Aflatoxin Exposure in Pregnant Women in Kisumu County, Kenya
1Maseno University, P.O Box 3803-40100, Kisumu, Kenya
2Maseno University, School of Public Health and Community Development, Department of Nutrition and Health, P.O. Box 333, Maseno- Kenya
3Kenya Medical Research Institute (KEMRI), Centre for Global Health Research, Kisumu. P.O Box 1578, Kisumu, Kenya
4Kenya Agricultural Research Institute (KARI) P.O Box 450-30200, Kitale, Kenya.
Corresponding Author Email: mobade2002@yahoo.com
DOI : http://dx.doi.org/10.12944/CRNFSJ.3.2.06
Download this article as:
![]()
About 4.5 billion people globally and 1.8 million Kenyans are exposed to large amount of aflatoxin. However, little is known about aflatoxin exposure levels in pregnant women through dietary intake. This study aimed to determine levels of aflatoxin exposure of pregnant women in Kisumu County, where up to 40% households have been found to be exposed to the toxin. Assessment of aflatoxin in maternal diet may shed light on potential risk of exposure of their infants to the toxin. Between June and August 2013, we conducted a cross sectional study where aliquot samples of food consumed by 553 pregnant women of up to 8 months gestation, in the preceding 24 hours, were collected and analyzed for aflatoxin using ELISA technique. Aflatoxin levels in the foods consumed by the women ranged from 0 to 39.5 ppb. The proportion of women exposed to aflatoxin levels above the Kenya regulatory limit of 10 ppb was 24.8%, with 37.6% having daily absolute aflatoxin intakes ranging from 10µg to 150µg. Of the exposed women, 14.1% (n=26) were recruited from Kisumu East District Hospital, compared to 30.2% (n=111), from Ahero District Hospital (OR=2.64, 95% CI=1.65-4.23, p<0.0001); and 14.0% (n=25) were from Kisumu East District, compared to 30.1(n=111) from Nyando District (OR=2.7, 95% CI=1.6-4.3, p<0.0001 and 20% (n=1) from Kisumu West District (OR 1.5, 95% CI=0.2-14.3). Of the 93 households with monthly income of Kshs. ≤2000, 41.9% (n=39) were exposed to aflatoxin above 10 ppb compared to 24.8% (n=77), 16.5% (n=16) and 9.4% of those earning monthly income of, 2001-5000, (OR=0.46, 95% CI=0.282-0.744, p=0.002), 5001-10000 (OR=0.27, 95% CI=0.139-0.538, p<0.0001); and >10000 (OR=0.144, 95%CI=0.053-0.396) respectively. Pregnant women in Kisumu County are exposed to low-to-high levels of aflatoxin which may in turn expose their infants to the toxin. The effect of such exposure on health should be assessed and appropriate mitigation measures instituted.
KEYWORDS:Pregnant women; aflatoxin; exposed; non exposed; ELISA
Introduction
Aflatoxins are a group of mycotoxins produced by Aspergillus flavus and Aspergillus parasiticus species and are carcinogenic in nature .1 It is estimated that 4.5 globally have chronic exposure to large amounts of aflatoxin in their diets.2 The toxins contaminate a wide range of agricultural produce and products before harvest and under post harvest conditions.3 Some of the foods prone to aflatoxin contamination include cereals, legumes and spices. The toxins are also found in milk, eggs, and meat products due to consumption of contaminated feeds by animals [4]. Kisumu County may be prone to aflatoxin contamination because of the following reasons: some of the foods grown and consumed in the County are high risk commodities for aflatoxin contamination5; prevailing climatic conditions in Kisumu County including drought, erratic rainfall (1200 mm and 1300 mm); high temperatures ranging between 20oc and 35oc and high humidity (40-89%), provide a favorable environment for growth of mould and production of aflatoxins.6 A recent study carried out in Kisumu County reported aflatoxin levels above 10 ppb in samples of maize, sorghum and groundnuts with sorghum having the highest median (IQR) of 14.2 (8.5, 19).7 Consumption of food contaminated with aflatoxin is of public health importance because of its effect on human health and food safety,8 and Kisumu County may be prone to low and high levels of aflatoxin exposure through dietary intake.
At least 14 different types of aflatoxins are produced in nature9 and aflatoxin B1 is considered the most toxic and most potent [10,11]. Aflatoxin AFM1, the hydroxylated metabolite of AFB1, is detected in milk 12-24 hours after ingestion12 and poses a health risk to breast-fed infants.13,14 Both AFM1 and AFB1 have been found in breast milk samples from Ghana and Nigeria.15 Human exposure to aflatoxins therefore begins early in life and a correlation has also been demonstrated between aflatoxin exposure in utero and growth faltering in infants.16 Consequently, exposure of pregnant women to aflatoxin poses a health risk not only to the women, but also to the developing fetus and the breastfeeding infant.
Aflatoxin poisoning resulting from consumption of contaminated maize has been reported yearly in Eastern Kenya, the worst having occurred in 2004.7 Contamination levels of 133 to 376 times above the Kenyan regulatory limit of 10 ppb have also been reported in peanut-growing areas in South Nyanza and 40% of food samples from farmers in the region had aflatoxin levels above the regulatory limit of 10 ppb.6 Although the Eastern region of Kenya is known to be most prone to outbreaks of aflatoxicosis, mean aflatoxin levels of 37ppb and 54ppb have been found in maize in Homa Bay and Rongo compared to 21ppb, 25ppb and 44ppb in Makueni, Mbeere North and Mbooni East respectively,9 indicating that similar and even higher levels of aflatoxin occur in foods in Nyanza region. In a cross sectional study to determine levels of aflatoxins in market foods, aflatoxin B1 levels in market foods ranged from 0 to 34.5 ppb and aflatoxin M1in milk samples ranged from 0.0002 to 0. 13 ppb.7
Most studies assessing associations between aflatoxin exposure and health have involved chronic exposure of much lower levels of aflatoxin, which have been implicated in poor health outcomes.11,12,13 Chronic exposure to levels of aflatoxin could pose more serious health problems than the outbreaks of aflatoxicosis which leads to sudden death. This is because of its potential to increase the risk for conditions such as cancer and growth faltering in children, which take a long time to manifest due to long latency periods; but impose an immense burden on health care costs and quality of life.13 Cancer ranks third among the causes of deaths in Kenya, accounting for 18,000 deaths annually (7% of all deaths) and liver cancer, associated with aflatoxin exposure, is one of the most common forms of cancer among Kenyan men.17 Aflatoxin exposure has also been implicated in speeding up rapid progression of HIV to AIDS due to aflatoxin-related immunosuppression.18 According to data from KDHS, 2008/2009, Kisumu is one of the Counties in Nyanza region with high HIV and AIDS prevalence.19
Exposure to aflatoxin affects micronutrient availability for body functions, and influences the incidence of aflatoxin related adverse health effects.20 Further, vitamin A and E supplementation significantly reduces aflatoxin induced toxicity and carcinogenesis, compromising the intended purposes of the nutrients.21,22 Aflatoxin exposure may also have an effect on availability of dietary zinc and selenium, which have antioxidant properties and are also essential for healthy immune function.23 Exposure to aflatoxin may therefore affect the availability of micronutrients for body functions resulting in poor health outcomes.
In Benin an inverse correlations was observed between maternal aflatoxin exposure and height-for age and weight-for height z-scores (HAZ and WAZ) in children; and AFM1 levels in maternal breast milk and HAZ in infants 90–120 days old.24 However, these associations were reported in children more than 3 months old. In a similar study, it was noted that children whose mothers were AFM1 positive had lower HAZ and WAZ.25 These findings reveal that maternal aflatoxin exposure may affect infant’s growth in utero as well as through breast milk. Studies have established that a reduction of maternal aflatoxin albumin adducts (AF-alb) from 110 pg/mg to 10 pg/mg would lead to a 0.8 kg increase in weight and 2 cm increase in height within the first year of life.16 This further supports the negative effect of aflatoxin exposure on weight and height in young children.
There is limited information available on exposure of pregnant women to aflatoxins. Assessment of aflatoxin in maternal diet, the main source of adult exposure to aflatoxin, may shed light on potential risk of exposure of their infants to the toxin. Assessment of aflatoxin levels in foods consumed by the mother is a one way of determining whether the foetus or the young child is exposed to the toxin. Studies assessing effect of aflatoxin on growth in children have mainly focused on the weaning period, with few addressing risk of infant exposure through maternal exposure.
This study aimed to investigate the exposure of pregnant mothers to aflatoxin contamination through diet in Kisumu County, Kenya, as an indicator of potential exposure of their infants to aflatoxin by: determining aflatoxin levels in foods consumed by the women; determining absolute amounts of aflatoxin consumed by the women in one day; determining the proportion of pregnant women exposed to aflatoxin levels above 10 ppb and assessing the association between socio-demographic factors and aflatoxin exposure.
Material and Methods
This was a cross sectional survey study conducted in Kisumu East and Nyando Districts, Kisumu County, Kenya. Ethical approval to conduct the study was granted by the Maseno University Ethics Review Committee. The study population included 553 pregnant women attending antenatal clinics, 185 from Kisumu East District and 368 from Ahero District Hospitals, respectively. All the subjects gave written informed consent to participate in the study.
Pregnant women were recruited and screened at the antenatal clinics at Kisumu East and Ahero District Hospitals. Community Health Workers assisted with the recruitment of pregnant women of up to the 8th month of pregnancy who were screened for eligibility to participate in the study. The women were eligible for inclusion into the study if they consented to participate in the study; were up to 8 months pregnant and resided in Kisumu County, Kenya. Aliquot samples of 10% of the foods eaten over 24 hours in a day by each woman were collected over a period of 3 months by trained Community Health Workers, kept in cooler boxes whilst in the field and stored in a -20oC freezer for two weeks before being taken to KARI Kitale laboratory for chemical analysis of aflatoxin levels. A survey questionnaire was used to collect basic data on socio-demographic characteristics, mother’s diet over the preceding 24 hours, and the daily, weekly, and monthly frequency of food consumption.
Aflatoxin B1 levels in food samples were analyzed using HELICA Total Aflatoxin Assay, a competitive Enzyme Linked Immunosorbent Assay (ELIZA) used for quantitative detection of aflatoxin B1, B2, G1 and G2 in foods. An aflatoxin specific antibody optimized to cross reacts with Aflatoxin B1, B2, G1 and G2, was coated to a polystyrene microwell. Toxins were extracted from a ground sample of 20g portion and 100 mls of 70% methanol. The extracted samples and hydrogen peroxidase preservative conjugate (HRP) Aflatoxin B1 were mixed and added to the antibody coated microwell. Microwell contents were decanted and nonspecific reactants were removed by washing. An enzyme substrate was added and the colour blue developed. The intensity of the color was directly proportional to the amount of bound conjugate and inversely proportional to the concentration of aflatoxin in the sample or standard. However, the sample had been diluted at a ratio of 5 to 1 with 70% methanol; therefore the aflatoxin shown by the standard was multiplied by 5 in order to indicate the ng of aflatoxin per gram of commodity (ppb).
Aflatoxin intake by women through diet was determined by aflatoxin levels in the aliquot foods samples collected from participants and analyzed at KARI Kitale. Absolute aflatoxin (µg) intake by pregnant women in a day was calculated using the formula:
Absolute aflatoxin (µg) = Amount of aflatoxin in analyzed food x Total
amount of food consumed in a day.26
Data were analyzed using Statistical Package for Social Sciences (SPSS) software (IBM SPPS Statistics®), a p value < 0.05 was considered statistically significant. Data were first assessed for normality using frequencies and histograms. Independent sample T-Tests were used to compare means of continuous variables between exposed and non exposed mothers. Chi Square Tests, Fishers Exact Tests were used to assess association between socio demographic characteristics and exposure. Descriptive analyses involved reporting of frequencies for categorical variables and median (with interquartile range [IQR] for continuous variables.
Results
Participants were recruited from two districts; 185 participants (33.5%) from Kisumu East District and 368 participants (66.5%) from Nyando District. Majority of the participants (83.2%) were aged between 15 – 19 years, with a mean age of 24.6 ± 5.2. Most households comprised of 1 to 6 people (91.1%). Eighty one percent of the mothers were married and a big proportion had either primary (55.4%) or secondary (37.4%) level of education. The major sources of income were business (49.7%) and husband (23.3%), with most of the households having a monthly earning of Kshs.2001- 5000 (56.1%).
Aflatoxin levels in participants’ food ranged from 0 ppb to 39.5 ppb with most samples (75.2%, n=416) having levels ranging from 0 ppb to 9 ppb (Table 1). The highest range of aflatoxin contamination level; 10 ppb to 39.5 ppb was found in 24.8% of the food samples. The highest level of exposure (>8.75 ppb, n=138, 25%) were in the 4th quartile (Table 2); and 62.5% of the women had daily absolute aflatoxin intake of 0 µg to < 10 µg, while 37.5% had daily absolute aflatoxin intake ranging from 10 to 150 µg (median 5.14 µg) (Table 3). Of the exposed women, 14.1% (n=26) were recruited from Kisumu East District Hospital, compared to 30.2% (n=111) from Ahero District Hospital (OR=2.64, 95% CI=1.65-4.23, p<0.0001); and 14.0% (n=25) were from Kisumu East District, compared to 30.1(n=111) from Nyando District (OR=2.7, 95% CI=1.6-4.3, p<0.0001 and 20% (n=1). from Kisumu West District (OR 1.5, 95% CI=0.2-14.3). Of the 93 households with monthly income of Kshs. ≤2000, 41.9% (n=39) were exposed to aflatoxin above 10 ppb compared to 24.8% (n=77), 16.5% (n=16) and 9.4% of those earning monthly income of 2001-5000, (OR=0.46, 95% CI=0.282-0.744, p=0.002), 5001-10000 (OR=0.27, 95% CI=0.139-0.538, p<0.0001); and >10000 (OR=0.144, 95%CI=0.053-0.396) respectively (Table 5). Based on multivariate analysis, the predictor of aflatoxin exposure was monthly household income, p<0.05 (Table 6).
Table 1: Aflatoxin levels in participants meals
| Variable Description | % (N) |
| Aflatoxin levels (ppb) | |
|
75.2 |
|
5.9 |
|
18.9 |
|
2.0 (1.0, 8.8) |
| Exposed to aflatoxin levels above 10 ppb | 24.8 (137) |
| Not exposed to aflatoxin levels above 10 ppb | 75.2 (416) |
A big proportion of the participants’ meals had aflatoxin levels ranging from 0 ppb to 9 ppb and 24.8% of the participants’ meals had aflatoxin levels above 10 ppb
Table 2: Aflatoxin exposure by Quartiles
| Quartile | Aflatoxin range (ppb) | Frequency (n) | % |
| Quartile 1 | 0 – 0.9 | 105 | 19 |
| Quartile 2 | 1.0 – 1.9 | 128 | 23.1 |
| Quartile 3 | 2.0 – 8.75 | 182 | 32.9 |
| Quartile 4 | > 8.75 | 138 | 25.0 |
The highest level of exposure (>8.75 ppb, n=138, 25%) was in the 4th quartile.
Table 3: Daily total aflatoxin intake by Pregnant mothers in µg
| Aflatoxin intake range (µg) | No of women | % |
| 0 – 9 | 345 | 62.5 |
| 10 – 19 | 44 | 8 |
| 20 – 39 | 61 | 11.1 |
| ≥ 40 | 100 | 18.5 |
Majority of the pregnant women had absolute daily aflatoxin intake of 0-9 ppb, while 37.5% had absolute daily aflatoxin intake ranging from 10 ppb to ≥ 40 ppb.
Table 4: Projected risk for liver cancer attributed to intake of aflatoxin M1 in milk (Henry et al., 2001)
| Aflatoxin M1 intake in ng/person per day | Prevalence of liver cancer attributable to aflatoxin M1 (cancer cases/ year per 106) |
| 6.8 | 1.5 |
| 15 | 20 |
| 150 | 200 |
Consumption of 150 ng of aflatoxin M1 per person per day would translate to prevalence of 200 liver cancer cases per year per 106 people
Table 5: Association between aflatoxin exposure and socio-demographic factors
| Variables |
n |
Exposed n (%) |
Not exposed n (%) |
Crude Odds Ratio[95%CI] |
p-value |
|
Age categories |
|||||
|
15-19 20-24 25-29 30-34 35-39 40-44 |
96 209 156 64 23 5 |
25(26.0) 63(30.1) 35(22.4) 6(9.4) 7(30.4) 1(20.0) |
71(74.0) 146(69.9) 121(77.6) 58(90.6) 16(69.6) 4(80.0) |
Ref 1.22[0712-2.110] 0.821[0.445-0.483] 0.294[0.113-0.764] 1.243[0.458-3.372] 0.710[0.076-6.657] |
0.463 0.514 0.012 0.670 0.764 |
| Health facility | |||||
| KisumuAhero |
185 368 |
26 (14.1%) 111(30.2%) |
169 (85.9) 257 (69.8) |
Ref 2.64 [1.65, 4.23] |
0.0001 |
|
District of residence |
|||||
|
Kisumu East Nyando Kisumu west |
179 369 5 |
25 (14.0%) 111(30.1%) 1(20.0%) |
154 (86.0) 258 (69.9) 4 (80.0) |
Ref 2.7 [1.6-4.3] 1.5 [0.2-14.3] |
0.0001 0.705 |
| Marital status | |||||
| SingleMarriedSeparatedDivorced |
93 448 5 2 |
22 (23.7%) 113 (25.1%) 1 (20.0%) 1 (50.0%) |
71 (76.3) 335 (74.8) 4 (80.0) 1 (50.0) |
Ref 1.1 [0.6-1.8] 0.8 [0.09, 7.6] Excluded |
0.750 0.851 |
| Educational level | |||||
| NonePrimarySecondaryCollegeUniversity |
2 306 207 28 10 |
1 (50.0%) 82 (26.8%) 47 (22.7%) 5 (17.9%) 2 (20.0%) |
1 (50.0) 224 (73.2) 160 (77.3) 23 (82.1) 8 (80.0) |
Ref 0.37 [0.023-5.920 0.29 [0.18-4.786] 0.22 [0.120-4.094] 0.25 [0.100-5.985] |
0.48 0.390 0.308 0.392 |
| Occupation | |||||
| HousewifeSelf employedEmployedOther |
153 300 39 61 |
39 (25.5%) 76 (25.3%) 8 (20.5%) 14 (23.8%) |
114 (74.5) 224 (74.7) 71 (79.5) 47 (77.0) |
Ref 0.992[0.634-1.551] 0754 [0.320-1.779] 0.87 [0.430-1.750] |
0.971 0.520 0.698 |
| Religion | |||||
| ChristianMuslim |
551 2 |
136 (24.7%) 1 (50.0%) |
415 (75.3) 1 (50.0) |
Ref 0.33 {0.20-5.28] |
0.434 0.431 |
| Source of income | |||||
| FarmingEmployedBusinessHusbandParentsSiblings |
57 48 276 129 42 7 |
14 (27.5%) 10 (20.8) 70 (25.4%) 31 (24.0%) 12 (28.6%) 0 (0.0%) |
37 (72.5) 38 (79.2) 206 (74.6) 98 (76.0) 30 (71.4) 7 (100.0) |
Ref 0.70 [0.28-1.76] 0.90 [0.46-1.76] 0.84 [0.40-1.75] 1.00 [0.43-2.62] Exclude |
0.444 0.754 0.633 0.905 |
|
Household monthly earnings Kshs) |
|||||
|
≤2000 2001-5000 5001-10000 >10000 |
93 310 97 53 |
39 (41.9%) 77 (24.8%) 16 (16.5%) 5 (9.4%) |
54 (58.1) 233 (75.2) 81 (83.5) 48 (90.6) |
Ref (1.0) 0.46[0.282-0.744] 0.27 [0.139-0.538] 0.144[0.053-0.396] |
0.002 0.0001 0.0001 |
Women attending antenatal clinic at Ahero District Hospital, those residing in Nyando District and those with monthly income ≤2000 were exposed to aflatoxin above 10ppb
Table 6: Predictors of aflatoxin exposure
| Variables | n | Exposedn (%) | Not exposedn (%) | Crude Odds Ratio[95%CI] | p-value |
| Health facility | |||||
| KisumuAhero |
185 368 |
26 (14.1%) 111(30.2%) |
169 (85.9%) 257 (69.8%) |
Ref (1.0) 2.24[0.126-9.894] |
0.583 |
|
District of residence |
|||||
|
Kisumu East Nyando Kisumu west |
179 369 5 |
25 (14.0%) 111(30.1%) 1(20.0%) |
154 (86.0%) 258 (69.9%) 4 (80.0%) |
Ref (1.0) 0.92 [0.052-16.448] 1.24[0.121-12.727] |
0.982 0.956 0.856 |
| Household monthly earnings (Kshs) | |||||
| ≤20002001-50005001-10000>10000 |
93 310 97 53 |
39 (41.9%) 77 (24.8%) 16 (16.5%) 5 (9.4%) |
54 (58.1%) 233 (75.2%) 81 (83.5%) 48 (90.6%) |
Ref (1.0) 0.510[0.311-0.837] 0.353[0.175-0.711] 0.198[0.071-0.556] |
0.002 0.008 0.004 0.002 |
The main predictor of aflatoxin exposure in Kisumu County by multivariate analysis was household monthly income, P<0.05.
Discussion
The findings of this study indicate that at aflatoxin levels in foods consumed by pregnant women in Kisumu County, exposure ranged from as low as 0 ppb to as high as 39.5 ppb per day. A regulatory limit of aflatoxin levels of 10 ppb is in force in Kenya. However, concern on aflatoxin mainly focuses on exposure to very high levels of contamination as occurs during aflatoxicosis outbreaks, and reflected by most studies on contamination having been carried out in Eastern Province, an area that is assumed to have highest levels of exposure.
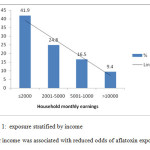 |
Figure 1: exposure stratified by income Higher income was associated with reduced odds of aflatoxin exposure. Click here to View figure |
The results of the analysis of cooked food consumed by pregnant women showed detectable levels of aflatoxin in most food samples. The results of aflatoxin in a combination of foods consumed by participants in a day indicate aflatoxin intake ranging from 0 to 39.5 ppb, Median (IQR) 2.0 (1.0,8.8). This range includes aflatoxin levels above maximum tolerable set limits in human food by Kenya and the international community. The Kenya Bureau of Standards recommends 10 ppb as the maximum permissible level of aflatoxin,27 while Codex Alimentarius recommends aflatoxin allowable limit of 9 ppb.28 The European Union has some of the strictest standards for aflatoxin and has set the upper limit of aflatoxin for foods destined for European market at 4 ppb.6 It is expected that the levels could have been higher if raw foods had been analyzed. Analysis of aflatoxin in prepared rather than raw foods has been considered the most reliable source for determining aflatoxin exposure since most grains are sorted out and unfit parts removed before preparation.8 In an earlier study carried out in market foods in Kisumu County, aflatoxin levels in selected food samples ranged from 0 to 34.5 ppb.7 A combination of these foods would result in higher absolute daily food intake and higher levels of exposure.
The results of this study further indicate that 24.8% of pregnant women in Kisumu County consume food with aflatoxin levels above the recommended Kenyan regulatory limit of 10 ppb (Table 1). If extrapolated to the entire population, the implication is that a large proportion of the population in Kisumu County has detectable levels of aflatoxin in their meals. This indicates exposure to both low to high levels of aflatoxin through cooked foods, which has been associated with negative health outcomes. Exposure of pregnant women shows the potential for exposure of the fetus and the infant through utero and breast milk intake. According to the Kenya Demographic and Health Survey 2008-09 (KNBS & ICF Macro, 2010), Nyanza region has a median duration of breastfeeding of 18.6 months and 0.6 months of exclusive breastfeeding. This supports exposure of infants of exposed mothers to aflatoxin through breast milk intake.
Amount of aflatoxin consumed by each woman in one day was determined from the levels of aflatoxin in food analyzed and the quantity of food consumed.29 Based on the results of aflatoxin analysis of foods consumed by the women, 37.6% of the pregnant women had daily absolute aflatoxin intake ranging from 10 µg to 150 µg per day. These figures are higher than the findings from the study carried out in The Gambia, West Africa, where subjects were exposed to aflatoxin originating from several foods with an intake ranging from 0 to 29 µg/day.30 Wild’s study supported a positive correlation between dietary aflatoxin intake and levels of aflatoxin-albumin adducts in the blood. This implies that there is a potential risk of aflatoxin exposure in pregnant women in Kisumu County since both low and high aflatoxin levels have been associated with negative health outcomes. For instance, Aflatoxin M1 intake of 6.8 ng, 15 ng and 150 ng per person per day have been associated with 1.5, 20 and 200 cancer cases per 1million people per year.26 Aflatoxin B1 found in most solid food is more toxic and more potent than aflatoxin M1. Data from our literature review reveal an upward trend in cancer cases both in adults and young children in Kenya.17 It is important to note that both the set limits of aflatoxin by Codex Alimentarius and the Kenyan limit may mean nothing to most people in Kenya and in Kisumu County because of food insecurity.
The results of this study showed a strong association between health facility, district of residence, household monthly earnings and exposure to aflatoxin levels above 10 ppb, p<0.0001. Women attending antenatal clinic at Ahero District Hospital were more likely to be exposed to aflatoxin levels above 10 ppb compared to those attending antenatal clinic at Kisumu District Hospital, OR=2.64, 95% CI=1.65-4.23, p<0.0001). Further, women residing in Ahero District were more likely to be exposed to higher aflatoxins compared to their counterparts leaving in Kisumu District, OR=2.7, 95% CI=1.6-4.3, p<0.0001 and Kisumu West District OR 1.5, 95% CI=0.2-14.3. This could be due to the location, as well as different environmental and weather conditions prevailing in the two sites. Kisumu District Hospital is situated within Kisumu City and could have the advantage of access to quality food. However, Ahero District Hospital is situated in the rural setup of Nyando District, which is prone to extreme weather conditions characterized by frequent floods and drought. These conditions have been found to be conducive to mould infestation and production aflatoxins.2,6,5 Households with lower household income were more likely to be exposed to aflatoxins compared to those with higher household income, p<0.0001. People with lower income are likely to consume contaminated food because of food insecurity and high poverty levels. Poor people may not have the luxury of choosing quality foods because of economic constraints. There was no evidence of any relationship between marital status, education level, occupation, religion, source of income, age and aflatoxin exposure, p>0.05.
Our analyzed cooked foods constituted participants’ one day’s meal. Due to interindividual variations in daily food intake, the amount of aflatoxin consumed through diet might not have been determined with high degree of accuracy. In addition, food samples were collected between the month of June and August 2013. This is normally the period when food harvesting is taking place in Kisumu County. Aflatoxin contamination has been reported to increase with storage time. In a study carried out in the Gambian children, aflatoxin albumin adduct concentration was strongly influenced by the month of sampling.23 Groundnuts, one of the foods known to be susceptible to aflatoxin contamination, and one of the major foods consumed in Kisumu County, is normally planted during the short rains season, August to October and harvested in December. This commodity was scarce in the market during the time of data collection, resulting in low consumption at household levels. It is assumed that aflatoxin levels could have been higher if groundnuts were in the households at the time of data collection.
Pregnant women and their infants, as well as the larger community in Kisumu County are potentially exposed to both low and high levels of aflatoxin contamination through dietary intake. Intervention measures to reduce exposure to the toxin merits investigation. Public information campaigns on aflatoxin management and prevention should be conducted in Kisumu County and the entire nation of Kenya. Appropriate measures should be instituted to reduce exposure to aflatoxin and its effects on the health of pregnant women, young children and the entire community. A comprehensive study should be undertaken during different seasons to determine seasonal variations, to give a clearer overview of aflatoxin contamination in Kisumu County.
Acknowledgements
Special tribute to my supervisors: Dr. Pauline Andang’o; Prof. Charles Obonyo and Dr. Francesca Lusweti for their dedication, patience and encouragement. The authors highly appreciate the Kenya Agricultural Research Institute (KARI) Kitale for the special role in aflatoxin analysis of the food samples. We appreciate East Africa Agricultural Productivity Project (EAAPP) for funding part of the research project. Many thanks to Mr. Vincent Were, from KEMRI, Kisumu for his input on statistical analysis. The authors owe a lot of gratitude to the management of Kisumu and Ahero District Hospitals for availing their facilities for the study. Special thanks to all the research assistants for their devotion and patience in recruitment of participants and collection of food samples. We salute all the pregnant women who gave their consent to participate in the study.
References
- Lee N.A., Wang S., Allan D.R. & Kennedy I.R A rapid aflatoxin B1 ELISA. Development and validation with reduced matrix effects for peanut, corn, pistachio and soybeans. J. Agriculture. Food Chem, 2004; 52, 2746 – 2755.
CrossRef - Centre for Disease Control (CDC) Outbreak of aflatoxin poisoning—Eastern and Central Provinces, Kenya, 2004.
- Muthomi J.M, Njenga, L.N, Gathumbi J.K. and Chemining’wa G.N The Occurrence of Aflatoxin in Maize and Distribution of Mycotoxins-Producing Fungi in Eastern Kenya. Plant Pathology Journal, 2009; 8 (3): 113-119.
CrossRef - Lunyasunya T.P., Wamae L.W., Musa H.H., Olowafeso O. and Lokwaleput I.K The risk of mycotoxins contamination of dairy feed and Milk on smallholder dairy farms in Kenya. Pakistan Journal of Nutrition. Pakistan Journal of Nutrition, 2005; 4 (3): 162-169.
CrossRef - MoA The Role of Post Harvest Technology in the Control of aflatoxins in Cereals And Pulses: Ministry of Agriculture, Nairobi, Kenya, 2010
- Mutegi C.K., Hendricks S.L., Jones R.B., Okello J.J. and Ngugi H.K Role of collective action and handling practices on aflatoxin contamination of groundnuts. Paper presented at the African Crop Science Conference Proceedings, 2007.
- Obade M.I., Andang’o P., Obonyo C., Lusweti F Exposure of children 4 to 6 months of age to aflatoxin in Kisumu County, Kenya. African Journal of Food, Agriculture, Nutrition and Development, 2015; 15 (2), 9949 – 9963
- Williams J.H., Phillips T.D., Jolly P.E., Stiles J.K., Curtis M. and Jolly C.M Human aflatoxicosis in developing countries: A review of toxicology, exposure, potential health consequences, and interventions. American Journal of Clinical Nutrition, 2004; 80:1106-1122.
- Reiter E., Zentek J. and Razzazi E Review on sample preparation strategies and methods used for the analysis of aflatoxins in food and feed. Mol. Nutr. Food Res, 2009;
CrossRef - Keskin Y., Baskaya R., Karsli S. and Yurdun T Detection of aflatoxin M1 in human breast Milk and raw cow’s Milk in Istanbul, Turkey. Journal of Food Protection. Journal of Food Protection, 2009; 72(4): 885–889.
CrossRef - Omer R.E., Verhoef L., Vant Veer P., Idris O.M., Abdelgadir M.Y., Kadaru M. Y., et al. Peanut butter intake, GSTM1 genotype and hepatocellular carcinoma: a case – control study in Sudan. Cancer Causes and Control, 2001;12, 23-32.
CrossRef - Sadeghi N., Oveisi M.R., Jannat B., Hajimahmood M., Boyani H. and Jannat F Incidence of aflatoxin M1 in human breast Milk in Tehran, Iran. Food Control, 2009; 20, 75-78.
CrossRef - Antonius E., Wagenaar E.L.S., Karnekamp B., Merino G., Jonker J. and Schinkel F. A Breast cancer resistance protein (Bcrp1/Abcg2) reduces systemic exposure of the dietary carcinogens aflatoxin B1, IQ and Trp-P-1 but also mediates their secretion into breast Milk. Division of Experimental Therapy, the Netherlands Cancer Institute, 1066 CX Amsterdam, 2005.
- Galvano F., Pietri A., Bertuzzi T., Gagliardi L., Ciotti S., Luisi S., et al. Maternal dietary habits and mycotoxin occurrence in human mature Milk. Mol. Nutr. Food Res, 2008; 52: 496-501.
CrossRef - Gürbay A., Sabuncuog˘lu S.A., Girgin G.S., Yig˘it S. and Yurdakok M Exposure of newborns to aflatoxin M1 and B1 from mothers’ breast Milk in Ankara, Turkey. Food and Chemical Toxicology, 2010; 48: 314-319.
CrossRef - Turner P.C., Collinson A.C., Cheung Y.B., Gong Y., Hall A.J., Prentice A.M., et al. Aflatoxin exposure in utero causes growth faltering in Gambian infants. Int J Epidemiol, 2007; 36: 1119-1125.
CrossRef - National Cancer Control Strategy (NCCS) 2011-2016. Ministry of Public Health and Sanitation (MoPHS). Nairobi, Kenya
- Turner P.C., Moore S.E., Hall A.J., Prentice A.M. and Wild C.P Modification of immune function through exposure to dietary aflatoxin in Gambian children. Enviro Health Perspect, 2003; 111 (2), 217-220.
CrossRef - KNBS & Macro Kenya Demographic and Health Survey 2008-09. Calverton, Maryland: KNBS and ICF Macro, 2010.
- Tang L., Xua L., Afriyie-Gyawub E., Liua W., Wanga P., Tanga Y., et al. Aflatoxin–albumin adducts and correlation with decreased serum levels of vitamins A and E in an adult Ghanaian population. Food Additives and Contaminants, 2009; 26 (1): 108-118.
CrossRef - Alpsoy1 L., Yildirim A., and Agar G The antioxidant effects of vitamin A, C, and E on aflatoxin B1-induced oxidative stress in human lymphocytes. Toxicology and Industrial Health, 2009; 25, 121-127.
CrossRef - Verma R.J., Shukla R.S., and Mehta D.N Amelioration of cytotoxic effects of aflatoxin by vitamin A: an in vitro study on erythrocytes. Toxicol In Vitro, 2001; 15: 39-42.
CrossRef - Mocchegiani E., Corradi A., and Santarelli L. et al. Zinc, thymic endocrine activity and mitogen responsiveness (PHA) in piglets exposed to maternal aflatoxicosis B1 and G1. Vet Immunol Immunopathol, 2001; 62, 245-260.
CrossRef - Gong Y.Y., Hounsa A., Egal S., Turner P.C., Sutcliffe A.E., Hall A.J. et al. Post weaning exposure to aflatoxin results in impaired child growth: a longitudinal study in Benin, West Africa. Environ. Health Perspect, 2004; 112, 1334-1338.
CrossRef - Mahdavi R., Nikniaz L., Arefhosseini S.R., and Vahed J.M Determination of aflatoxin M1 in breast Milk samples in Tabriz-Iran. Matern Child Health J, 2010; 14, 141-145.
CrossRef - Henry S.H., Bosch F.X., Bowers J.C Aflatoxin, hepatitis and worldwide liver cancer risks. Adv Exp Med Biol, 2002; 504: 229 –233.
CrossRef - Kenya Bureau of Standard, KEBS The Benchmark. The official magazine of Kenya Bureau of Standards, Issue 19, July 2013
- Codex Alimentarius Discussion and possible opinion on a draft commission regulation amending regulation (EC) No. 466/ 2001 as regards aflatoxins and ochratoxin A in foods for infant and young children (SanCO/0983/2002 REV.6), 2004.
- Gong Y.Y., Cardwell K., Hounsa A., Egal S., Turner P.C., Hall A.J. et al. Dietary aflatoxin exposure and impaired growth in young children from Benin and Togo: cross sectional study. Br. Med. J, 2002; 325, 20-21.
CrossRef - Wild C.P., Hudson G.J., Sabbioni G., Chapot B., Hall J.A., Wogan N.G et al. Dietary intake of aflatoxins and the level of albumin-bound aflatoxin in peripheral blood in The Gambia, West Africa Cancer Epidemiol Biomarkers Prev, 1992; 1, 229-234.





Web of Science Coverage
Emerging Sources Citation Index (ESCI)
2024 Journal Impact Factor: 1.1
Scopus Journal Metrics
CiteScore 2025: 2.6
CiteScore Details
Sustainable Nutrition: Food Systems, Nutrient Retention, and Public Health Impact
![]()
This journal is a member of, and subscribes to the principles of, the Committee on Publication Ethics (COPE)








