Maternal Knowledge and Complementary Feeding Practices and their Relationship with Nutritional Status Among Children 6-23 Months Old in Pastoral Community of Marsabit County, Kenya: A Cross-Sectional Study
Joyce Nzilani Mutuku1*
and Justus Osero1 1Department of Community Health and Epidemiology in the School of Public Health and Applied Human Sciences, Kenyatta University, Kenya
2Department of Food, Nutrition and Dietetics in the School of Public Health and Applied Human Sciences, Kenyatta University, Kenya
Corresponding Author Email: mutukujoyn@gmail.com
DOI : http://dx.doi.org/10.12944/CRNFSJ.8.3.17
Download this article as:
![]()
Appropriate complementary feeding practices have positive impact on health and growth of children aged 6-23 months. Little is known about complementary feeding practices among the pastoralists. The aim of this study was to document the influence of maternal knowledge on child feeding and complementary practices on the nutritional status of children aged 6-23 months amongst a pastoral community in Kenya. A WHO standard validated questionnaire was used to collect data from 289 randomly selected mothers/primary caregivers and their children aged 6-23 months. The interviews were conducted through face-to-face in a one-time household visit. The findings showed that half (50.2%) of the children received complementary foods at the age of six months. The proportion of breastfed and non-breastfed children that achieved the recommended Minimum Meal Frequency (MMF) was 28.7% and 2.6% respectively. About one-quarter (23.9%) achieved the recommended Minimum Dietary Diversity (MDD). A total of 5.9% achieved the Minimum Acceptable Diet (MAD). Majority of the mothers/caregivers (95.1%) knew that children should be encouraged to feed while 61.6% knew that children should be fed more frequently during and after illness. The timing of introduction of complementary feeding ([OR]=0.307, P=0.001) and child’s dietary diversity ([OR]=3.112, P=0.020 were predictors of wasting among the children while timing of introduction of complementary feeding ([OR]=0.226, P=0.000) and maternal knowledge on the duration of breastfeeding ([OR]=6.359, P=0.012) predicted child underweight.. Complementary feeding practices are not optimal and the nutritional status of the children is poor. Complementary feeding practices predicted child nutritional status whereas maternal/caregivers’ knowledge on complementary feeding practices had limited impact on child nutrition status.
KEYWORDS:Complementary Feeding; Minimum Acceptable Diet; Minimum Dietary Diversity; Minimum Meal Frequency; Nutritional Status; Pastoralists
Introduction
Infant and young child feeding is critical for child’s health and development since it has direct influence on how a child grows. World Health Organization (WHO) recommends that mothers be empowered and supported to initiate breastfeeding within one hour of birth, practice exclusive breastfeeding for the first six months of life and continue breastfeeding until the child is two years old or more in addition to appropriate complementary feeding1.
Malnutrition in young children is majorly a result of poor practices of complementary feeding 2. Complementary feeding practices have direct effects on child nutritional status and impacts child growth, development and survival 3. The effects of inappropriate feeding practices include poor mental and social development and reduced productivity 4. The first two years of a child’s life are critical for ensuring appropriate growth, health and development through optimal feeding. Improving infant and young child feeding practices during this period when they are most vulnerable is therefore crucial1. Promoting appropriate practices in infant and young child feeding for children below two years is therefore recommended to improve their health and development3.
Children from the developing countries are more affected by poor growth that occurs due to inappropriate complementary feeding practices than those from developed countries. Compromised child growth and development peak during the period when complementary foods are initiated and when breast milk consumption decreases. Poor child feeding practices are considered as one of the major causes of malnutrition. In particular, lack of knowledge on appropriate child feeding practices and cultural practices contribute to poor child nutritional status. Some of the inappropriate feeding practices include too early or too late introduction of complementary foods, lack of dietary diversity and inadequate quantity of food 5.
Appropriate complementary feeding depends on accurate information on child feeding among the caregivers. Inadequate or limited maternal knowledge on what to feed a child on, when and how to feed a child is often a major cause of malnutrition compared to food unavailability 4. In addition, lack of knowledge about the risks associated with poor child feeding practices and the outcome on children’s health, development and survival has resulted to limited actions and interventions to promote optimal practices 6. Nutrition education targeting caregivers on child feeding practices can result into improved child nutritional status and child survival 7. Findings of a research conducted in rural China, for example, showed that nutrition education activities conducted by healthcare providers have the potential to effectively and positively transform caregivers’ practices on complementary feeding and to promote infants’ growth and development 8.
In Kenya, 16% of children are given pre-lacteals before initiation of breastfeeding and 61% of those below six months of age are exclusively breastfed. Initiation of complementary feeding starts before the recommended age of six months for many children. By the age of 4-5 months, 58% of breastfeeding children are fed on semi-solid foods. Less than half (41%) of children 6-23 months of age receive diets with minimum dietary diversity9.
There is limited information with regard to complementary feeding practices and their relationships with nutritional status of children among the pastoralists in Kenya. The residents of Laisamis Sub-county in Marsabit County, the study site, are majorly pastoralists. There are many developmental and humanitarian organizations implementing nutrition and nutrition-related activities in partnership with the County government with the goal of reducing acute malnutrition among the under-fives. Despite these efforts the prevalence of acute malnutrition remains high. The major aim of nutrition surveys conducted in the study area is to establish the prevalence of malnutrition prevalence rather than investigating the drivers of malnutrition. Furthermore, there is limited scientific data on maternal knowledge on complementary feeding and the practice of complementary feeding among children 6-23 months old among pastoralist communities in Kenya. The aim of this study therefore was to establish maternal knowledge on complementary feeding and the practices of complementary feeding and their relationships with child nutritional status in a pastoralist community.
Materials and Methods
Study Design
This was a community-based cross-sectional study to investigate the relationship between complementary feeding practices and nutritional status of children 6-23 months old in Laisamis sub-county, Marsabit County.
Study Area
The study was conducted in Laisamis sub-county of Marsabit county, northern Kenya. Majority of the inhabitants (89.9%) are pastoralists with insignificant practices of crop farming and fishing in a few areas. The sub-county lies in an arid and semi-arid (ASAL) area and experiences chronic food insecurity due to unreliable rainfall. Consequently, a large proportion of the population relies on emergency food aid.
Inclusion Criteria for Study Participants
An inclusion criterion was mothers/primary caregivers and children aged 6-23 months pairs to be recruited into the study because the mothers/caregivers were able to provide information about the child feeding practices. Secondly, the mothers/primary caregivers were included in the study if they together with their children had lived in Laisamis sub-county for at least six months before the study. This period was considered adequate for the mothers/caregivers and their children to have had adequate experience living in the study area to influence the complementary feeding practices.
Exclusion Criteria
Children 6-23 months old with congenital malformation such as cleft palate, limb deformities and chronic diseases were excluded from the study because these conditions can have adverse effects on complementary feeding practices and nutritional status of the children.
Sample Size and Sampling Technique
A random sample of 289 mother/caregiver child pairs was enrolled into the study.
A two-stage cluster sampling technique was used to select the study population. In stage one, two out of five wards in Laisamis sub-county were randomly selected to participate in the study. In stage two, a total of 23 villages from the two wards were randomly selected based on proportion to population size. At the village, simple random sampling was used to select households to be visited among those with children 6-23 months old.
Data Collection Instruments and Data Collection Methods
A semi-structured researcher-administered questionnaire was used to collect data in a one-time household face-face interview with mothers/primary caregivers of children 6-23 months old. The questionnaire consisted of questions that solicited information on the socio-demographic characteristic of mothers/caregivers as well their knowledge on complementary feeding and on practices of complementary feeding. The WHO standard and validated questionnaire on Infant and Young Child Feeding Practices which is widely used in Kenya and other similar circumstances for studies on infant and young child feeding practices was used to collect data in this study10. Complementary feeding practices were determined based on 24-hour recall in accordance with the WHO recommendations. The questionnaire was contextualized to the study objectives and translated from English to the local language (Samburu) that is commonly spoken in the study site. The questionnaire was back translated to English to ensure accurate translation. The questionnaire was pretested for content validity and reviewed based on the feedback.
Weight and length measurements were taken from the children using bathroom scale (SECA model) and length board. Weight was measured twice and the mean taken if the two measurements were within acceptable margin of error and to the nearest 0.1kg. Child’s length was also measured twice and mean of the two measurements taken if they were within the acceptable margin of error and to nearest 0.1cm.
Questionnaire Validity and Reliability
To ensure that data collection instruments measured what they purported to measure, questionnaire was presented to experts in nutrition department of Kenyatta University to establish content validity. The data collection instruments were then reviewed based on the feedback given. Test-retest reliability of the research instrument was established during pretesting. Two pretest sessions with a difference of four days were conducted among 10 caregivers selected from one of the villages not sampled for data collection. Test retest reliability was established by examining the consistency of pre-test responses and reliability co-efficient calculated. The reliability co-efficient was 0.87 and therefore the questionnaire was considered reliable.
Data Analysis
Anthropometric data was entered and analyzed using ENA for SMART Software version 2010 and then exported to SPSS version 20 for cross analysis with other variables. Descriptive statistics (frequency, mean, median, standard deviation and percentages) were used to describe socio-demographic and economic characteristics of the study population, complementary feeding practices and maternal knowledge on feeding practices. Chi –square test was used in univariate analyses to test for association between nominal variables. Logistic regression was used in multivariate analysis to identify the predictors of nutritional status.
Definition of complementary feeding practices and nutritional status
Complementary feeding – Refers to the process of giving solid, semi-solid or soft foods to infants in addition to breast milk. The period for complementary feeding is 6-23 months of age even though breast feeding should continue to two years or beyond1.
Dietary diversity – Refers to food variety consumed from various food groups over a particular period of time. To meet the recommended dietary diversity, children aged 6-23 months old need to be given foods from at least four out of seven food groups1.
Nutritional status – In this study nutritional status refers to anthropometric indices; weight for height Z-score (acute wasting), height for age Z-score (stunting) and weight for age Z-score (underweight). Children with <2 Z-score from median reference were termed as wasted, stunted or underweight3.
Meal frequency – Refers to the number of times a breastfed and non-breastfed child aged 6-23 receives solid, semi-solid or soft foods during the previous 24 hours. This includes milk feeds given to non-breastfeeding children10.
Minimum acceptable diet – It is a composite indicator that shows children 6-23 months who receive both minimum dietary diversity and the minimum meal frequency during the previous 24 hours10.
WHO Indicators of Complementary Practices
Timing of introduction of complementary foods – Refers to introduction of solid, semi-solid or soft foods to children at the age of 6-8 months10.
Minimum meal frequency (MMF) – This is the proportion of breastfed and non-breastfed children 6-23 months who receive solid, semi-solid or soft foods the minimum number times or more10.
Minimum dietary diversity (MDD) – It is the proportion of children 6-23 months of age who receive foods from four or more food groups out of the seven recommended food groups10.
Minimum acceptable diet (MAD) – It is a composite indicator that combines the proportion of children 6-23 months who receive both minimum dietary diversity and minimum meal frequency. This is an indicator of the quality diet10.
WHO Indicators of Complementary Practices
Timing of introduction of complementary foods – Refers to introduction of solid, semi-solid or soft foods to children at the age of 6-8 months10.
Minimum meal frequency (MMF) – This is the proportion of breastfed and non-breastfed children 6-23 months who receive solid, semi-solid or soft foods the minimum number times or more10.
Minimum dietary diversity (MDD) – It is the proportion of children 6-23 months of age who receive foods from four or more food groups out of the seven recommended food groups10.
Minimum acceptable diet (MAD) – It is a composite indicator that combines the proportion of children 6-23 months who receive both minimum dietary diversity and minimum meal frequency. This is an indicator of the quality diet10.
Ethical Considerations
The study received ethical approval from Kenyatta University, Nairobi. Ethical Clearance Committee (Application Number PKU/313/1289). The respondents gave informed consent by either signing or thumb printing before being recruited to participate in the study.
Results and Discussions
Socio-Economic and Demographic Characteristics of the Mothers/Caregivers and Household Heads
A total of two hundred and eighty nine (289) mothers/primary caregivers representing the same number of households were interviewed during the study. Majority of mothers (64.4%) were aged 20-29 years with those aged above 40 years being 4.8%. Most of them (93.4%) were married and 87.5% were house wives and not engaged in any form of in-come generating activities. Only 2.8% were formally employed (Table 1).
Majority (63%) of the household heads was pastoralists and 15.8% were casual labourers (Table 1). Only 3.6% were in formal employment. Three quarters (75.8%) of the household heads had no formal education whereas 14.9% had primary level of education. About two-thirds (65.7%) of the households depended on sale of livestock as the main source of income whereas 14.5% were involved in small scale businesses. Almost all the families (98.6%) obtained their food through purchase, 61.2% from domestic animal products and 15.6% from food aid. A large proportion of households (59.5%) allocated 70% of the total income to food (Table 1).
 |
Table 1: Demographic and Socio-Economic Characteristics of Mothers/Caregivers and Household Heads |
Characteristics of the Children
Both sexes were almost equally represented with 52.2% males and 47.8% females. More than a third (36.0%) of the children were aged between 12 – 17 months, 33.6% were aged 6 – 11 months while the proportion of those aged 18 – 23 months was 30.4%. The mean age was 14.73 (±4.97) months.
Nutrition Status of the Children
About a fifth of the children (21.8%) were wasted with more boys (25.5%) being wasted than girls (17.4%). Overall 26.0% of the children were stunted with a higher percentage (31.8%) of boys being stunted than girls (17.4%). A similar scenario was observed for underweight children, 25.5% with 29.1% boys and 21.0% girls underweight respectively (Table 2).
Table 2: Prevalence of Under Nutrition Among the Children 6-23 Months Old
| Alln = 289 | Boysn = 151 | Girlsn = 138 | |
| Wasting | (63) 21.8 %(14.7 – 31.1 95% C.I.) | (39) 25.8 %(13.9 – 42.9 95% C.I.) | (24) 17.4 %(12.3 – 24.0 95% C.I.) |
| Stunting | (75) 26.0 %(16.3 – 38.7 95% 95% CI.) | (48) 31.8 %(19.3 – 47.5 95% 95% CI.) | (27) 19.6 %(10.9 – 32.5 95% C.I.) |
| Underweight | (73) 25.3 %(20.0 – 31.3 95% C.I.) | (44) 29.1 %(20.2 – 40.0 95% C.I.) | (29) 21.0 %(13.8 – 30.7 95% C.I.) |
Complementary Feeding Practices
About half (50.2%) of the children received complementary foods at the age of 6 months (Table 3). The proportion of breastfed and non-breastfed that achieved the recommended Minimum Meal Frequency (MMF) per day was 28.7% and 2.6% respectively. Less than a quarter (23.9%) attained the Minimum Dietary Diversity (MDD) and only 5.9% attained Minimum Acceptable Diet (MAD) (Table 3).
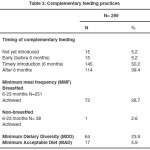 |
Table 3: Complementary Feeding Practices |
Maternal Knowledge on Complementary Feeding Practices
A large majority of the mothers (95.1%) knew that children should be encouraged to eat even when they have low appetite; 79.2% knew the correct age when children should be introduced to complementary feeding and the lowest knowledge exhibited was about feeding children more frequently during and when recovering from an illness as reported by 61.6% of the mothers/caregivers (Table 4).
 |
Table 4: Maternal Knowledge on Various Aspects of Complementary Feeding Practices |
Relationships Between Complementary Feeding Practices and Child Nutritional Status
A chi-square test revealed significant relationships between the time of initiation of complementary feeding and the three indicators of nutrition status; underweight, wasting and stunting (Chi-square test = 23.33, p=0.000, Chi-square test =12.428, p=0.002 and Chi-square test =10.823, p=0.004 respectively (Table 5).
 |
Table 5: Relationship Between Complementary Feeding Practices and Child Nutritional Status |
Association Between Maternal Knowledge on Complementary Feeding and Child Nutritional Status
Mothers who reported that the duration of breastfeeding should be two years and beyond were less likely to have children who were underweight (Chi-square test =7.323, p=0.017) compared to those who stated otherwise. The children of those mothers who knew that children should be fed more frequently and given food more frequently during and after illness were less likely to have underweight children (Chi-square test =12.028, p=0.002). Mothers who responded positively that complementary feeding before six months poses health risk to the child were less likely to have stunted children (Chi-square tests =8.025, p= 0.033) than those who responded negatively. Mothers who stated that introduction of complementary feeding should start after a child attains six months of age were more likely to have underweight children (Chi-square test 6.542, p= 0.030) than those who knew that children should be introduced to complementary feeding at 6 months (Table 6).
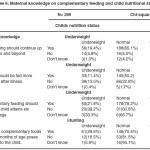 |
Table 6: Maternal knowledge on complementary feeding and child nutritional status |
Predictors of Child Nutritional Status
Factors that had significant relationship with child nutritional status in bivariate analysis (chi-square test) were subjected to a multinomial logistic regression analysis to establish the predictors of child nutritional status (Table 7). In terms of complementary feeding practices, timing of the introduction of complementary feeding was a predictor of underweight and wasting whereas minimum dietary diversity was a predictor of wasting. Maternal knowledge was also a predictor of nutritional status of children. Maternal/caregivers’ knowledge about the duration of breastfeeding was a predictor of underweight (Table 7).
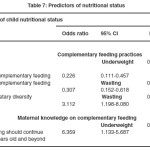 |
Table 7: Predictors of Nutritional Status |
Discussion
Prevalence of Under Nutrition
The prevalence of stunting in the study site was high (26%) an indication of chronic malnutrition among the children. The stunting rate compares with that of the findings of nutrition survey conducted in Marsabit 11. A higher percentage of boys were stunted compared to the girls and this finding also compares with findings of a nutrition survey conducted in Isiolo County, a neighbouring ASAL region whose residents are also pastoralists12. The prevalence of underweight was high (25.3%) and this was in agreement with nutrition survey findings for Turkana County and a similar study conducted in Aceh Besar District, Indonesia13,14. The underweight rate was however lower compared to that of Marsabit County 11. The study results revealed higher prevalence of underweight among the boys than girls concurring with the results of nutrition surveys conducted in Turkana and Samburu counties in northern Kenya13,15. The prevalence of wasting was also high among the children; with a higher prevalence among the boys as demonstrated in surveys conducted in the neighbouring ASAL counties of Isiolo and Samburu12,15. The higher prevalence of underweight, stunting, and wasting among boys than girls in this study is consistent with the national rates in Kenya9. Studies in other African countries have also demonstrated similar findings, for example, a study conducted in Nigeria by Ekerette et al2.
The high malnutrition prevalence in Laisamis sub-county could be attributed to the chronic food insecurity due to its dry climatic conditions and consequently affecting nutritional status of children. For improved nutritional status to be achieved among children 6-23 months old in Laisamis sub-county, interventions should also address food availability and accessibility since this has been reported to be a major limitation to appropriate child feeding practices in the Knowledge, Attitudes, Practices and Beliefs (KAPB) surveys conducted in Marsabit16.
Complementary Feeding Practices
In this study, majority (86.9%) of the children 6-23 months old were still breastfeeding and this is comparable to the Kenya national rate9. The percentage still breastfeeding was however higher than that reported in a KAPB survey conducted in Marsabit county (69.0%) and Samburu county (41.1%)16,17. A study conducted at Lahore in Pakstani by Hasnain et al. showed that majority of children 6-23 months of age were still being breastfed alongside complementary feeding18.
Initiation of adequate and safe complementary foods at the appropriate time is essential for optimal health and improved child nutritional status especially during the period of increased nutritional needs19. In the current study, half of the children were appropriately initiated to complementary foods at the age of 6 months. This percentage was double that reported in a study conducted in Nigeria2 but similar to those of researches done in Indonesia and Napel14,20. The percentage of children who were introduced timely to complementary feeding in this study was higher than that reported in KAPB surveys conducted in other arid and semi-arid (ASAL) areas in Kenya; Marsabit County (44.3%), Samburu County (47.9%) and Turkana County (36.0%)16,17,21 but lower than that of a similar study done in the informal settlement in Nairobi, Kenya22. More than one third of the children in this study were introduced to complementary foods late (after six months) concurring with findings of a KAPB survey for Turkana County and a similar study done in Pakistan21,23. This implies that many children were not getting the right quantity and quality of nutrients for their growth and development because breastmilk is not adequate to provide all the required nutrients from 6 months of age.
Minimum Meal Frequency (MMF) is considered a proxy for energy intake from foods other than breastmilk. Majority (74.7%) of the children in this study did not achieve MMF unlike that reported in a study conducted in Jigjiga, Ethiopia, a town that lies in a region where about 85% of population depends on pastoralism or agro-pastoralism for livelihood24. The findings of this study differed with those of a KAPB survey conducted in Marsabit County, (Laisimis sub-county the study site is part of the Marsabit County) that showed that close to half of the children 6-23 months old attained minimum meal frequency16. This difference could partly be attributed to the fact that in Marsabit County there are some regions that have favourable climatic conditions for crop farming and therefore have better food security status and accessibility to a wider variety of foods. Laisamis sub-county is mainly arid with no significant practice of crop farming.
Growth, development and survival of all infants from the age of six months onwards depends largely on additional provision of foods supplied through complementary foods in order to help them grow into healthy and active adults. They need to be fed on an appropriate diet that provides all the nutrients and energy required for normal growth and vitamins and minerals to alleviate their hidden hunger and keep them strong23. The findings of this study showed poor complementary feeding in terms of dietary diversity with less than one-quarter of the children having attained the Minimum Dietary Diversity (MDD). Studies have shown varying rates in the achievement of MDD among children. Some studies have shown high rates of MDD among children such as those conducted in Nigeria and Ethiopia25,26. In contrast, studies such as that conducted in Nigeria by Ekertte have demonstrated low rates of MDD among children2. The finding of this study in regard to MDD was similar to that of a KAPB survey done in Samburu County, Kenya17.
Researches conducted in ASAL regions have shown low MDD. Nutrition surveys for Marsabit and Turkana Counties revealed low MDD of 15.5%, and 19.5% respectively16,21. The low MDD could be attributed to the issue of food insecurity leading to poor food unavailability and inaccessibility.
In this study, a very small proportion (5.9%) of the children achieved Minimum Acceptable Diet (MAD), implying low quality diet consumed by a majority of the children. This is similar to findings of a study done in Ethiopia26. This low rate of the attainment of MAD compares to those of the nutrition survey findings conducted in Laisamis (5.4%) and North Horr (4.8%) sub-counties of Marsabit County16. The finding however differs with that of the larger Marsabit County that reported a higher proportion (15.6%) of children 6-23 months having achieved MAD16. In this study, the low MAD may be attributed to the consumption of diet with low diversity of foods and low feeding frequency probably due to prolonged food insecurity in the region.
Some cultural beliefs have also been identified as hindrances to appropriate child feeding practices. KAPB surveys conducted in Marsabit and Samburu counties in Kenya reported that some foods are not fed to children below two years of age because they are associated with delayed speech and ill health16,17. Appropriate child nutrition messages (including those addressing cultural hindrances) should be developed and up-scaled through behavior change communication.
Maternal Knowledge on Complementary Feeding and Child Nutritional Status
Accurate information on complementary feeding is crucial for improved child feeding practices. In addition, focused support from the family and community members together with a well-established health care system can positively contribute to improved practices and behaviors around child feeding4. This study revealed high maternal knowledge regarding complementary feeding that does not necessarily translate into appropriate complementary feeding practices and consequently improved child nutritional status. This finding compares to those of surveys and studies conducted in other parts of Kenya as well as Pakistan17,21,22,23. A study conducted in Jigjiga town in Ethiopia also demonstrated high maternal knowledge on complementary feeding24. In this study the proportion of mothers/primary caregivers who knew that late introduction of complementary feeding could result to child malnutrition was higher compared to that of a study done in Nigeria25. Maternal knowledge on child feeding frequency was consistent with that of a study conducted in Lahore, Pakistan that revealed lower maternal knowledge on child feeding frequencies18. The reason for high maternal knowledge on complementary feeding practices in Laisamis sub-county could probably be due to the presence of many Non-Governmental Organizations (NGOs) and Community Based Organizations (CBOs) that implement nutrition programmes focusing on behavioral change in collaboration with the County government. The behaviour change communication focuses on the promotion of optimal infant and young child feeding practices.
As a whole, only one aspect of maternal knowledge (the correct duration of breastfeeding) was associated with child nutritional status. Knowledge is a pre-requisite for optimal practices in child feeding. The results of this study has demonstrated that despite the high maternal knowledge on complementary feeding practices – this knowledge did not to a large extent lead to optimal practices, implying that factors other than knowledge influenced complementary feeding practices to a greater extent. Similar findings have been shown in many studies investigating the relationship between maternal knowledge and complementary feeding practices. KAPB surveys conducted in, Marsabit, Samburu and Turkana Counties in Kenya revealed high maternal knowledge on complementary feeding practices that had limited positive effects on child nutritional status16,17,21. A study in Ethiopia by Yimer also revealed high maternal knowledge with no significant association with complementary feeding practices24. Some studies have however demonstrated the contrast, that maternal knowledge has a positive effect on child nutritional status. A study done in Nairobi, Kenya indicated that maternal knowledge on complementary feeding had positive effect on child feeding practices and nutritional status22.
Predictors of Nutritional Status
The main predictors of poor child nutritional status were inappropriate child feeding practices. Correct timing of initiation of complementary feeding and minimum dietary diversity were predictors of wasting and underweight among the children. These findings are in line with those of other studies conducted in Kenya22,27 and also reported in Cross River State, Nigeria by Ekerette et al.2. The findings of this study are however not similar with those of a study done in Indonesia that revealed no relationship between complementary feeding and child nutritional status14.
Maternal knowledge was not a major predictor nutritional status. The findings of this study demonstrate the need to address context-specific factors in the promotion of appropriate child feeding practices because there is no one-fix for all the challenges experienced.
The major strength of this study is its contribution to the body of knowledge of complementary feeding practices among pastoralist communities which has hitherto received limited attention in research.
The major limitation of the study is that, being a cross-sectional study design, the findings do not reflect the effect of seasonality on complementary feeding practices in the study area.
Conclusions
The complementary feeding practices in the area of study are not optimal and the nutritional status of the children 6-23 months old is poor. Mothers’/caregivers’ knowledge in regard to complementary feeding is high but with no positive impact on nutritional status of children in Laisamis sub-county. Efforts to improve nutritional status of the children in Laisamis sub-County should go beyond imparting knowledge on appropriate feeding practices to tackling household food insecurity which is the major reason for inappropriate complementary feeding practices as reported in other studies conducted in the semi-arid regions such as the study area.
Funding Source
No financial support was received to conduct this research but was financed by the researchers.
Conflict of Interest
The authors declare that no conflict of interest in this article.
References
- WHO. Infant and young child feeding: Model chapter for textbooks for medical students and allied health professional (2009).
- Ekerette E. U., Olukemi K. A. Complementary feeding practices among mothers and nutrition status of infants in Akpabuyo area, Cross river state Nigeria. Udoh and Amodu SpringerPlus, 2016;5:2073.
CrossRef - WHO. Strengthening action to improve feeding of infants and young children 6-23 months of age in nutrition and child health programmes. Geneva, (2008).
- WHO. Global Strategy for Infant and Young Child Feeding (2003).
- USAID. Behavior change intervention and child nutritional status: Evidence from the The promotion of improved complementary feeding practices (2011).
- Black R. B., Allen L. H., Bhutta Z. A., Caulfield L.E., Onis M., Ezzat M., Mathers C., Ruvera J. Maternal and child under nutrition: Global and Regional exposure and Consequences. 2008; 371(9608):243-60.
CrossRef - Lartey A. Maternal and child nutrition in Sub-saharan Africa: Challenges and Interventions. Proceedings of the Nutrition Society. 2008; 67:105-108.
CrossRef - Shi L., Zhang J., Wang Y., Caulfield L. E., Guyer B. Effectiveness of an educational intervention on complementary feeding practices and growth in rural China: A Cluster randomized Controlled Trail. Public Health Nutrition. 2009;13(4):556-565.
CrossRef - Kenya National Bureau of Statistics (KNBS) & ICF macro. 2010. Kenya Demographic Health Survey Caverton, Maryland: KNBS and ICF macro (2014).
- WHO. Indicators for Assessing Infant and Young Child Feeding practices: Part 1. Conclusions of a consensus meeting, Washington D.C., USA (2008).
- MOH/UNICEF. Standardized Monitoring and Assessment of Relief and Transitions (SMART) nutrition survey report for Marsabit County, Kenya (2017).
- MOH/UNICEF. Standardized Monitoring and Assessment of Relief and Transitions (SMART) nutrition survey report for Isiolo County, Kenya (2018).
- MOH/UNICEF. Standardized Monitoring and Assessment of Relief and Transitions (SMART) nutrition survey report for Turkana County, Kenya (2018).
- Aripin A., Siti, M., Cesilia M. D., Risatianti K. Complementary feeding practices and nutritional status of children 6-23 months old: formative study in Aceh, Indonesia. Nutrition Research and Practice. 2018;12(6):512-52.
CrossRef - MOH/UNICEF. Standardized Monitoring and Assessment of Relief and Transitions (SMART) nutrition survey report for Samburu County, Kenya (2018).
- MOH/UNICEF. Maternal Infant and Young Child Nutrition (MIYCN) Knowledge, Attitudes, Beliefs and Practices (KABP) Survey Report for Marsabit County, Kenya (2018).
- MOH/UNICEF. Maternal Infant and Young Child Nutrition (MIYCN) Knowledge, Attitudes, Beliefs and Practices (KABP) Survey Report for Samburu County, Kenya (2018).
- Hasnain S., Majrooh M. A., Anjum R. Knowledge and practices of mothers for complemenatry feeding in babies visiting pediatrics outpatient department of Jinnah hospital, Lahore. Biomedica. 2013;29(4):221-230.
- WHO. Feeding and nutrition of infant and young children: Guidelines for the WHO European Region, with emphasis on the former soviet countries (2003).
- Helen Keller International. Household food insecurity and nutritional status of Children aged 6-23 months in Kailali district of Nepal (2010).
- MOH/UNICEF. Maternal Infant and Young Child Nutrition (MIYCN) Knowledge, Attitudes, Beliefs and Practices (KABP) Survey Report for Turkana County, Kenya (2017).
- Korir J. K. Determinants of complementary feeding practices and nutritional status of children 6-23months old in Korogocho slum, Nairobi County, Kenya (2013). A thesis presented at the department of Foods, Nutrition and Dietetics, Kenyatta University, Nairobi.
- Liaqat P., Rizvi M. A., Qayyum A., Ahmed H., Ishtiaq N. Maternal Education and complementary feeding: Pakistan Journal of Nutrition. 2006;5(6):563-568.
CrossRef - Yimer M. Maternal Knowledge on Complementary Feeding Practice and Nutritional Status
- of Children 6-23 Month in Jigjiga Town. Global Journal of Nutrition & Food Science. 2018;1(1): GJNSF.MS.ID.000505.
- Foluke A. O., Jesupelumi O. A., Adedeji A., Oluwafunmilayo F. A. Complementary Feeding Knowledge, Practices, and Dietary Diversity among Mothers of Under-Five Children in an Urban Community in Lagos State, Nigeria. International Journal of MCH and AIDS. 2017;6 (1), 46-59.
CrossRef - Disha A. D., Rawat R., Subandoro A., P. Menon. Infant and Young Child Feeding (IYCF)
- Practices in Ethiopia and Zambia and their Association with Child Nutrition: Analysis of Demographic and Health Survey Data. African Journal of Food, Agriculture, Nutrition and Development. 2012;12(2): ISSN 1684 5374
- Judith K., Peter C. Complementary feeding practices and nutritional status of children 6-23 months in Kitui county, Kenya. Journal of applied Biosciences. 2015;85(1): 7881-7890.
CrossRef
Accepted on: 9/10/2020
Second Review by: Dr.Monica Romania
Final Approval by: Dr. Neha Sanwalka





Web of Science Coverage
Emerging Sources Citation Index (ESCI)
2024 Journal Impact Factor: 1.1
Scopus Journal Metrics
CiteScore 2025: 2.6
CiteScore Details
Sustainable Nutrition: Food Systems, Nutrient Retention, and Public Health Impact
![]()
This journal is a member of, and subscribes to the principles of, the Committee on Publication Ethics (COPE)








