Glycemic Index of Two Different Fried Potato Varieties Cultivated Under Organic Fertilization Conditions
1University of Athens, School of Physical Education and Sports Science, Greece
2TEI Peloponnese, Dept. Food Technology, Kalamata, Hellas.
Corresponding Author Email: theovarzakas@yahoo.gr
DOI : http://dx.doi.org/10.12944/CRNFSJ.4.1.02
Download this article as:
![]()
This study identified the glycemic index (GI) of two different commercially available varieties of potatoes, Lady Rosetta (LR) and Spunta (S), cultivated under organic fertilization conditions and fried in extra virgin olive oil. Eight healthy males 26 ± 1.5 years of age, 84.7 ± 3.2 Kg body mass and 19.2 ± 1.5% of body fat participated (mean ± SE). Volunteers consumed in a random order 50 g of anhydrous glucose in 300 ml of water (G), or 50 g of available carbohydrate of sliced and fried LR or S twice. Blood glucose was measured enzymatically from capillary blood samples before food consumption and at 15, 30, 45, 60, 90 and 120 min postprandially. Each meal was prepared and consumed in the morning after a 12-hour overnight fast, whereas diet and physical activity were controlled. For the calculation of GI the mean blood glucose values of the two trials (i.e. 1st and 2nd time) in each potato variety (i.e. LR or S) were considered. The incremental area under the blood glucose-time curve (IAUC) was used according to trapezoidal rule for the determination of GI. The IAUC was 5504 ± 1173 mg.min/dl and 4012 ± 911 mg.min/dl whereas the GI was 114 ± 15 and 83 ± 12 in LR and S respectively. However, these differences were not significant (IAUC: p= 0.21 and GI: p=0.20). Fried potato slices in extra virgin olive oil derived from LR and S potato varieties cultivated under organic fertilization conditions possess similar GI in healthy male volunteers.
KEYWORDS:glycemic index; French fries; biological fertilization
Introduction
The importance of the glycemic index (GI) in diet and health in general has been questioned by some scientists.1,2 However, the consumption of foods with low GI as well as a low glycemic load in the daily diet is epidemiologically linked to positive health effects such as better control of blood glucose, blood lipid and the body weight and reducing the risk of diabetes and heart disease.3-13 For these reasons, the World Health Organization as well as other scientific bodies recommend the bulk of dietary carbohydrates to come from foods with low GI.14-16
Potato consumption in the daily diet both in Greece and around the world is very high and this fact justifies the widespread cultivation of many potato varieties. In Greece potatoes are grown throughout the country (Viotia, Evia, Achaia, Ilia, Messinia, Crete, Evros, Drama, Arcadia) in an area of up to 500,000 hectares and annual production of more than 1,000,000 tons.
In many investigations researchers have studied the GI of various potato varieties such as Asterix, Burbank Russet, California White, Charlotte, Desiree, Ontario White, Pontiac, Prince Edward Island, Sebago etc. But the way of cooking was usually boiling, baking in the oven or in microwave, boiling and melting (mashed potato), pre-cooked (boiled or baked) and recooked, or even manufacture of ready mashed (instant potato).17-29 The determination of the GI of different potato varieties has also been carried out by in vitro analysis.22,30 The most popular way of potato consumption (French Fries) in olive oil is not well studied, while GI of tubers shaped as French Fries has been determined by heating in an oven or micro wave.25,27,29 Even the GI of widely-used potato varieties marketed in Greece and Europe as the Lady Rosseta and Spunta has not been studied.
The GI of a food depends on many factors such as the type of starch, cooking method, the degree of processing the food has undergone, the amount of fiber and the viscous degree thereof, the acid content, the levels of sugar, fat and protein,14 or even if the food is served cooked from fresh or recooked after refrigerated storage.27,31
The structure of the starch in a food may be comprised of long-chain glucose (amylose) and branched chain glucose (amylopectin). Because of the amylopectin structure is readily accessible to the appropriate enzymes for hydrolysis, the proportion of amylose to amylopectin in a food affects the GI.32 Since it has been observed that the variety of potato also affects the GI,27 it would be interesting to study the GI of different potato varieties with different amylose / amylopectin ratio. Finally, the ever increasing demand and offer biologically cultivated food is an additional reason to study the GI biologically cultivated potato varieties.
Therefore, the aim of this investigation was to study and determine the GI of two different commercially available varieties of potatoes, Lady Rosetta (LR) and Spunta (S), cultivated under organic fertilization conditions and fried in extra virgin olive oil.
Methods
Experimental Design
Eight healthy males 26 ± 1.5 years of age, 84.7 ± 3.2 Kg body mass and 19.2 ± 1.5% of body fat participated (mean ± SE). Volunteers consumed in a random order 50 g of anhydrous glucose (D-Glucose monohydrate) in 300 ml of water (G), or 50 g of available carbohydrate of sliced and fried LR or S twice. Blood glucose was measured enzymatically from capillary blood samples before ingestion and at 15, 30, 45, 60, 90 and 120 min postprandially. Each meal was prepared and consumed in the morning after a 12-hour overnight fast, whereas diet and physical activity were controlled. For the calculation of GI the mean blood glucose values of the two trials (i.e. 1st and 2nd time) in each condition (i.e. LR or S) were considered. The incremental area under the blood glucose-time curve (IAUC) was used according to trapezoidal rule for the determination of GI7,15,20,33,34 according to the following mathematical formula:
GI = (Potato testIAUC / Glucose controlIAUC) x 100
Where GI = glycaemic index,
Potato testIAUC= IAUC of LR or S,
Glucose controlAUC = IAUC of glucose.
Preliminary Measurements, Physical Activity and Diet Control
Body mass measurements were taken with an appropriate scale (Seca 711, UK). The percentage of body fat was estimated by the method of densitometry and skinfolds using a skinfold caliper (Harpenden, RH15 9LB, UK) and equations of Durnin & Womersley.35
Volunteers were required to avoid any physical activity two days before each trial. Also, they were asked to record their food intake the day before the first trial and to replicate this in the next tials.
Experimental Procedures
Volunteers arrived at the laboratory at 8:00 hrs and after relaxing for 10 min in a sited position placed their hand in warm water for 5 min in order to increase the blood flow to the fingers from which samples of arterialized capillary blood were taken. This procedure is suggested as more accurate for the determination of blood glucose compared to blood samples taken from an anticubital vein.36,37 After the 5-min warm-up of the hand volunteers dried their hand and a dublicate 25 μl of capillary blood sample was collected in calibrated glass micropipets (Micropipets Ringcaps Duran 25 μl, Fisher Scientific, Germany) using a one-use sterile fine needle (Microlet, Bayer Germany). The content of each 25 μl sample was immediately placed in 1.5 ml tubes containing 250 μl of 2.5 % perchloric acid to deproteinize the blood. After that tubes were centrifuged (Eppendorf, Model 5414, USA) for 5 min at 1500 g and stored at -35 oC for the determination of blood glucose. This procedure was identically followed for all blood samples taken.
Following the collection of the preprandial blood sample volunteers consumed either 50 g of G in 300 ml of water (G), or 50 g of available carbohydrate in the form of fried LR (LR), or 50 g of available carbohydrate in the form of fried S (S) accompanied with 300 ml of water. Each of the LR and S conditions was conducted twice at different days due to the variety of blood glucose postprandially when food is consumed.15 Volunteers were instructed to consume the meals within 5 min whereas during the 2-hour postprandial period no water or other form of food was allowed. The postprandial period was initiated immediately after the ingestion of G, LR, or S.
Preparation and frying of potato tubers
Potato tubers were harvested, washed, dried and stored in a refrigerator at 5-8 ° C temperature. Within 7-10 days the tubers were used for preparing fried potatoes. The day on which the participants consumed the LR or S, tubers were washed, had their peel removed and cut into 0.5 cm thick slices. Frying was done with extra virgin olive oil at 180-190 ° C for 15 min. Then the fried potato slices were placed on a paper towel for 3 minutes to remove as much quantity of oil and were served to the participants. The quantity of food for both varieties was 250 g, which value was indicative of starch and sugar measurements at the Laboratory of Food Chemistry TEI Kalamata and identified available carbohydrates in 20 g / 100 g of food.
Blood glucose analysis
Blood glucose was carried out enzymatically using a reagent of Randox company (GOD-PAP, GL 26 23, Randox Lab. Ltd, UK) with the aid of a suitable spectrophotometer (Jenway Spectrophotometer 6300, Jenway, UK). For each blood sampling time point two samples were collected. When analyzing the samples, each sample was analyzed in duplicate so that the final value of each time point (preprandially, 15 min, 30 min, 45 min, etc.) was determined from the average of four blood glucose readings for greater accuracy and reduction of possible errors during blood receiving. It should also be noted that all the samples of the five conditions (ie. 2 x LR, 2 x S, and 1 x G) per participant were simultaneously analyzed on the same day.
Statistical analysis
Changes in blood glucose versus time (Condition x Time) for 3 conditions (G vs. LR vs. S) were analyzed using 2-way Analysis of Variance (ANOVA) for repeated measures. Comparison of the IAUC value for the 3 conditions (G vs. LR vs. S) was carried by one-way ANOVA for repeated measures. When the variance of the values in ANOVA showed no sphericity, Epsilon Greenhouse-Geisser correction factor was used for the degrees of freedom. To determine the differences between the averages (post-hoc test) in case of significance in ANOVA the Bonferroni method for multiple comparisons was used. The comparison of the GI between the two potato varieties (LR vs. S) was performed with the Student’s T- test for double distribution (2-tailed) for repeated measures. Data are presented as values of Mean ± Standard Error (SE). The significance level was set at p <0.05.
Results
Blood Glucose
The blood glucose responses in the three conditions are presented in Figure 1. Blood glucose peaked at 30 min postprandially in G whereas in LR and S at 60 min. Statistical analysis did not show any difference between G (125 ± 5 mg.dl-1), LR (130 ± 9 mg.dl-1) and S (118 ± 6 mg.dl-1) in the main effect level (F2,14 = 2.44, p=0.12), neither at interaction level (meals x time) (F3.07, 21.52 = 2.40, p=0.095). However, a time effect was observed (i.e: 15 min vs. 30 min vs. 45 min…etc) (F1.96, 13.96 = 12.376, p=0.001). In particular and irrespective conditions blood glucose was higher at 30 min (138 ± 8 mg.dl-1 ; p=0.006) and 45 min (157 ± 16 mg.dl-1 ; p=0.02) compared to preprandial values ( 0 min: 90 ± 2 mg.dl-1).
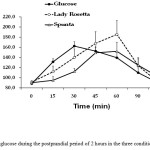 |
Figure 1: Blood glucose during the postprandial period of 2 hours in the three conditions (mean ± SE). |
IAUC and GI
The IAUC in the 3 conditions is presented in Figure 2. The IAUC in LR was 19% higher than in G, whereas the IAUC in S was 16% lower than in G. These differences, however, were not significant between conditions (F2,14 = 1.737, p=0.21).
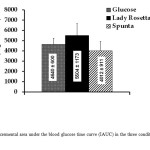 |
Figure 2: Incremental area under the blood glucose time curve (IAUC) in the three conditions (mean ± SE). |
The GI in the two potato varieties is presented in Figure 3. Although the GI in LR was about 37% higher than in S this difference was not significant (p= 0.20).
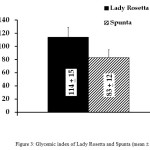 |
Figure 3: Glycemic index of Lady Rosetta and Spunta (mean ± SE).
|
Discussion
Both potato varieties possessed GI> 80 that classifies these foods with high (> 70) GI15,38,39 Many researchers have also reported high GI for different potato and different ways of cooking varieties such as boiling, boiling and melting (mashed), baking in the oven or microwave and manufacture of ready mashed (instant mashed potato) in healthy and diabetic subjects.17-29,39 However, almost the same researchers report lower values of GI (51-70) for boiled potatoes, baked, chips or canned potato products also in healthy and diabetic individuals.20,26-29,33 The reasons for these differences as presented in the literature may have to do with how the potato tubers are cooked, as well as the potato variety.27 In a recent study that investigated the effect of frying on the molecular structure of potato starch it was observed that when potato chips from Spunta and Lady Rosetta varieties fried in soybean oil and overcooked a more noticeable effect on the molecular structure of the starch was produced compared to olive oil and undercooking and this may well affect the GI of the food.40 Generally speaking, however, potatoes present a higher GI compared to many other foods such as white bread, cereal, rice, pasta, fruits, vegetables and dairy.38,39
Furthermore, despite the fact that the GI for LR (114 ± 15) was about 37% higher than that of S (83 ± 12) this difference was not found statistically significant (p= 0.20). One reason might be the similarity of the available carbohydrates in the two varieties (20 g /100 of food). Another reason might be that the type of starch (amylose/ amylopectin ratio) between LR and S was probably not so different to cause different postprandial glucose increase which in turn would create a difference in the GI of the two potato varieties.
In conclusion, the GI of LR and S potato varieties cultivated under organic fertilization conditions is high (> 80) but do not differ from each other when they are consumed in the form of fried slices in olive oil in healthy males.
Acknowledgments
Research project co-financed by the European Union (European Social Fund) and Greek National Funds through the Operational Program Education and Lifelong Learning of the National Strategic Reference Framework (NSRF)-Research Funding Program: Archimedes III, Work program 6, TEI Peloponnese (ex Kalamata).
References
- Pi-Sunyer F. X. (2002) Glycemic index and disease. American Journal of Clinical Nutrition, 76:290S–298S.
- Beals K. A. (2005) The Glycemic Index: Research Meets Reality. United States Potato Board, Special Publication. Available in: http://www.uspotatoes.com/downloads/3581giwhite.
- Salmerón J, Manson J. E., Stampfer M.J., Colditz G.A., Wing A.L., Willett W.C. (1997) Dietary fiber, glycemic load, and risk of non-insulin-dependent diabetes mellitus in women. Journal of the American Medical Association, 277(6):472-477.
CrossRef - Liu S., Willett W. C., Stampfer M. J., Hu F. B., Franz M., Sampson L., Hennekens C. H., and Manson J. E. (2000) A prospective study of dietary glycemic load, carbohydrate intake, and risk of coronary heart disease in US women. American Journal of Clinical Nutrition, 71:1455–61.
- Buyken A. E., Toeller M., Heitkamp G., Karamanos B., Rottiers R., Muggeo M., and Fuller J. H. (2001) Glycemic index in the diet of European outpatients with type 1 diabetes: relations to glycated hemoglobin and serum lipids. American Journal of Clinical Nutrition, 73: 574-581.
- Ford E. S. and Liu S. (2001) Glycemic index and serum high-density lipoprotein cholesterol concentration among US adults. Archives of Internal Medicine, 161: 572-576.
CrossRef - Brand-Miller J. C., Holt H. A., Pawlak D. B., and McMillan J. (2002) Glycemic index and obesity. American Journal of Clinical Nutrition, 76(suppl):281S–285S.
- Liu S., Willett W. C., Manson J. E., Hu F. B., Rosner B., and Colditz G. (2003) Relation between changes in intakes of dietary fiber and grain products and changes in weight and development of obesity among middle-aged women. American Journal of Clinical Nutrition, 78(5):920-927.
- Ebbeling C. B., Leidig M. M., Sinclair K. B, Seger-Shippee L. G., Feldman H. A., and Ludwig D. S. (2005) Effects of an ad libitum low-glycemic load diet on cardiovascular disease risk factors in obese young adults. American Journal of Clinical Nutrition, 81:976–82.
- Oh K., Hu F. B., Cho E., Rexrode K. M., Stampfer M. J., Manson J. E., Liu S., and Willett W. C. (2005) Carbohydrate intake, glycemic index, glycemic load, and dietary fiber in relation to risk of stroke in women. American Journal of Epidemiology, 161:161–169.
CrossRef - Burani J and Longo P. L. (2006) Low–Glycemic Index Carbohydrates. An Effective Behavioral Change for Glycemic Control and Weight Management in Patients With Type 1 and 2 Diabetes. The Diabetes Educator, 32: 78-88.
CrossRef - Hare-Bruun H., Nielsen B.M., Grau K., Oxlund A. L., and Heitmann B. L. (2008) Should glycemic index and glycemic load be considered in dietary recommendations? Nutrition Reviews, 66(10):569–590.
CrossRef - Burger K. N. J., Beulens J. W. J., Boer JMA, Spijkerman A. M. W., van der A D. L. (2011) Dietary Glycemic Load and Glycemic Index and Risk of Coronary Heart Disease and Stroke in Dutch Men and Women: The EPIC-MORGEN Study. PLoS ONE 6(10): e25955. doi:10.1371/journal.pone.0025955.
CrossRef - FAO/WHO (1998) Carbohydrates in human nutrition: Report of a joint FAO/WHO Expert Consultation, Rome. Food and Agriculture Organization, Food and Nutrition paper 66.
- Foster-Powell K, Holt SH, Brand-Miller JC (2002) International table of glycemic index and glycemic load values: 2002. American Journal of Clinical Nutrition, 76(1):5-56.
- Riccardi G., Rivellese A. A., and Giacco R. (2008) Role of glycemic index and glycemic load in the healthy state, in prediabetes, and in diabetes. American Journal of Clinical Nutrition, 87(suppl): 269S-274S.
- Crapo P. A., Reaven G., Olefsky J. (1977) Postprandial plasma-glucose and insulin responses to different complex carbohydrates. Diabetes, 26:1178–1183.
CrossRef - Crapo P. A., Kolterman O. G., Waldeck N., Reaven G. M., Olefsky J. M. (1980) Postprandial hormonal responses to different types of complex carbohydrate in individuals with impaired glucose tolerance. American Journal of Clinical Nutrition, 33:1723–1728.
- Crapo P. A., Insel J., Mark Sperling M., and Kolterman O. G. (1981) Comparison of serum glucose, insulin, and glucagon responses to different types of complex carbohydrate in non insulin-dependent diabetic patients. American Journal of Clinical Nutrition, 34: 184- 190, 1981.
- Jenkins D. J. M., Wolever T. M. S., Taylor R. H., Barker H., Fielden H., Baldwin J. M.., Bowling A. C., Newman H. C., Jenkins A. L. and Goff D. V. (1981) Glycemic index of foods: a physiological basis for carbohydrate exchange. American Journal of Clinical Nutrition, 34: 362-366.
- Jenkins D. J. A., Wolever T. M. S., Jenkins A. L., Thorne M. J., Lee R., Kalmusky J., Reichert R. and Wong G. S. (1983) The Glycaemic Index of Foods Tested in Diabetic Patients: A New Basis for Carbohydrate Exchange Favouring the Use of Legumes. Diabetologia, 24:257-264.
CrossRef - Brand J. C., Nicholson P. I., Thorburn A. W., and Truswell S. A. (1985) Food processing and the glycemic index. American Journal of Clinical Nutrition, 42: 1192-1196.
- Bornet F. R. J., Costagliola D., Saiwa W Rizkalla S. W., Blayo A., Fontvieille A.-M., Haardt M.-J., Letanoux M., Tchobroutsky G. and Slama G. (1987) Insulinemic and glycemic indexes of six starch-rich foods taken alone and in a mixed meal by type 2 diabetics. American Journal of Clinical Nutrition, 45:588-595.
- Krezowski P. A., Nuttal F. Q., Gannon M. C., Billington C. J. And Parker S. (1987) Insulin and glucose responses to various starch-containing foods in type II diabetic subjects. Diabetes Care, 10:205–212.
CrossRef - Wolever T. M. S., Katzman-Relle L., Jenkins A. L., Vuksan V., Josse R. G., and Jenkins D. J. A. (1994) Glycaemic index of 102 complex carbohydrate foods in patients with Diabetes. Nutrition Research, 14(5):651-669.
CrossRef - Soh N. L. and Brand-Miller J. (1999) The glycaemic index of potatoes: the effect of variety, cooking method and maturity. European Journal of Clinical Nutrition, 53: 249-254.
CrossRef - Fernandes G., Velangi A. and Wolever T. M. S. (2005) Glycemic index of potatoes commonly consumed in North America. Journal of the American Dietetic Association, 105: 557-562.
CrossRef - Aston L. M., Gambell J. M., Lee D. M., Bryant S. P., and Jebb S. A. (2008) Determination of the glycaemic index of various staple carbohydrate-rich foods in the UK diet. European Journal of Clinical Nutrition, 62: 279–285.
CrossRef - Leeman M., Ostman E. and Bjorck I. (2008) Glycaemic and satiating properties of potato products European Journal of Clinical Nutrition, 62: 87–95.
CrossRef - Ek K. L., Wang S., Copeland L. and Brand-Miller J. C. (2013) Discovery of a low-glycaemic index potato and relationship with starch digestion in vitro. British Journal of Nutrition, Oct 8:1-7, doi:10.1017/S0007114513003048.
CrossRef - Kanan W., Bijlani R.L. , Sachdeva U., Mahapatra S. C. , Shah P., Karmarkar M. G. (1998) Glycaemic and insulinaemic responses to natural foods, frozen foods and their laboratory equivalents. Indian Journal of Physiology and Pharmacology, 42(1):81-89.
- Hallfrisch J. and Behall K. M. (2000) Mechanisms of the effects of grains on insulin and glucose responses. Journal of the American College of Nutrition, 19: 320S-325S.
CrossRef - Wolever T. M. S. and Jenkins D. J. A. (1986) The use of the glycemic index in predicting the blood glucose response to mixed meals. American Journal of Clinical Nutrition, 43: 167-172.
- Le Floch J.-P., Escuyer P., Baudin E., Baudon D., and Perlemuter L. (1990) Blood Glucose Area Under the Curve. Methodological Aspects. Diabetes, 13 : 172-175.
CrossRef - Durnin J. V. G. A. & Womersley J. (1974) Body fat assessed from total body density and its estimation from skinfold thickness: measurements on 481 men and women aged from 16 to 72 years. British Journal of Nutrition, 32: 77-97.
CrossRef - American Diabetes Association (1969) Standardization of the Oral Glucose Tolerance Test Report of the Committee on Statistics of the American Diabetes Association. Diabetes, 18: 299-310.
CrossRef - Wolever T. M. S., Vorster H. H., Bjo¨rck I., Brand-Miller J., Brighenti F., Mann J. I., Ramdath D. D., Granfeldt Y., Holt S., Perry T. L., Venter C. and Wu X. (2003) Determination of the glycaemic index of foods: interlaboratory study. European Journal of Clinical Nutrition, 57: 475–482.
CrossRef - Brand-Miller J C, Stockmann K., Atkinson F., Petocz P., and Denyer G. (2009) Glycemic index, postprandial glycemia, and the shape of the curve in healthy subjects: analysis of a database of more than 1000 foods. American Journal of Clinical Nutrition, 89: 97-105.
CrossRef - International Standards Organisation (2010). Food Products –Determination of the Glycaemic Index (GI) and Recommendation for Food Classification. ISO 26642-2010. Geneva: International Organisation for Standardisation.
- Dinu V. T. (2014) The effect of frying on the molecular structure of potato starch. BSc Dissertation, University of Nottingham.





Web of Science Coverage
Emerging Sources Citation Index (ESCI)
2024 Journal Impact Factor: 1.1
Scopus Journal Metrics
CiteScore 2025: 2.6
CiteScore Details
Sustainable Nutrition: Food Systems, Nutrient Retention, and Public Health Impact
![]()
This journal is a member of, and subscribes to the principles of, the Committee on Publication Ethics (COPE)








