mother is crucial (33) and may have played a role in better practice than knowledge. However, we could not explore the complementary feeding practice of secondary caregivers in this study despite believing that further exploration of these practices can be beneficial for child nutrition. While adequate complementary feeding practices may be ensured by targeted intervention to the secondary caregivers for the children of the working mothers; ensuring proper breast feeding still heavily rely on the mothers.
Breast feeding practice is universal in Bangladesh. Although three-quarter of the mothers knew about duration of exclusive breast feeding, the proportion of mothers who exclusively breast fed their child was only 44%. Having accurate knowledge may not always be translated into adequate practice which is evident from other studies in the neighboring countries with similar findings. A recent study conducted in Ahmedabad revealed 96% had correct knowledge about the duration of exclusive breast feeding but 68% practiced it (34). Even the national proportion of accurate practice of EBF, which has declined in recent days (64% in 2011 to 55% in 2014) is higher than our study findings (24, 35).
The reasons behind low exclusive breast feeding practice is multifaceted. Most of the women working in garment factories reported that their maternity leave ended within three months of their child’s birth. Similarly, other studies also found that mothers commonly introduce breast milk substitute (BMS) and/ or sometimes even solid or semisolid food to their child at the age of three months (36, 37). A recent survey done in RMG sector of Bangladesh suggests that two-thirds of the female garments workers join prematurely before completion of maternity leave as per Bangladesh Labour Law, 2006 (38-40). Even though, the Government of Bangladesh has declared six months paid maternity leave for public sector, women working in the RMG sector are deprived of their basic right and almost half of them are denied of any maternity leave (39). Further context analysis showed that on many occasion, garments worker have to take leave without pay after childbirth (41, 42) which force them to rejoin at their earliest and work extra hours to meet their family needs. Working extra hours has negative implications on breast feeding practices (43).
Significant association was found with working hours and practice of EBF in this study, consistent with other findings. Among working mothers, who kept their children in daycare, had higher prevalence of exclusive breast feeding than their counterparts. Longer working hour in absence of day care facilities in the workplace compel the mothers to start breast milk substitute or even semi solid/ solid food. The lesser a child is exclusively breast fed, the more s/he gets dependent on other unwanted alternatives, i.e.- breast milk substitute and semi-solid/ solid food. Dependence of the child on other alternatives, results in decreased breast milk production; as breast milk production requires adequate suckling stimuli by her child (44). Decreased breast milk production, again, may lead to perception of insufficient breast milk by the mothers giving rise to a vicious cycle resulting in difficulty for the mothers to continue breast feeding. Mother’s perception of insufficient breast milk was another barrier to exclusive breast feeding and continued breast feeding till two years of age consistent with other findings (45-46). We found that, one third of the children of 6-23 months were not breast fed which was 6.5% nationally in this age group (24). In order to improve this situation, baby friendly work place initiative could be one way for supporting working mothers to continue exclusive breast feeding. Feeding expressed breast milk during the office hour could be another solution.
Conclusion
Recommendations
Proper practice related to IYCF emphasizing age adjusted complementary feeding practices should be communicated though nutrition counselors during each contact with every expecting mother and new mother during ante natal visits, delivery and post-natal visits. The counseling will be translated into appropriate practice if mothers have a working environment facilitating the IYCF practices. The baby friendly workplace initiative can play a pivotal role to improve IYCF practices at workplaces. Apart from workplace, while the children are at home, the role and impact of secondary caregiver on IYCF practice during the first two years of life should be explored.
The need for a paid six months maternity leave should be communicated with the Bangladesh Garment Manufacturing Export association (BGMEA) authority stating the immense importance of exclusive breast feeding. The statement should further be enforced through rigorous monitoring by relevant implementing authorities, so that paid maternity leave is practiced by all mothers according to Bangladesh Labour Code (amendment) 2013 (40).
Limitations
There were some limitations in this study that need to be considered when interpreting the findings.
Selection of the study participants could not be done in a random manner and were conveniently selected as there was resistance and reluctance from the factory owners to provide a full list of all the workers, from which random sampling of all the working mothers meeting our eligibility criteria could be done.
The findings were based on self-reported maternal IYCF practices and may therefore differ from actual practices. In addition, we did not observe the practices and also did not include secondary caregivers who fed the children in absence of the mother. The study included mothers who had children aged 6-23 months and therefore the results may not reflect the knowledge and practices of all women working in the RMG sector. However, given the consistency of findings, we are confident that the findings represent actual practices and are representative of IYCF practices of women working in RMG sector who have children of 6-23 months.
Acknowledgements
The authors would like to thank the Maternal and Child Health Division and the Nutrition and Clinical Services Division of icddr,b for their continuous cooperation. We also are grateful to the largest contributors in this research process- the respondents who provided their invaluable time out of their busy schedule for the interviews.
Funding Source
James P Grant School of Public Health, BRAC University funded the study.
Ethical Review Committee (ERC) at the BRAC James P Grant School of Public Health, BRAC University has approved the ethical review and issued the ID 2013-MPH-ERC13-002.
Conflict of Interests
The author declares that there is no competing interest.
References
- Shrimpton R. Victora C.G., de Onis M., Lima R.C., Blossner M., Clugston G. Worldwide timing of growth faltering: implications for nutritional interventions. Pediatrics. 2001;107(5):E75.
CrossRef - Black R.E., Allen L.H., Bhutta Z.A., Caulfield L.E., de Onis M., Ezzati M., et al. Maternal and child undernutrition: global and regional exposures and health consequences. Lancet. 2008;371(9608):243-60.
CrossRef - SESSION 1, The importance of infant and young child feeding and recommended practices. Infant and young child feeding: model chapter for textbooks for medical students and allied health professionals. Geneva: World Health Organization (WHO); 2009.
- Programming Guide: Infant and Young Child Feeding 2011. Available from: UNICEF https://www.unicef.org/nutrition/files/Final_IYCF_programming_guide_2011.pdf.
- Meeting the challenges to improve complementary feeding. SCN News. 2003.
- WHO, UNICEF. Global strategy for infant and young child feeding. Geneva: World Health Organization (WHO); 2003.
- Daelmans B., Dewey K., Arimond M., Working Group on I., Young Child Feeding I. New and updated indicators for assessing infant and young child feeding. Food Nutr Bull. 2009;30(2 Suppl):S256-62.
CrossRef - Complementary feeding: report of the global consultation, and summary of guiding principles for complementary feeding of the breastfed child. Geneva, World Health Organization 2003. Report No.: 924154614X.
- Kimmons J.E., Dewey K.G., Haque E., Chakraborty J., Osendarp S.J., Brown K.H. Low nutrient intakes among infants in rural Bangladesh are attributable to low intake and micronutrient density of complementary foods. J Nutr. 2005;135(3):444-51.
CrossRef - Dibley M.J., Roy S.K., Senarath U., Patel A., Tiwari K., Agho K.E., et al. Across-country comparisons of selected infant and young child feeding indicators and associated factors in four South Asian countries. Food Nutr Bull. 2010;31(2):366-75.
CrossRef - Gulati J.K. Child Malnutrition: Trends and Issues. The Anthropologist. 2010;12(2):131-40.
CrossRef - Rasheed S., Haider R., Hassan N., Pachon H., Islam S., Jalal C.S., et al. Why does nutrition deteriorate rapidly among children under 2 years of age? Using qualitative methods to understand community perspectives on complementary feeding practices in Bangladesh. Food Nutr Bull. 2011;32(3):192-200.
CrossRef - Hanif H.M. Trends in infant and young child feeding practices in Bangladesh, 1993-2011. International breastfeeding journal. 2013;8(1):10.
CrossRef - Saleh F., Ara F., Hoque M.A., Alam M.S. Complementary Feeding Practices among Mothers in Selected Slums of Dhaka City: A Descriptive Study. Journal of Health, Population, and Nutrition. 2014;32(1):89-96.
- Patel A., Pusdekar Y., Badhoniya N., Borkar J., Agho K.E., Dibley M.J. Determinants of inappropriate complementary feeding practices in young children in India: secondary analysis of National Family Health Survey 2005-2006. Matern Child Nutr. 2012;8 Suppl 1:28-44.
CrossRef - Bureau of Labour Statistics. Women in the Labor Force. U.S. Bureau of Labor Statistics, Statistics DoLF; 2009.
- Kabeer N. Globalization, labor standards, and women’s rights: dilemmas of collective (in)action in an interdependent world. Feminist Economics. 2004;10(1):3-35.
CrossRef - Mirdha R. Bangladesh remains the second biggest apparel exporter. The Daily Star. 2018.
- The Bangladesh Garment Manufacturers and Exporters Association. RGM membership & empoyment status in Bangladesh. BGMEA; 2018.
- Absar S.S. Problems surrounding wages: the ready made garments sector in Bangladesh. Labour and Management in Development Journal. 2001;2(7):1-17.
- Khosla N. The ready-made garments industry in Bangladesh: A means to reducing gender-based social exclusion of women? J Journal of International Women’s Studies. 2009;11(1):289-303.
- Balogun O.O., Dagvadorj A., Anigo K.M., Ota E., Sasaki S. Factors influencing breastfeeding exclusivity during the first 6 months of life in developing countries: a quantitative and qualitative systematic review. Matern Child Nutr. 2015;11(4):433-51.
CrossRef - Indicators for assessing infant and young child feeding practices. Geneva,: World Health Organization (WHO); 2008 6–8 November 2007.
- National Institute of Population Research and Training (NIPORT). Bangladesh Demographic and Health Survey. The DHS Program, Ministry of Health and Family Welfare GoB; 2014 March 2016. Report No.: FR311.
- Ahmed A.M., Ahmed T., Roy S.K., Alam N., Hossain M.I. Determinants of undernutrition in children under 2 years of age from rural Bangladesh. Indian Pediatr. 2012;49(10):821-4.
CrossRef - Ruel M.T. Is dietary diversity an indicator of food security or dietary quality? A review of measurement issues and research needs. Food Nutr Bull. 2003;24(2):231-2.
CrossRef - Thorne-Lyman A.L., Valpiani N., Sun K., Semba R.D., Klotz C.L., Kraemer K., et al. Household dietary diversity and food expenditures are closely linked in rural Bangladesh, increasing the risk of malnutrition due to the financial crisis. J Nutr. 2010;140(1):182S-8S.
CrossRef - Tegegne M., Sileshi S., Benti T., Teshome M., Woldie H. Factors associated with minimal meal frequency and dietary diversity practices among infants and young children in the predominantly agrarian society of Bale zone, Southeast Ethiopia: a community based cross sectional study. Archives of public health = Archives belges de sante publique. 2017;75(1):53.
CrossRef - Kabeer N., Mahmud S. Imagining the Future: Children, Education and Intergenerational Transmission of Poverty in Urban Bangladesh. IDS Bulletin. 2009;40(1):10-21.
CrossRef - Hossain N. Exports, equity, and empowerment: The effects of readymade garments manufacturing employment on gender equality in Bangladesh. Background paper for the WDR. 2012.
- Kabir I., Khanam M., Agho K.E., Mihrshahi S., Dibley M.J., Roy S.K. Determinants of inappropriate complementary feeding practices in infant and young children in Bangladesh: secondary data analysis of Demographic Health Survey 2007. Matern Child Nutr. 2012;8 Suppl 1:11-27.
CrossRef - Pryer J.A., Rogers S., Rahman A. The epidemiology of good nutritional status among children from a population with a high prevalence of malnutrition. Public Health Nutr. 2004;7(2):311-7.
CrossRef - Davis C. Examination of the associations between indices of caregiver capabilities on infant and young child feeding practices and nutrition status: University of Washington; 2018.
- Sriram S., Soni P., Thanvi R., Prajapati N., Mehariya K.M. Knowledge, Attitude and Practices of Mothers Regarding Infant Feeding Practices. National Journal of Medical Research. 2013;3(2):147-50.
- National Institute of Population Research and Training (NIPORT). Bangladesh Demographic and Health Survey. The DHS Program, Ministry of Health and Family Welfare GoB; 2011 January 2013. Report No.: FR265.
- Moland K.M., van Esterik P., Sellen D.W., de Paoli M.M., Leshabari S.C., Blystad A. Ways ahead: protecting, promoting and supporting breastfeeding in the context of HIV. International breastfeeding journal. 2010;5(1):19.
CrossRef - Kassier S.M., Veldman F.J. Cry, the beloved bottle: infant-feeding knowledge and the practices of mothers and caregivers in an urban township outside Bloemfontein, Free State province. J South African Journal of Clinical Nutrition. 2013;26(1):17-22.
CrossRef - Alam K., Blanch L., Smith A. Stitched Up: Women Workers in the Bangladeshi Garment Sector: War on Want; 2011. 10 p.
- Bangladesh Labour Act (Ammendment) 45-50 LC. Sect. 4 (2013).
- Islam MZ. Maternity Benefits In Bangladesh Labor Law: An Empirical Study On Apparel Industry. 2015;4(1):1-11.
- Bangladesh Institute of Labour Studies. Women’s Participation In Trade Unions In Bangladesh: Status, Barriers And Overcoming Strategies. International Labour Organization (ILO); 2010 20 March 2010.
- Chowdhury M.S. Compliance With Core International Labor Standards in National Jurisdiction: Evidence from Bangladesh. Labor Law Journal. 2017;68(1):78-93.
- Adugna B., Tadele H., Reta F., Berhan Y. Determinants of exclusive breastfeeding in infants less than six months of age in Hawassa, an urban setting, Ethiopia. International breastfeeding journal. 2017;12:45.
CrossRef - Leung A.K.C., Sauve R.S. Breast is best for babies. Journal of the National Medical Association. 2005;97(7):1010-9.
- Kruger R., Gericke G.J. A qualitative exploration of rural feeding and weaning practices, knowledge and attitudes on nutrition. Public Health Nutr. 2003;6(2):217-23.
CrossRef - Gatti L. Maternal perceptions of insufficient milk supply in breastfeeding. Journal of nursing scholarship : an official publication of Sigma Theta Tau International Honor Society of Nursing. 2008;40(4):355-63.
CrossRef
Accepted on: 27 Jan 2021
Second Review by: Fatemeh Ramezani Ohio
Final Approval by: Neha Sanwalka





Web of Science Coverage
Emerging Sources Citation Index (ESCI)
2024 Journal Impact Factor: 1.1
Scopus Journal Metrics
CiteScore 2025: 2.6
CiteScore Details
Sustainable Nutrition: Food Systems, Nutrient Retention, and Public Health Impact
![]()
This journal is a member of, and subscribes to the principles of, the Committee on Publication Ethics (COPE)








