Nutritional Status and Dietary Habits of Subjects with Urolithiasis
Department of Studies in Food Science and Nutrition, University of Mysore, Manasagangothri, Mysore 570 006, India.
DOI : http://dx.doi.org/10.12944/CRNFSJ.3.1.06
Download this article as:
![]()
The lifestyle, environmental factors, nutritional status and dietary habits of patients with Urolithiasis, visiting the major hospitals in Mysore city was studied. The mean age of onset of the disease was > 20 y. A higher incidence was found in men belonging to younger age group. Subjects exhibited a positive urinary tract infection, difficult urination and pain. Somatic assessment indicated a low protein status. Urea, creatinine and other biochemical parameters were within the normal range for majority of subjects. Subjects were involved in heavy activity as they were agricultural laborers. Dietary were mixed types, with the cereals being the predominant items of the daily meals. Consumption of green leafy vegetables/ fruits was very low. The energy intake was lower than RDA. Higher intake of finger millet and horsegram, which are rich sources of calcium, oxalate and dietary fiber, and low fluid intake was reported by the subjects. Research is needed to identify risk factors specific to different geographical regions.
KEYWORDS:urolithiasis; somatic status; biochemical profile; food habits; nutrient intake
Introduction
Urinary stones have afflicted human kind since antiquity, with the earliest recorded example being bladder and kidney stones detected in Egyptian mummies dated to 4800 B.C. The specialty of urologic surgery was recognized even by Hippocrates, who wrote, in his famous oath for the physician “ I will not cut, even for the stone, but leave such procedures to the practitioners of the craft”.1 A dramatic rise in incidence of calcium stones of the kidney within the last 100 years has been observed. The overall incidence and pattern of idiopathic stone disease in different countries is found to relate to their economic development. In developed countries like India, Thailand, Turkey and other South East Asian countries, a high incidence of childhood bladder stone disease is observed. On the other hand, in industrialized countries like UK, USA, Japan etc., ‘modern pattern’ of stone disease in adults is more common.2 The urinary stone of history was the Idiopathic bladder stone – a childhood problem predominantly afflicting the male. It was quite common in Western Europe and England some hundreds of years ago, now it is a rarity in Western world. However, it still occurs in the “endemic stone areas” Northeast Thailand, Indonesia, Northwest India, Middle East and Egypt.3 Idiopathic urolithiasis is a multi-factorial disease. Its genesis is influenced by extrinsic factors such as climate, diet, economic status and fluid intake. The intrinsic factors identified are age, gender, ethnic background and genetic predisposition.2,4,5 There are well recognized physico-chemical factors in respect of stone formation associated with increased excretion rates of calcium, oxalate and uric acid. Evidence from metabolic studies of idiopathic stone formers implicate that the diet typical of the affluent westernized countries increases the likelihood of calcium oxalate crystallization in the urine and decreases the activity of urinary inhibitors.3,6 The calculogenic dietary risk factors are of 2 types – those arising out of dietary excess and those due to dietary deficiencies or under nutrition. The prevailing pattern of urolithiasis in different regions of the world appears to depend upon the nature of malnutrition.7 Several dietary factors have been implicated in the incidence of urinary stones viz., animal protein, calcium, sugar and dietary fiber.3,4 Several studies have demonstrated a significant increase in urinary excretion rates of calcium, oxalate and uric acid. These three products are all known risk factors for the formation of calcium -containing stones. Several reports on chemical analysis of renal stones are available from different endemic regions in India.8-11 Various studies from India have also documented that calcium oxalate forms the major constituent of urinary calculi.12
However, no information is available on the nutritional status and dietary habits of patients afflicted with renal stones. Therefore, the present study was planned to evaluate the lifestyle and environmental factors, food habits of persons afflicted with urolithiasis and to assess the dietary status, by using somatic measurements, biochemical parameters and food intake data.
Methodology
A total of 130 patients in the age range of 18-75 yrs admitted ad the hospitals during the study period, with urolithiasis, were selected with help of the attending urologist. The duration of their stay at the hospital ranged from 3-6 days. Detailed enquiries about past and present complaints, personal and other habits and about the family disease history were made using a formatted questionnaire schedule. Personal histories on habits such as smoking and alcohol consumption were also elicited.
Biochemical Investigation: Biochemical tests such as hemoglobin, Blood urea, glucose, Blood creatinine and urinary albumin and urinary glucose carried out routinely at the hospitals were also recorded in the questionnaire. The above mentioned biochemical tests were measured using standard diagnostic methods in all the hospitals. Hemoglobin was measured by the cyanomethemoglobin method.13 Blood glucose, urea, creatinine and urinary albumin were estimated using standard methods.14-17
Anthropometric Measurements: Body weight was checked to the nearest, 100g standard balance in light clothing and without shoes. Mid upper arm circumference (MUAC) is taken on the left hand, using a non-stretchable measuring tape. The reading was taken to the nearest millimeter. Skin fold measurements, to the nearest 0.2 mm were made using Lange skin fold calipers. The measurements were taken from the right side of the body at the biceps, triceps, suprailiac and sub-scapular levels. Measurements of body circumference were taken to the nearest 0.1 inch at waist and hips using a non-stretchable measuring tape. The anatomical sites for the waist and hip circumference measurements were taken at the level of the smallest girth above the umbilicus and at the widest part of the hip region, while the subject was relaxed, in the standing position.
Dietary habits and food frequency of family diet was recorded with the help of a questionnaire. Subjects were asked to recall foods consumed on the previous day, for two days, retrospective dietary intake data was also elicited to obtain information on the actual dietary habits of the subjects. The study was approved by the respective hospital authorities.
Results
Disease History and Personal Data of the Subjects
The study was conducted at 3 hospitals viz, JSS Hospital, Mission Hospital and Kamakshi Hospital in Mysore city. A total of 130 patients afflicted with urolithiasis were interviewed during the study period of six months. All the subjects were found to be men in this study.
For majority of patients the onset of disease was after 21 yrs, the percentage of men being affected was greater in the age group of 21-30 yrs and 31-40 yrs (35% and 26% respectively). In other age group like 41-50, 51-60 and above 60 (15%, 14% and 10% respectively) less percentage compared to 21-30 year age group.
Table 1: Age-Wise Distribution of Subjects and Disease Symptoms
| Symptoms |
Age group |
||||
|
21-30 n = 45 |
31-40 n = 34 |
41-50 n = 19 |
51-60 n = 18 |
>60 n = 14 |
|
| Difficult urination |
3 |
6 |
7 |
11 |
19 |
| Nausea + pain |
5 |
6 |
7 |
8 |
3 |
| Vomiting + difficult urination |
3 |
7 |
7 |
12 |
13 |
| Pain + nausea + difficult urination |
– |
4 |
2 |
2 |
5 |
|
Total |
11 |
23 |
22 |
33 |
40 |
Disease history of subjects revealed that 42% of the subjects did not suffer from any other associated health problems before the onset of urolithiasis. The rest of the subjects were found to be having diabetes (4%), hypertension (19%), urinary tract infection (15%) and heart burn (15%).
Disease symptoms varied from nausea, difficult urination and pain, the severity of symptoms were found to be higher in older patients > 40 years (Table 1). The prevalence of different types of calculi is shown in Fig 1. The incidence of ureteric stones was seen in all age groups, however the occurrence was more in the older age group.
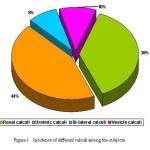 |
Figure 1: Incidence of Different Calculi Among Subjects |
Occurrence of stones in the kidney was also found in all age groups, although the number was more in > 50 years. The overall incidence of different types of calculi was in the following order; ureteric > kidney> vesicle> bilateral.
Although it was not an epidemiological study the occurrence of kidney and ureter calculi was higher in 41-50 years while, 21-30 years was less. Majority of the patients (44%) were offered flush therapy while the rest were treated surgery (28%) and extra corporeal shock wave lithotripsy (ESWL). Flush therapy was the common mode of treatment in the younger age group (21-30 years)
Health Habits of the Subjects
Many subjects were in the habit of chewing and smoking was also a common habit. 52% of them were in the habit of smoking, while 33% of the subjects were also consuming alcoholic drinks with whisky and toddy being the drinks of choice. Majority of them (75%) expressed to have good sleep while the others opined moderate sleep.
Somatic Status of the Subjects
Mean anthropometric measurements of the subjects are presented in Table-2. BMI-Indicates energy status of the individual MUAC and MUAMC indicates the protein status of individual and TSF thickness and WHR indicates body fat status of the individual. Majority of the subjects (69%) had BMI within the normal range. Comparisons of MUAC, MUAMC and TSF thickness with standards showed more number of subjects to be malnourished, indicating utilization of energy from body protein, because of low energy intake, compared to their energy expenditure.
Table 2: Somatic Status of the Subjects
|
Parameter |
Age Group |
|||||||||
|
21-30 |
31-40 |
41-50 |
51-60 |
>60 |
||||||
|
Mean |
SD |
Mean |
SD |
Mean |
SD |
Mean |
SD |
Mean |
SD |
|
| Weight (kg) |
58 |
+6.1 |
59 |
+5.2 |
58 |
+4.2 |
55 |
+3.3 |
45 |
+2.8 |
| Height (cm) |
166 |
+3.1 |
165 |
+2.6 |
166 |
+2.4 |
157 |
+3.2 |
168 |
+2.0 |
| BMI |
19 |
+2.6 |
21 |
+4.2 |
21 |
+3.1 |
21 |
+1.9 |
20 |
+3.1 |
| Waist (cm) |
70 |
+0.3 |
76 |
+0.8 |
77 |
+0.2 |
72 |
+0.8 |
71 |
+0.2 |
| Hip (cm) |
76 |
+0.6 |
84 |
+0.4 |
86 |
+0.01 |
85 |
+0.7 |
84 |
+0.06 |
| WHR |
0.8 |
+0.18 |
0.8 |
+0.05 |
0.9 |
+0.03 |
0.8 |
+0.12 |
0.8 |
+0.17 |
| MUAC (mm) |
84 |
+3.1 |
85+ |
+3.6 |
84 |
+2.3 |
78 |
+3.2 |
75 |
+2.8 |
| TSF (mm) |
71 |
+6.6 |
82 |
+7.7 |
82 |
+6.1 |
75 |
+8.0 |
71 |
+6.5 |
| MUAMC (mm) |
88 |
+5.2 |
87 |
+2.7 |
82 |
+4.3 |
86 |
+4.6 |
83 |
+4.12 |
| Body fat (%) |
9 |
+4.3 |
8 |
+4.1 |
8 |
+3.7 |
8 |
+2.1 |
7 |
+3.75 |
Clinical Data of the Subject
Mean hemoglobin, creatinine, urea and blood glucose are given in table-3. All the four parameters found to be within the normal range. The urinary glucose and albumin was also recorded.
Table 3: Bio- Chemical Profile of the Subjects
|
|
Parameter |
Subjects |
Normal values |
| 1 | Haemoglobin (g%)<910-12>12-14 |
2 26 102 |
12-14% |
| 2 | Creatinine (mg%)0.7-0.91.0-1.4>1.4 |
28 87 15 |
1.0-1.4 mg/dl |
| 3 | Urea (mg%)<2526-40>40 |
20 100 10 |
Upto 40 mg/dl |
Majority of the subjects (79%) had hemoglobin within the normal range of 12-14%, only 21% were found to have below normal value. Creatinine and urea levels were within the normal range for majority of the subjects.
Dietary Pattern and Intake Data
The meal pattern at home consisted of Ragi (foxtail millet) dumplings, Rice, Chapathi etc. During the hospital stay the subjects were consuming soft and liquid diet. Cereals were predominant items of the daily menu. The cereal commonly used was Ragi, Rice, Wheat and Jowar (sorghum) in the descending order. Among pulses, split pulses were used less frequently (58%), while a variety of whole grams like Horse gram, Red gram, Field bean, Green gram etc were used daily (78%). Milk was being used daily by all the patients in the form of Coffee/ Tea, Curds/Butter milk. 72% of the subjects family were using Buffalo milk, while 28% used cow’s milk. 52% of the families were buying less than half liter, while rest were found to use ½ – 1 liter/day. The majority of families (48%) used ground nut oil, while 38%, used both palm oil and refined sunflower oil, while the rest used hydrogenated fat and gingelly oil also. Fruit consumption was very low (15%). The diets were predominantly of cereals-type and low in protective foods like vegetables specially green leafy vegetables which are rich in anti-oxidants. The frequency of use of foods rich in calcium and oxalates by the subjects, it was found to vary widely, ranging from daily for Ragi (95%) and horse gram (45%) to weekly once or twice for green leafy vegetables and other pulses like Black gram and Green gram. Among these foods, horse gram and ragi are also rich in phytates and oxalates.18 The mean food intake of the subjects is given in Table-4. Cereals were the major items of food consumed, followed by pulses and other vegetables. The mean of all food items except cereals pulses and roots and tubers were satisfactory, when compared to the desirable dietary pattern (DDP), very poor intake of green leafy vegetables and fruits.
Table 4: Mean Food Intake Data of the Subjects
|
Parameter |
Age Group |
|
||||||||||
| 21-30 |
31-40 |
41-50 |
51-60 |
>60 |
||||||||
|
Mean |
SD |
Mean |
SD |
Mean |
SD |
Mean |
SD |
Mean |
SD |
Total |
DDP* |
|
| Cereals (g) |
425 |
56 |
430 |
51 |
410 |
49 |
415 |
47 |
420 |
49 |
415 |
600 |
| Pulses (g) |
58 |
8 |
60 |
9 |
61 |
7.6 |
60 |
806 |
62 |
9 |
60 |
60 |
| Green leafy vegetables (g) |
13 |
4 |
15 |
7.8 |
20 |
14 |
20 |
16 |
10 |
3.2 |
60 |
100 |
| Other vegetables (g) |
65 |
9 |
70 |
8.1 |
85 |
13 |
65 |
8.7 |
17 |
9.7 |
70 |
100 |
| Roots & tubers (g) |
76 |
9.6 |
65 |
9.7 |
90 |
12.6 |
60 |
8.5 |
55 |
9.2 |
65 |
80 |
| Milk & milk products (ml) |
95 |
14 |
85 |
13 |
85 |
9.3 |
95 |
14.8 |
65 |
11.4 |
85 |
200 |
| Sugar/jaggery (g) |
14 |
5 |
12 |
6.1 |
20 |
12.1 |
15 |
5.5 |
15 |
6.7 |
15 |
30 |
| Fats & oils (g) |
12 |
3 |
12 |
3.01 |
15 |
6.4 |
15 |
7.2 |
20 |
6.2 |
13 |
40 |
| Fruits (g) |
10 |
2.8 |
10 |
5 |
10 |
3.9 |
30 |
15 |
15 |
4 |
15 |
100 |
* – For manual agricultural laborers (Total – 3790 kcal ) – recommended by ICMR
Mean energy intake ranged between 2584-2700 Kcal (table 5). It was found that mean energy intake was higher in 21-30 and 31-40 years when compared to other age group of the subjects. The energy intake was found to be lesser when compared to DDP. The mean protein intake was found to be adequate ranging from 60-63 g. Nutrition quality of the diets consumed by these patients is represented in fig-2. Nutrients as proportions of energy were adequate with regard to the protein, thiamine, calcium, retinol and vitamin C, but fell short of iron and two of the B-complex vitamins, riboflavin and niacin.
Table 5: Daily Intake of Major Nutrients Among Subjects
|
Nutrients |
Age Groups |
DDP * |
|||
|
21-30 Yrs
|
31-40 Yrs
|
41-50 Yrs
|
51-60 Yrs
|
||
| Energy(K cals) |
1290 ± 40 |
1240 ± 31.01 |
1250 ± 25 |
1390 ± 19.1 |
3788 |
| Protein (g) |
30 ± 3.8 |
25 ± 2.17 |
25 ± 1.18 |
30 ± 3.6 |
60 |
| Carbohydrate (g) |
225 ± 13.1 |
210 ± 11.1 |
215 ± 10.1 |
220 ± 9.13 |
600 |
| Fat (g) |
30 ± 3.17 |
25 ± 2.8 |
35 ± 2.18 |
30 ± 2.18 |
45 |
| Dietary Fibre (g) |
30 ± 3.60 |
35 ± 2.71 |
40 ± 2.71 |
33 ± 3.4 |
– |
* DDP- desirable dietary pattern, Values are mean of RDA computed according to occupation (for heavy physical activity) using ICMR data (20)
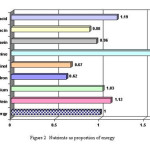 |
Figure 2: Nutrients as proportion of energy |
The intake of iron and thiamine was found to be unsatisfactory, however the bio availability may be expected to be low. Most of the calcium appears to be contributed from the daily consumption of ragi. The daily diet, met RDI with respect to protein, calcium, retinol and vitamin C but was inadequate in calories, B-complex vitamins and Iron. Recommended energy allowance for adult men involved in heavy physical activity is 60 kcal per kg. In this study population, actual intake was lower compared to recommended energy. The estimated mean energy expenditure of the subjects, particularly those engaged in heavy activities such as farmers, Coolies, Workshop men was 3717 kcal which was higher than the mean energy intake of 2638 kcal . It is evident that energy expenditure exceeds the actual energy intake by nearly 1000 Kcal. It clearly indicates that the energy expended by these subjects was more in case of farmers (85%) than in others.
Discussion
The study brings out several interesting factors, Urolithiasis, was more prevalent in men belonging to lower socio-economic status. Among the subjects high percentage of them were engaged in heavy activity like farming and daily laborers and workshop. Urolithiasis is multifactorial diseases caused by several intrinsic and extrinsic factors. Among the intrinsic factors, age and gender are reported to be important factors.1 The peak age of occurrence of disease, in the present study, was found to be between 20-40 years which is similar to reported age of occurrence in various parts of India.18,19
Altered mineral metabolism accounts as greater risk factor. However, these parameters could not be studied, hence no conclusion can be drawn on these aspects. Among the extrinsic factors, climate, fluid intake and occupation appeared to play a role in the formation of stone. Occupation can also have an impact on the incidence of urinary stone.1,4 Individuals working in the field are exposed to hot climate, are prone to dehydration. Heat may cause higher fluid intake but increased perspiration results in low/concentrated urine. This factor may precipitate crystal formation. Geographical variation and socio economic status impact on the dietary habits has been reported by other researchers among subjects from Jaipur, Rajasthan where environment and climatic situation favours fluid loss and dietary habits which play a major role in the formation of calculus.19 Consumption of hard water, foods rich in minerals as Bajara (Pearl Millet), dairy products and dry hot climate our excessive loss of water are the factors associated with the higher incidence.
Increased exposure to sunlight increases vitamin D3 production, which increases intestinal calcium absorption and hence calcium excretion.1,4 It was observed that the intake of fluid including water, by the subjects was in the normal range (6-8 glass per day). Individuals engaged in occupation such as farming, are encouraged to increase fluid intake. In addition water hardness might also contribute, to greater incidence of stone disease. In this population, it was found that bore well water was the major source in these areas. Dietary composition data provides a base line of stone incidence within community, thus influencing risk factors towards over saturation with the salt like calcium oxalate and phosphates.1,3,4
Several dietary factors have been implicated in the occurrence of disease (2-4 ) most important being high protein, calcium, sugar, dietary fiber and oxalate intake. The mean protein intake of the subjects was found to be adequate, calcium intake was higher while the energy was low. Body size measurements indicate a very low energy protein status, despite adequate protein intake. Energy balance is one of the factors which determines the risk of protein deficiency, which is attributed to increased energy requirement.20 It was observed that the energy expended by the subjects was more in case of farmers. Their energy intake was lower compared to the ICMR recommendation.20 It may be stated that low protein status, could be due to utilization of protein as energy intake in the absence of adequate energy intake. The intake of ragi, a cereal rich in calcium, fiber and oxalate was found to be very high among the subjects.
Although calcium intake was more (800 mg) the mineral absorption may be inhibited by the simultaneous presence of high fiber in ragi. The studies in North India have shown a relationship between the incidence of Urolithiasis and wheat consumption..2 Wheat flour and bran have been shown to possess calculogenic property in animals.2 The consumption of horse gram rich in oxalate was also common among the subjects (55%). Mineral absorption is reported to be depressed significantly in the presence of both oxalate and fiber.21 Thus, it appears that the dietary calculogenic effects may be due to the co-ingestion of a mixture of fiber from various sources such as ragi and whole grams (Horse gram). The implications of these observations is that Urolithiasis, which may be due to metabolic abnormalities can be prevented by appropriate change of diet.
Diet counseling is integral part of therapy offered to urinary stone patients. It should aim to reduce the concentration or excretion of stone components (oxalates and calcium) by reducing consumption of specific high-risk foods. The diet therapy should also correct inherent imbalances. Detailed epidemiologic and experimental studies are needed to establish the role of specific risk factors and also to identify causative factors specific to different regions. The results of the study are useful in observing dietary habits, somatic status and health of the population sample. Since, the disease is a common syndrome which recurs, and is complicated by infection and obstruction. It is suggested that systematic diagnostic evaluation, should be conducted, while the patients follow, their usual diet.
References
- Campbell’s Urology; (Ed.), Wash, Retik, Vaughon, Wein W.B, Saunders Company, Vol.3, 2661 (1996).
- Mahtab S. Bamji, Pralhad Rao.N, Vinodini Reddy, Text book of Human Nutrition, Oxford and IBH. Co. Pvt. Ltd., 385 (1996).
- Norman Black lock Renal stone; In Dietary fibre, Fibre- depleted foods and diseases, (Ed.) Hugh Trowell, Denis Burkitt Kenneth Heaton, Academic press, Inc., London, 77 (1985).
- Vijaya T, Sathish Kumar M, Ramarao N.V, Narendra Babu A, Ramarao N. Urolithiasis and Its Causes- Short Review. J of Phytopharmacology 2(3): 1-6 (2013)
- Massary and Glassock’s; Text book of Nephrology, (Ed.), Shal.G, Richard.J. 3rd ed., Vol.2, 1054 (1992).
- Anderson.D.A; Environmental factors in the aetiology of urolithiasis (Ed.), Rapado L.D, Madrid.A, New York, London, Sydney, 130 (1973).
- Anasuya.A; Urinary calculous diseases, Role of nutrition- A review. Nutr.Rep. International, 1095-1100 (1983).
- Parikh H.S and Shah.R.C; Chemical composition of calculi, Indian Journal of Medical Science, 14 (5): 401-405 (1960).
- Raju.R.V.S., Rao C.N. and Satyanarayana.U; Chemical analysis of Urinary Calculi in coastal Andra Pradesh, Indian J.Med.Res, 8: 565-571 (1987)
- Pundir.C.S., Goyal.L., Thakur M., Kuchhal N.K., Bhargava A.K., Yadav S.P.; Chemical analysis of Urinary Calculi in Harayana, Indian J.Med.Res, 62: 17-21 (1973).
- Sarinder Man Singh, Rao.D.V.N and Bapna B.C; Recurrent renal calculi A- study of incidence by follow-up examination, Indian .J.Med. Science, 59: 1077-1082 (1971).
- Singh RG, Behura SK, Kumar R. Litholytic property of kulattha vs. Potassium citrate in renal calculus diseases: a comparative study. JAPI, 58 : 286- 289 (2010).
- Doumas B.T; Clinical Biochemistry Vol.8, Acta press Inc., New York, 87 (1983).
- Tinder P, Determination of blood glucose by enzymatic method. Ann Clinical Biochemistry, 6 : 24 – 29 (1964).
- Chaney A.L and Marbach. Clinical chemistry, 8: 130-132 (1962).
- Kostir J.V and Sonka J. Creatinine estimation in blood serum a new method. Biochimica et Biophysica Acta. 8: 86-89 (1952).
CrossRef - Drupt F. Colorimetric method for determination of albumin. Pharm Bio. 9:777-779(1974)
- Pendse A.K and Singh P.P . The etiology of Urolithiasis in Udaipur (Western part of India) Urol Res 14: 59-62 (1986)
CrossRef - Siddiqui V.A, Singh H, Gupta J, Naya C, Singh. V, Sinha M.N, Gupta A.K, Sumithran P, Rai Y , Rajakumar, Rupali Dixit R, Dewan D. A multicentre observational study to ascertain the role of homoeopathic therapy in Urolithiasis Ind J of Research in Homoeopathy 5: ( 2) 30-39 ( 2011).
- Dietary guidelines for Indians- A manual., National Institute of Nutrition, India 2nd edition (2010)
- Ruth Schwartz, Jean Apgar. B and Wein E.M. Apparent absorption and retention of Ca, Cu, Mg, Mn and Zn from a diet containing Iron, Am. J .Clin. Nutr 43 : 444-455 (1986).





Web of Science Coverage
Emerging Sources Citation Index (ESCI)
2024 Journal Impact Factor: 1.1
Scopus Journal Metrics
CiteScore 2025: 2.6
CiteScore Details
Sustainable Nutrition: Food Systems, Nutrient Retention, and Public Health Impact
![]()
This journal is a member of, and subscribes to the principles of, the Committee on Publication Ethics (COPE)








