Effectiveness of training among food handlers: A review on the Mauritian Framework
1Ministry of Health and Quality of Life, Mauritius.
2Department of Health Sciences, Faculty of Science, University of Mauritius, Réduit, Mauritius.
DOI : http://dx.doi.org/10.12944/CRNFSJ.1.1.01
Download this article as:
![]()
Food handlers are crucial links in the food chain from farm to fork. The safety of our food depends largely on them. However malpractices have been reported on numerous occasions resulting in food poisoning outbreaks. Therefore it is essential that food handlers are properly trained so that they take the necessary precautions to avoid such accidents. The current review analyses the Mauritian model of food handlers training which is mandatory according to the Food Regulations (1999). Although the present model is accessible to the general public as it regionalised and free of charge, there are several weaknesses such as absence of continuous education, no targeted modules and assessment. It is important that these issues be addressed in order to improve the effectiveness of this model. This review also addresses the importance of the food handlers training, conflicting views about the efficiency of training staff to improve food safety practices and provides a critical appraisal of its importance.
KEYWORDS:Training, Food handlers,Food safety,Foodborne diseases
Introduction
A study on food poisoning cases reported that food handlers are responsible for foodborne disease outbreaks for the past years and there is no indication that this is diminishing (Greig et al., 2007). Unsafe food has been a human health problem since history was first recorded, and many food safety problems encountered are not new. Although governments all over the world are doing their best to improve the safety of the food supply, the occurrence of foodborne disease remains a significant health issue in both developed and developing countries (WHO,2006). According to the World Health Organisation (WHO), in 2005 alone, 1.8 million people died from diarrhoeal diseases and most of these cases can be attributed to contaminated food or water. In 2009, 27,037 notifications of 9 diseases or conditions that are commonly transmitted by food have been reported in Australia (The OzFoodNet Working Group. 2009). In Europe, there has also been a marked increase in reported food poisoning cases. In 2009 there were 212,064 human cases of campylobacteriosis as compared to 99,020 cases of salmonellosis (Eurosurveillance editorial team, 2010). Proper food preparation can prevent most foodborne diseases. The WHO has long been aware of the need to train food handlers about their responsibilities for food safety. In the early 1990s, WHO developed the Ten Golden Rules for Safer Food Preparation which was replaced in 2001 by the Five Keys to Safer Food, a global health message which explains the basic principles that each individual should know all over the world to ensure safe food handling practices and prevent foodborne diseases. The Five Keys to Safer Food, and associated training materials, were developed to provide countries with materials that are easy to use, reproduce and adapt to different target audiences (WHO, 2006).
A survey among food handlers in Bangkok concluded that food handlers should attend proper training in the basic principle of food safety and rules of personal hygiene in order to improve their practices in food handling (Cuprasitrut et al., 2011). However, on the other hand studies have highlighted that food safety training alone was not sufficient to improve hygiene attitude and practices of food handlers (Chang et al., 2003; Walker et al., 2003).
Training of managers, supervisors and all people who can influence the safety of food is essential to reduce the unacceptable high levels of food poisoning. According to Sprenger (2009), training is intended to modify or develop knowledge, skills and attitude through learning experience and to achieve effective performance in an activity or range of activities. However, the emphasis on classroom-based, foundation courses and certification in isolation has not been particularly successful in reducing levels of food poisoning. The main reason for this is the belief that ignorance is the main reason for food poisoning (Sprenger, 2009). This observation is supported by a study carried out in Iran, where it was found that half of the food handlers interviewed were not aware that Salmonella, Staphylococcus and Hepatitis A &B viruses and are major causal agents of food-borne diseases (Ansari-lari et al., 2010). It is important for food safety training course to include both theory and practical (Rennie, 1994; Taylor, 1996). The theory part usually englobes core messages such as cleaning, cross-contamination, adequate cooking, temperature control and use of safe water and raw materials (WHO, 2006), whereas the practical part should include aspects such as hand washing which has been demonstrated to reduce the risk of diarrhoea diseases (Xavier et al., 2007).
Furthermore, it is assumed that if food handlers are aware of their legal obligations and they are provided with the knowledge and understanding on the prevention of food poisoning, this will automatically result in the implementation of good hygiene practices (Sprenger, 2009). In fact there is limited evidence that food handlers training, whether mandatory or not, improves food safety practices of food handlers working in food premises, and limited evidence that it enhances knowledge or behaviour ( Pajot and Aubin, 2011)
The objectives of this review are to:
1) provide an overview of the food handler’s training programme in Mauritius;
2) critically analyse the effectiveness of the actual food handler’s training; and
3) recommend correctives measures to improve the present model.
Current Prevalence of Foodborne Diseases in Mauritius
Foodborne diseases have been increasing in recent years, with a greater impact on the health and economy of developing countries (WHO, 2002). Mauritius is not spared from such threats. This is confirmed by the general ascending trend in the number of domestic and commercial reported food poisoning cases for the past twenty years (Health statistics report, 2011) as shown in Table 1 and Figure 1, with sporadic peaks which are more frequent in the last few years, putting our health services under pressure.
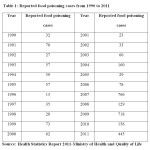 |
Table 1: Reported food poisoning cases from 1990 to 2011 Click here to View table |
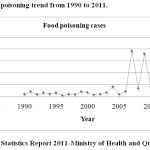 |
Figure 1: Food poisoning trend from 1990 to 2011 Click here to View figure |
In fact, the peaks were due to episodes of mass food poisoning caused mostly by the consumption of contaminated chicken ‘kebab’ containing mayonnaise and cream filled pastries. This increase may be partly attributed to improved surveillance (Griffith et al., 1995; Kaferstein and Abdussalam, 1999) but may equally reflect increased global trade and travel, changes in modern food production, the impact of modern life styles, changes in food consumption and the emergence of new pathogens (Collins, 1997; Tauxe, 1997). In addition, food poisoning cases are mostly caused by human handling errors (Ehiri & Morris, 1996; Greig et al., 2007; Howes et al., 1996) or poor handling practices (Djuretic et al., 1996; Evans et al., 1998). In fact, the inappropriate handling of foods by the food service industry has been implicated in 97% of food poisoning cases (Greig et al., 2007; Howes et al., 1996). Foodborne illnesses typically involve cross-contamination of raw and cooked foodstuff, inadequate cooking, and storage at inappropriate temperatures as well as asymptomatic carriers of food poisoning organisms (Cruickshank, 1990). Consequently, food becomes contaminated, pathogenic bacteria are provided with the opportunity to multiply or they survive inadequate cooking or processing (Sprenger, 2009).
The current scenario of the food producing sector in Mauritius relies heavily on a multiplicity of independently managed operations namely growing, breeding, transport by air or sea, transhipment, land transport, storage, processing, repackaging, distribution, sale at wholesale and retail levels and cooking for sale. Each of these operations is developing into areas of business activity, embracing an ever-increasing number of operators. Aided by the present policy of promoting self-employment, Mauritian Government has encouraged the establishment and expansion of family-run businesses in each of these areas of activity. Competition to maximise revenue and reduce costs have driven operators to continually explore means to avoiding control and supervision. This coincides with the lack of resources and manpower available to agencies responsible for the function of inspecting and analysing food items on sale to the public (NESC, 2010).
Overview of the Mauritian Framework of Food Handlers Training
Prior to 1998, all persons engaged in the handling of food were required under the “Tuberculosis Regulations 1926” to be in possession of a medical certificate delivered by a Government Medical Officer appointed by the Permanent Secretary of the Ministry of Health stating that he is free from Tuberculosis (Section 4). However, with the advent of the Food Act (1998), food handlers are now required, in addition to medical examination, to follow a food hygiene training course approved by the Permanent Secretary of the Ministry of Health and Quality of Life to obtain a Food Handler’s Certificate issued by a Government Medical Officer ( Section 47 of the Food Regulations (1999). The motivations for the change in policy were to modernise and consolidate the law related to the quality of food (Food Act, 1998). The certificate is valid for one year and shall be renewed for two additional years after which the food handler need to apply for a new one without having to undergo the training course again but medical examination only.
To obtain a Food Handler’s Certificate for the first time, a person needs to apply to the nearest Regional Health Office by submitting his/her particulars together with two passport size photographs. An appointment is given to him/her for the training course and medical examination. Usually the applicants have to attend to lectures delivered in a venue of the office. However, for large organisations such as hotels, supermarkets, hypermarkets or food processing plants where the populations of food handlers are important, training courses are delivered on site in order not to disrupt the activities of the operators. Specific tasks undertaken and knowledge in food hygiene is the same for all categories of food handlers irrespective whether they deal with raw, ready to eat, high risk or low risk food. All the services related to the Food Handler’s Certificate are offered free of charge by the Ministry of Health and Quality of Life.
Training course approved by the Permanent Secretary of the Ministry of Health and Quality of Life is also run by private individuals and organisations, but against payment. However, issue of the Food Handler’s Certificate is only done by Government Medical Officers of the Ministry of Health and Quality of Life. According to records available at the Ministry of Health and Quality of Life, 21,344 Food Handler’s Certificates have been issued in 2012.
Importance, Benefit and Effectiveness of Training in Food Safety and Hygiene.
Having recognized that the objective of food safety training is to provide competent food handlers who continuously produce safe food, management must be convinced of the importance and benefit of training to provide the necessary resources. Training should be considered as an investment in the future and evidence is available to show that companies providing high levels of training usually have better growth and profits. Food safety remains a critical issue with outbreaks of foodborne illness resulting in substantial costs to individuals, the food industry and the economy (Kaferstein et al., 1997). Such training should contribute significantly to the profitability of a food business by assisting in the production of safe food, safeguarding the quality of the product and reducing food wastage Training is necessary to enable staff to fulfil their potential by understanding their responsibilities and improving their skills.
Hygiene training of staff should stress the importance of hygiene to the commercial viability of the organisation and how a food poisoning incident or serious food complaint is likely to affect them. Training also helps to promote confidence, increase job satisfaction, improve performance/morale and supervisory skills of managers, generate pride in appearance and practices, develop team spirit, and reduce the amount of supervision required; reducing complaint, increasing job satisfaction and probably reducing staff turnover are equally essential. Moreover, training contributes to increase productivity, promotes a good company image as well as ensures that all the correct procedures, including cleaning, are followed so as to comply with any legal provisions or the requirements of industry guides or codes of practice. Through training the food industry will benefit by having available a pool of trained food handlers. It has been reported that when selecting restaurants, customers increasingly perceived hygiene as a critical determinant ( Park et al., 2010) and owners of restaurants highlighted that food quality and hygiene are considered as key factors in the profitability of the food business ( Yoon and Moon, 2003). On the other hand the Food Standards Agency (FSA) and Health Protection Agency (HPA) estimated that in England and Wales economic loss due to food- borne diseases amounted to approximately £1.4 billion, with 765,000 cases recorded (FSA, 2006).
Food handler training is seen as one strategy whereby food safety can be increased, offering long-term benefits to the food industry (Smith, 1994). A study to evaluate knowledge, attitudes, and behavior concerning foodborne diseases and food safety issues among food handlers in Italy demonstrated that the level of knowledge was higher among those who attended training courses in food safety (Angelillo, 2000) .Effective food safety training involve two stages. Firstly the provision of knowledge in a way that develops understanding and a positive attitude, for example, the importance of hand washing and the knowledge when to wash the hands. In fact, hand washing has proved to reduce contamination significantly ( Bidawid et al., 2000) compared to glove wearing where a study has reported that such practice failed to reduce bacterial contamination due to protracted period and complacency (Lynch et al., 2005). However, combining the use of gloves with proper hand washing can reduce the risk of cross contamination (Montville et al., 2001).The second stage involves the implementation of the knowledge by washing the hands properly when required. Practice, motivation and effective supervision, especially coaching, should result in the objective being achieved, i.e. the competency of the food handler and implementation of good practice at all times (Sprenger, 2009).
Critical Appraisal of the Effectiveness of the Mauritian Food Handler’s Training Framework.
In Mauritius, it is mandatory for food handlers to follow a food hygiene training course. Several studies have attempted to evaluate the effectiveness of food safety training on practices in foodservice establishments and resulted in divergent arguments. A study on the effectiveness of an in-house food safety programme among mid-level managers and food handlers in large catering establishment showed that food safety training improved microbiological quality of food (Cohen et al., 2001). Other studies established that inspection score improved after staff were trained in food safety (Cotterchio et al., 1998; Kneller & Bierma, 1990; Mathias et al., 1995). Cotterchio et al. (1998) demonstrated that a year after the training, the mean inspection score increased by 14.7 points among 23 restaurants in Boston. On the other hand studies found that there was no or insignificant change in inspection score after food handlers were trained (Cassey & Cook, 1979; Mathias et al., 1994 and Wright & Feun, 1986). Although there is evidence that food safety training is effective at enhancing knowledge (Park et al., 2010), the latter does not always improve practices (Howes et al., 1996). Therefore the legal obligation for food handlers to be trained in food safety is not a guarantee that they are going deliver safe food to the public.
A study among restaurant staff in Korea demonstrated that food hygiene training significantly improved knowledge and so practicing continual and repetitive food hygiene training could be effective in improving knowledge further and even practices (Park et al., 2010). However this observation contrasts sharply with the Mauritian framework where food handlers are required to undergo food hygiene training course only once in their career, that is when they start to work in the food sector. Such a procedure defeats the purpose of ensuring safe food to the population as education must be continuous in order to be successful (Hinkin, 2000).
In the Mauritian model of food safety training course, the content of the modules is the same for all categories of food handlers irrespective whether they deal with raw, ready to eat, high risk or low risk food. According to the World Health Organisation – Europe (Fact sheet Copenhagen and Parma, 2010), infections with Salmonella spp. rise by 5-10% for each one-degree increase in weekly temperature, at ambient temperature above 5oC due to climate change. Actually food poisoning outbreaks involving Salmonella seem to be on the rise in recent decades (Greig et al., 2007). It is estimated that 93.8 million cases of gastroenteritis due to Salmonella species occur globally each year, among which approximately 80.3 million is of foodborne origin and resulting in 155,000 deaths (Majowicz et al., 2010). It is reported that raw poultry and eggs, whether on the shell or internally, can be contaminated with Salmonella and this represents potential cause of foodborne outbreaks (Gómez-Aldapa et al., 2012). In 2012, Mauritius had a population around 1.3 million and the consumption of eggs and chicken per inhabitant was estimated at 6.86 kg/year and 35.7 kg/year respectively. The average monthly household disposable income increased by 53.9% from USD 615 (Rs 19,080) in 2006/07 to USD 947 (Rs 29,360) in 2012 where the largest broad category of household expenditure remained ‘Food and non-alcoholic beverages’ accounting for 27.3% of total household consumption expenditure in 2012 (USD 211 (Rs 6,540) per month) compared to 28.5% in 2006/07 (USD 145 (Rs 4,500) per month) (Statistics Mauritius, 2012). In Mauritius food poisoning cases increased drastically over the past ten years (Table 1 and Figure 1). In 2008, 53 cases of Salmonella were reported in one episode of food poisoning after ingestion of contaminated egg- containing food namely “Marlin mousse” (Issack et al., 2009). However, much of the risk posed by Salmonella can be mitigated through proper handling and correct food safety practices (Gómez-Aldapa et al., 2012) and so it is important that food safety training courses be tailor-made to target specific audience which are more liable to cause Salmonella food poisoning.
In the Mauritian model, no provision has been made for assessment of the food handlers after the training course. Certification is based according to the attendance of the participants. However, evaluation is integral to the cycle of training, providing feedback on the effectiveness of the method used, checking the achievement of the objectives set by both the trainer and trainee and assessing whether the needs originally identified have been met ( Bramley, 1996Aa study among food handlers in Brazil concluded that training course should include an evaluation process to ensure its effectiveness (Soares et al., 2012).
Conclusion and Recommendations
Although there are diverging opinions about the impact of food hygiene training course on practices, there is a consensus that it improves knowledge. The Mauritian model provides the opportunity for everyone involved in food activities to have access freely to such education. However the actual model is incomplete in the sense that some components are missing such as continuous education, assessment and targeted modules, although enforcement plays an important role in compelling food handlers to put into practice what they have learnt.
Therefore in order to improve the efficiency of food handler training model it is recommended to:
- Make it mandatory for food handler to undergo a refresher food safety training course prior to renewal of their Food Handler’s Certificate after its expiry after 3 years.
- Assess the food handlers before issuing the certificate in order to evaluate the knowledge retained after the training course.
- Train food handlers according to their need and risk which the food may represent to consumers in terms of food poisoning.
References
- Greig J.D., Todd E.C.D., Bartleson C.A. and Michaels B.S., “Outbreaks where food workers have been implicated in the spread of foodborne disease. Part1, Description of the problem, methods, and agents involved”, J. of Food Prot. Tech., 70(7), 1752-1761 (2007).
CrossRef - World Health Organisation, “Five keys to safer food manual” 2006, available at: http://www.who.int/foodsafety/publications/consumer/manual_keys.pdf (accessed 24 July 2013).
- The OzFoodNet Working Group, “Monitoring the incidence and causes of diseases potentially transmitted by food in Australia: annual report of the OzFoodNet Network, 2009”, Commun Dis Intell, 34(4), 396-426 (2010).
- Eurosurveillance Editorial Team, “The European Union summary report on trends and sources of zoonoses, zoonotic agents and food-borne outbreaks in 2010”, available at: http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=20113 ( accessed 22 July 2013).
- Cuprasitrut T., Srisorrachatr S. and Malai D., “Food safety knowledge, attitude and practice of food handlers and microbiological and chemical food quality assessment of for making merit for monks in Ratchathewi District”, Asia J. of public health, 2(1), 27-34 (2011).
- Chang H.J., Lee J.S., Kwak T.K., “Effectiveness of HACCP-based training on the food safety knowledge and behaviour of hospital foodservice employees”, Nutritional Sci, 6,118-26 (2003).
- Walker E., Pritchard C. and Forsythe S, “ Food handlers’ hygiene knowledge in small food businesses”, Food Control, 14, 339-43 (2003).
CrossRef - Sprenger R.A., “Hygiene for Management”, Highfield Publications, SouthYorkshire, 15th edition, 150-151 (2009)..
- Ansari-Lari M., Soodbakhsh S. and Lakzadeh L., “Knowledge, attitudes and practices of workers on food hygienic practices in meat processing plants in Fars, Iran”, Food Control, 21, 260-263 (2010).
CrossRef - Rennie, D.M., 1994, “Evaluation of food hygiene education”, British Food J., 96(11), 20-25 (1994).
CrossRef - Taylor, E., “Is food hygiene training really effective?”, Env. Health, 275-276 (1996).
- Xavier C.A.C. , Oporto C.F.O., Silva M.P. , Silveira I. A. and Abrantes M.R., “Prevalence of Staphylococcus aureus in food handlers from grades schools located in Natal city, RN, Brazil”, The Brazilian Magazine of Clinical Analyses, 39(3), 165-168 (2007).
- Pajot M. and Aubin L., “Does food handler training improve food safety? A critical appraisal of the literature” (2011), available at: http://www.peelregion.ca/health/resources/pdf/mandatory-food-handler-training.pdf (access on 25 July 2013).
- World Health Organistion, “ Food safety and foodborne illness” Fact sheet No. 237, (2002), available at: https://apps.who.int/inf-fs/en/fact237.html (access on 28 July 2013).
- Health Statistics Unit, “Health Statistics Report 2011”, Ministry of Health and Quality of Life (2012).
- Griffith C.J., Mullan B. and Price P.E., “Food safety: implications for food medical and behavioural scientist” British Food J., 97(8), 23-28 (1995).
CrossRef - Kaferstein F.K. and Abdussalam M., “Food safety in the 21st century”, Bulletin of the World Health Organisation, 77(4), 347-351(1999).
- Collins J.E., “Impact of changing consumer lifestyle on the emergence of and re-emergence of foodborne pathogens”, Emerg. Infect. Dis., 3(4), 471-479 (1997).
CrossRef - Tauxe R.V., “Emerging foodborne disease, an evolving public health challenge”, Emerg. Infect. Dis., 3(4), 425-434 (1997).
CrossRef - Ehiri J.E. and Morris G.P., “Hygiene training and education of food handlers: does it work?”, Ecology of Food and Nutrition, 35, 243-2511 (1996).
CrossRef - Howes M., McEwen S., Griffiths M. and Harris L., “Food handler certification by home study: measuring changes in knowledge and behaviour”, Dairy Food Env. Sanitation, 16, 737-744 (1996).
- Djuretic T., Ryan M. and Wall P.G., “The cost of inpatient care for acute infectious intestinal diseases in England from 1991 to1994”, CDR Review, 6, R78-R80 (1996).
- Evans H.S., Madden P., Douglas C., Adak G.K., O’Brien S.J., Djuretic, T. et al., “General outbreaks of infectious intestinal diseases in England and Wales: 1995 and 1996”, Communicable Diseases and Public Health, 1(3), 165-171 (1998).
- Cruickshank J.G., “Food handlers and food poisoning: training programmes are best”, British Medical J., 300(6719), 207-208 (1990).
CrossRef - National Economic And Social Council, “An investigation into food safety in Mauritius: recommendations for a policy review”, NESC Report 15 (2010).
- Tuberculosis Regulations 1926, GN 152/1926 (1926).
- Food Regulations, 1999, Government Notice No. 173 of 1999, Government Gazette of Mauritius No. 114 of 8 December 1999 (1999).
- Food Act, 1998, Act No. 1 Government Gazette of Mauritius No. 64 of 13 June 1998.
- Kaferstein F.K., Moterjemi Y. and Bettcher D. W., “Foodborne disease control: a transnational challenge”, Emerg. Infect. Dis., 3(4), 503-510 (1997).
CrossRef - Park S.H., Kwak T.K. and Chang H.J., “Evaluation of the food safety training for food handlers in restaurants operations”, Nutrition Research and Practice, 4(1), 58-68 (2010).
CrossRef - Yoon J.Y. and Moon H.K., “Job satisfaction and business attitude of restaurant owners – focused mainly in the Gyeongnam area”, Korean J. of Community Nutrition;8:610-20 (2003).
- Food Standards Agency Oct 2006, Board Paper, available at : www.food.gov.uk/multimedia/pdfs/pro061001.pdf ( accessed 24 July 2013 )
- Smith R., “Food hygiene training: the chance to create a coherent training policy”, British Food J., 96(7), 41-45(1994).
CrossRef - Angelillo I.F., Viggiani N.M., Rizzo L. and Bianco A., “Food Handlers and Foodborne Diseases: Knowledge, Attitudes, and Reported Behaviour in Italy”, J. of Food Prot.; 63(3). 381-385 (2000).
CrossRef - Bidawid S., Farber J.M., Sattar S.A., “Contamination of foods by food handlers: experiments on hepatitis A virus transfer to food and its interruption”, Appl. Env. Microbiol., 66(7), 2759–63 (2000).
CrossRef - Lynch R.A., Phillips M.L., Elledge B.L., Hanumanthaiah S. and Boatright D.T., “A preliminary evaluation of the effect of glove use by food handlers in fast food restaurants”, J Food Prot.,68(1):187–90 (2005).
CrossRef - Montville R., Chen Y. and Schaffner D., “Gloves barriers to bacterial cross-contamination between hands to food”, Journal of Food Prot., 64, 845e849 (2001).
- Cohen E., Rachel A. and Schwartz Z., “On the efficiency of an in-house food sanitation training program: Statistical measurements and practical conclusions”, J. of Hosp. and Tourism, 25(1), 5-16 (2001).
- Cotterchio M.J., Gunn M.J., Coffill T., Tormey P. and Barry B.A., “ Effect of a manager training program on sanitary conditions in restaurants”, Public Health Report, 113, 353-358 (1998).
- Kneller P. and Bierma T., “Food service certification measuring the effectiveness of a state program”, J. Env. Health, 52(2), 292-294 (1990).
- Mathias R.G., Sizio R., Hazelwood A. and Cocksedge W., “ The effect of inspection frequency and food handler education on restaurant inspection violation”, Can. J. of Public Health, 86(1), 46-50 (1995).
- Cassey, R. and Cook, C., “Assessment of a food service management sanitation course”, J. Env. Health, 41(5), 281-284 (1979).
- Mathias R.G., Riben P.D., Campbell E., Wiens M., Cocksedge W., Hazelwood, B., Kirschne R, B. and Pelton, “The evaluation of the effectiveness of routine restaurant inspections and education of food handlers: restaurant inspection survey” J., Can. J. Public Health, 85(1), S61-669 (1994).
- Wright J. and Feun, L., “Food service manager certification: An evaluation of its impact” J. of Env. Health, 49(1), 12-15 (1986).
- Hinkin J., “Hand decontamination: what interventions improve compliance?”, EDTNA ERCA journal, 28(3), 134-7 (2002).
CrossRef - World Health Organisation, Europe, “The solid facts on climate change and health” , Fact sheet Copenhagen and Parma, 12 March 2010, available at: http://www.euro.who.int/__data/assets/pdf_file/0010/95815/FS_ParmaClosure.pdf (accessed 28 July 2013)
- Majowicz S.E., Musto J., Scallan E., Angulo F.J., Kirk M., O’Brien S.J., Jones T.F., Fazil A., and Hoekstra R.M., “ The global burden of nontyphoidal Salmonella gastroenteritis”, Clin Infect Dis, 50(6):882-889 (2010).
CrossRef - Gómez-Aldapa C.A., Torres-Vitela M.R., Villarruel-López A. and Castro-Rosas J., “The Role of Foods in Salmonella Infections, Salmonella – A Dangerous Foodborne Pathogen”, Dr. Dr. Barakat S M Mahmoud (Ed.), ISBN: 978-953-307-782-6, InTech, availableat:http://cdn.intechopen.com/pdfs/26421/InTechThe_role_of_foods_in_salmonella_infections.pdf ( accessed 24 July 2013).
- Statistics Mauritius, “Household Budget Survey 2012 – Preliminary results & Updated weights for the Consumer Price Index” Statistics Mauritius 2013.
- Issack M.I., Hendriksen R.S., Lun P.L., Lutchun R.K. and Aarestrup F.M., “Salmonella enterica serovar Typhimurium in Mauritius linked to consumption of marlin mousse”, Foodborne Pathogens and Disease, 6(6), 739-741(2009).
CrossRef - Bramley P., “Evaluating training effectiveness: translating theory into practice”, McGraw-Hill1, London, (1996).
- Soares L.S., Almeida R. C.C., Cerqueira E.S., Carvalho J.S. and Nunes I.L., “Knowledge, attitudes and practices in food safety and the presence of coagulase-positive Saphylococci on hands of food handlers in the schools of Camaçari, Brazil”, Food Control, 27, 206-213 (2012).
CrossRef
Accepted on: August 18, 2013





Web of Science Coverage
Emerging Sources Citation Index (ESCI)
2024 Journal Impact Factor: 1.1
Scopus Journal Metrics
CiteScore 2025: 2.6
CiteScore Details
Sustainable Nutrition: Food Systems, Nutrient Retention, and Public Health Impact
![]()
This journal is a member of, and subscribes to the principles of, the Committee on Publication Ethics (COPE)








