
Introduction
Gastric cancer (GC) is one of the most rapidly lethal malignancies. It has been the fifth most frequent type of cancer worldwide and the second-leading cause of cancer-related death, responsible for over 1,089,103 new cases and an estimated 769 000 deaths in 20201. While there has been a decline in gastric cancer incidence in certain regions, it remains a significant clinical challenge due to late detection in the majority of cases, limited predictive capabilities, and few treatment options available.2. The prevalence of gastric cancer in Asian countries and Middle East varies greatly by regions, most prevalent being in Eastern Asia. In Japan, it is projected to be 12 times greater than in India and Iran, and seven times more common than in Iraq3. Gastric cancer develops when malignant cells start to grow out of control in the lining of the stomach4. Many factors may play a role in the development of gastric cancer. Age, gender, blood type, family history and genetic factors may contribute to the development of gastric cancer, but they are neither modifiable nor preventable5. Nutritional factors, body weight, body fat, and behavioral habits like cigarette smoking and alcohol consumption, along with Helicobacter pylori infection, are all recognized contributors to the onset of gastric cancer5 6. However, these factors are largely modifiable and preventable. Moreover, physical activity may play a role in the prevention of gastric cancer.
Diet is an important modifiable risk factor for gastric cancer. Various epidemiological studies observed an association between some nutritional exposures and dietary components with gastric cancer. High intake of processed meat, fat, sugar, salty and fried food and dairy products has been associated with a higher risk of gastric cancer7 8. The consumption of unhealthy processed food and low consumption of fruits and vegetables may increase the risk of development of gastric cancer. Conversely, a diet high in vegetables and fruits and a variety of natural food may have a preventive effect. Therefore, conducting a comprehensive review of studies, including cross-sectional, case-control, and cohort studies, as well as systematic reviews and meta-analyses, on both non-modifiable and modifiable factors in GC is essential for obtaining a thorough understanding of the disease. Such a review encompasses genetic, demographic, lifestyle, and dietary factors, providing valuable insights for healthcare professionals. This comprehensive understanding aids in patient assessment and management by informing healthcare professionals about relevant risk factors. Moreover, it facilitates the development of effective preventive strategies and guides research priorities in the field. Additionally, the findings of this review can play an important role in patient education, empowering individuals to make informed decisions about their health and contributing to improved outcomes in the management of GC.
Methods
A PubMed, ScienceDirect, Google Scholar and Scopus search was performed for publications from February 1998 through April 2022. Our search included modifiable and non-modifiable risk factors that are associated with the risk of GC, of any type (adenocarcinoma, lymphoma, sarcoma, or carcinoid) and location (cardia or non-cardia).
Terms used in the search strategy included the exposures— body weight and body fat, diet, fruits and vegetables, meats and processed meats, fried and fast foods, milk and dairy products, salty foods, food and dietary patterns, fat and sweets intake, alcohol consumption, smoking, physical activity, age, sex, family history, blood type, genetics, medication —and the risk of gastric cancer.
Observational (cohort and case-control) studies, systematic reviews and meta-analysis addressing the association between gastric cancer and any of the above exposures were included.
We restricted our extensive search to studies related to the objective of the review and those published in English and reported on human subjects. All of the authors conducted the literature search independently. Table 1 shows the search strategy summary.
Table 1: Summary of Search Strategy
|
Items |
Specification |
|
Date of Search |
October-December; 2023 |
|
Databases and other sources searched |
Google Scholar; MEDLINE (PubMed); Scopus; and ScienceDirect |
|
Search terms used |
Body weight and body fat; Diet; Fruits and vegetables; Meats and processed meats; Fried and fast foods; Milk and dairy products; Salty foods; Food and dietary patterns; Fat and sweets intake; Alcohol consumption; Smoking; Physical activity; Age; sex; Family history; Blood type; Genetics; Medication —and the risk of gastric cancer. |
|
Duration |
2001 to 2024 |
|
Inclusion Criteria |
– Studies from different designs; from cross-sectional, case-control, and cohort studies; as well as systematic reviews and meta-analysis. – Articles published in English language |
|
Selection process |
Each of the authors independently conducted the literature search. |
Factors associated with gastric cancer
Many factors that may lead or prevent cancer exist. It is divided into modifiable and non-modifiable factors. In this literature review we will shed the light on the most important modifiable and non-modifiable factors that are associated with GC.
Modifiable risk factors associated with gastric cancer
Body weight and body fat
Several studies show that there is an association between excess body weight and cancer prevalence7-9. Obesity has been linked to both cancer incidence and mortality in many epidemiological studies 8. Although some studies have established a link between excess body weight and an increased risk of GC7, existing epidemiologic research on the link between high body weight and the risk of stomach cancer has shown controversial results10. It might be explained by the high levels of estrogen secreted by the adipose tissue. Exposure to estrogenic effects for prolonged periods of time may reduce the incidence of GC. Most studies show that there is an indistinct association between body fat and GC8 9. In fact, high adipocytes in the body and inflammatory cells that secrete adipokines and cytokines may promote tumor development and contribute to the development of GC. Gastroesophageal reflux disease (GERD), a risk factor for esophageal cancer and cardia gastric cancer (GC), may be caused directly by abdominal fat11. Furthermore, fat is metabolically active, producing a variety of metabolic products that circulate throughout the body such as insulin-like growth factor and leptin9. Both metabolites have been linked to cancer, possibly by inducing pro-growth modifications in the cell cycle, reduced cell death, and pro-neoplastic cellular changes. In most investigations, obesity was linked to a higher risk of stomach cancer9, especially in men and non-Asians. Being overweight and obese was linked to a higher risk of gastric cardia cancer (GCC)9. The link between total body fat and stomach cancer may vary between men and women12. For men, there is no sufficient evidence of an association, while in female participants, total body fat mass was associated with a reduced risk of stomach cancer12 (Figure 1).
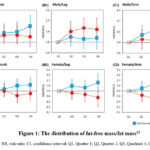 |
Figure 1: The distribution of fat-free mass/fat mass12 |
(Abbreviations: RR, risk ratio; CI, confidence interval; Q1, Quarter 1; Q2, Quarter 2; Q3, Quadrant 3; Q4, Quadrant 4).
A recent study shows an association between lean and fat mass distribution and GC risk12. The analyses were segmented by age (37–49, 50–59, or ≥75 years) and further adjusted for various factors including ethnicity, smoking status, alcohol consumption, polygamy index, physical activity, fruit and vegetable consumption, diabetes, height, NSAID use, and family history of cancer. Additionally, adjustments were made for lean mass and fat mass, with mutual adjustments for each other12. The authors observed that lean body mass, especially located in the arms and torso in women, was associated with an increased risk of GC12. However, total and arm fat mass were associated with a reduced risk of stomach cancer in women12. For both sexes, lean arm mass is probably the best predictor of stomach cancer risk12. These results indicate that lean and fat mass may play different roles in GC development in men and women12.
Diet and GC
Fruits and vegetables and GC
Several studies investigated the association between the consumption of fruits and vegetables and the risk of GC13-18. Schwingshackl et al. (2017) conducted a systematic review and meta-analysis study, and reported that high adherence to the Mediterranean diet has a positive effect on overall cancer risk in primary prevention17. Mediterranean diet mainly consists of high content of fruits, vegetables, and whole grains17. As a result, the phytic acid, resistant starch, and soluble fiber found in the stated food groups are capable of binding and neutralizing potentially carcinogenic compounds in foods which may protect from GC development (RR observational: 0.82, 95% CI 0.75 to 0.88; I2 = 73%, n = 11 studies; RR cohort: 0.86, 95% CI 0.80 to 0.92, I2 = 28%, n = 6 studies; RR case-control: 0.71, 95% CI 0.57 to 0.88, I2 = 88%, n = 5 studies)17. Moreover, Cover et al. (2013) demonstrated that high consumption of fruits and non-starchy vegetables protects against stomach cancer14. In women, flavonoids have been associated with a 20% reduction in the risk of developing GC14. The protective effect of fruits and vegetables against the development of stomach cancer was associated to the high amounts of antioxidants14. Furthermore, Farmanfarma et al. (2020) found that citrus fruits, fresh fruits, and garlic intake were associated with a lower risk of stomach cancer15. Fruits are high in antioxidants, fibers, vitamins, and minerals that can prevent cancer development or progression15. Some vegetables, such as onions, had a little preventive effect against this malignancy when consumed less than twice a week (OR=1.28; 0.73–2.23)15. The reason is unclear; however, it could be from the soil’s contents15. Bae et al. (2016) reported that citrus fruit consumption significantly reduces the risk of stomach cancer, particularly cardiac gastric cancer (CGC) (p-value=0.002)13. Consuming 100 g of citrus fruit per day decreased CGC risk by 40% (RR, 0.603; 95% CI, 0.439 to 0.827)13. Similarly, Wang et al. (2014) showed that fruit intake had a strong protective impact on GC risk, however not for vegetable consumption (fruit: SRR= 0.95, 95% CI: 0.91–0.99; vegetable: SRR = 0.96, 95% CI: 0.91–1.01)18. Nemati et al. (2012) reported that a lack of fresh fruits and vegetables consumption was a risk factor for stomach cancer16. In fact, high consumption of fruits, particularly citrus fruits are associated with a lower risk of stomach cancer due to its antioxidant activity16. This study indicates that citrus fruit reduced the risk of developing GC more than other fruits due to high levels of ascorbic acid and beta-carotene16.
Meats and processed meats and GC
In the meta-analysis study conducted by Kim et al. (2019), a distinct correlation was observed between elevated consumption of red and processed meats and a heightened risk of gastric cancer19. Red and processed meat were linked to a 41% and 51% higher risk of GC, respectively (RR, 1.41; 95% CI, 1.21–1.66; RR, 1.57; 95% CI, 1.37–1.81)19. Also, Tayyem et al. (2023) found that patients who consumed cooked red meat (veal and lamb) were more likely to develop GC20. In addition, Zhao (2017) stated that the dietary guidelines should be updated due to the relationship between red and processed meat consumption and GC risk21. Moreover, a study that was conducted in Iran by Farmanfarma et al. (2020) reported that there is a significant link between processed red meat intake and the risk of developing stomach cancer15. Furthermore, Huang et al. (2021) found that red meat consumption increased the risk of GC by 11%-51%, with every 100 grams/day raising the overall cancer mortality22. Besides, every 50 gram/day increase in processed meat consumption was linked positively to GC by 8%-72%22. These findings might be explained by the high concentrations of nitrite present in processed meat that interact with secondary amines and N-alkylamides to form Carcinogenic N-nitroso compounds (NOCs), which is a mixture of nitrosamines and nitrosamides22. O6-Alkylguanines couple with thymine instead of cytosine, which causes changes in DNA base pairs, forming carcinogens due to the metabolism of nitrosamines22. Likewise, Collatuzzo et al. (2022) indicated a positive correlation between GC and total red meat intake23. This correlation had an HR of GC equal to 1.4123. Overall red meat consumption was associated with an 8% and 9% increase in GC risk23. Similarly, a significant increase was observed with the consumption of red meat and it was reported that red meat and processed meat consumption cause GC24. However, according to Poorolajal et al. (2020), the intake of red meat had no significant impact on stomach cancer (p=0.080), and the overall OR was 1.31 (95% CI, 0.87 to 1.96) when eating red meat ≥4 times/week vs. <4times/week25. In addition, Wilunda et al. (2022) demonstrated that consumption of all meats, red meats, and processed meats was not associated with GC26. In fact, meats heme iron promotes the endogenous formation of (NOCs), which is a risk factor for GC. It affects high levels of nitrogen residues in the gastrointestinal tract, which contributes to the formation of DNA adducts. Another reason is high temperatures used to cook red and processed meats, which creates a significant amount of carcinogens including polycyclic aromatic hydrocarbons, heterocyclic amines, and N-nitroso compounds15 19 21.
 |
Figure 2: The catalytic effect of heme iron on fat peroxidation and N-nitrosation, as well as their inhibition through dietary interventions 27. |
Nitrosation and fat peroxidation are catalyzed by heme iron27. The end products are N-nitroso compounds (NOCs), malondialdehyde (MDA), and 4-hydroxy-nonenal (4-HNE)27. Through these pathways, red and cured meat promotes cancer27. Calcium carbonate or chlorophyll can be used to trap heme iron and inhibit its catalytic activity27. Vitamin C and E inhibit endogenous NOC formation27. Moreover, certain polyphenols may inhibit fat peroxidation and-or nitrosation27.
Fried and fast foods and GC
A study conducted by Guo et al. (2018) in China demonstrated that fried food consumption is linked to stomach cancer and pre-cancerous lesions28. Fried food consumption was found to be a risk factor for GC (OR=1.89, 95% CI: 1.57-2.28; OR=1.91, 95% CI: 1.66-2.20)28. Another study conducted in China found that fast-food patterns have been linked to increase gastric cancer risk29. In addition, Koszucka et al. (2020) demonstrated that acrylamide is a carcinogenic compound that is formed during heat-induced processes, such as frying, and causes mitochondrial dysfunction30. Moreover, Li et al. (2022) showed that GC and pre-cancerous lesions were independently associated with frequent consumption of fried foods31. Furthermore, Duan et al. (2021) reported that there was an independent risk for GC associated with both irregular meals and eating fast food (OR = 1.71, 95% CI: 1.62-1.91 for irregular meals, and OR = 1.83, 95% CI: 1.71-2.01 for fast food)32. Ghaffari et al. (2019) reported that one of the risk factors that leads to GC is consuming fried food33. Additionally, Sun et al. (2019) found that the consumption of fried foods is associated with a significant risk of GC as it lowers the levels of vascular endothelial growth factor (Z=1.740, P=0.006) and increases tumor necrosis factor –α levels (P<0.05)34. The mucous membrane of the upper digestive tract could be damaged by eating fried foods and fast food, which may lead to GC34. On the other side, fat may induce inflammatory events in diabetes by activating the Toll-like receptor 4 (TLR4) pathway in dendritic cells and Th17, which could result in chronically inflamed tissues producing high levels of IL-1534. Thus, serum IL-15 levels were higher in GC patients that consume large amounts of fried foods34. Similarly, Vahid and Davoodi (2021) showed that the risk of GC increased as it is associated with excessive consumption of fried foods at high temperatures and the frequent use of oil when cooking24. According to a meta-analysis study, fried food intake is positively correlated with gastric cancer risk35. The body converts nitrate to nitrite during metabolic processes, and nitrite has been linked to cancer development35. Therefore, a high nitrate intake can increase gastric cancer risk35. Nitrate content in foods is modulated by the cooking process35. In an additional study evaluating the risk of nitrate in vegetables, the cooking methods applied to raw vegetables resulted in a reduction of nitrate content, ranging from 4.094% to 59%. Notably, the boiling process exhibited the most substantial decrease, ranging from 47% to 59%36 37. In contrast, frying vegetables increases nitrate content (12.46–29.93%)36 37. It has been shown that frying oil is four-fold more likely to cause digestive cancers if it is reused more than four times35. Depending on the temperature and duration of cooking, the harmful components of frying oil can have different impacts35. However, Aljumaily et al. (2023) showed that sautéed or fried vegetables cooked in olive oil can protect against gastric cancer in the second and third tertiles (AOR = .55 (.31-.97) and AOR = .53 (.32-.87))38. In fact, virgin olive oil consumption has been linked to protection against cancer due to its high content of polyphenols38. Polyphenols are natural substances found in olive oil that have antioxidant, anti-cancer, and anti-inflammatory properties38. Therefore, it protects against oxidative damage and helps regulate the immune system38. Additionally, individuals with the highest intake of olive oil have been found to have a 23% lower risk of gastric cancer39. Overall, limiting fried food consumption can help to avoid stomach cancer and pre-cancerous lesions, but using virgin olive oil as a substitute to sautéed or fried vegetables can protect against the development of gastric cancer.
Salty foods and GC
According to the World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR), salt is one of the most major risk factors for stomach cancer40. Fang et al. (2015) demonstrated that excessive salt consumption has been linked to an increased risk of stomach cancer in earlier research41. According to estimates, more than 6 grams of salt per day was linked to 24% of stomach cancer incidences in the UK (31% in males and 12% in women) 42. According to the meta-analysis that was conducted by D’Elia et al. (2012), people who consume high amounts of salt have a greater risk of stomach cancer than those who consume less salt43. Furthermore, a Korean cohort research found that people who consumed more salty meals had a higher risk of stomach cancer (Kim et al., 2010)44. Moreover, Ge et al. (2012) found that a high salt diet raised the incidence of stomach cancer by 22%45. Umesawa et al. (2016) reported that even after controlling for sodium consumption, there was a significant link between salty food choices and the risk of stomach cancer by approximately 30%46. Several epidemiological studies have found a link between salty pickle consumption and the incidence of stomach cancer46. However, in this study there was no link 46. Furthermore, Kim et al. (2022) found a significant correlation between salty food and GC, and high sodium consumption can contribute to gastritis and mucosal irritation by damaging the mucosal barrier (relative risk = 1.68, 95% CI = 1.17–2.41)47. Wu et al. (2021) showed an increase in GC risk associated with high and moderate salt intakes48. There is a high probability (RR: 1.25; 95%CI: 1.10-1.41); P = 0.001) or moderate probability (RR: 1.20; 95%CI: 1.04-1.38; P = 0.012)48. Additionally, Vahid and Davoodi (2021) demonstrated that higher risk of GC was associated with salt consumption24. In the presence of H. pylori infection, salt may have synergistic effects, including strengthening cytotoxin-associated gene A(CagA) expression, increasing mucus viscosity, inducing epithelial damage, increasing inflammatory responses, and causing hypergastrinemia24. Likewise, Yang et al. (2020) reported that GC may be increased by high salt intake, particularly in the presence of H. pylori infection and atrophic gastritis49. In summary, excessive salt intake amplifies gastric carcinogens like N-methyl-N-nitro-N-nitrosoguanidine and can act as a stimulant to the gastric mucosa, leading to atrophic gastritis, accelerated DNA synthesis, and increased cell proliferation.
Milk and dairy products and GC
Wang et al. (2018) has found a strong relation between dairy consumption and the risk of stomach cancer50. Qin et al. (2004) stated that oestrogen found in milk may have a role in the development of prostate cancer, but it may also protect against stomach cancer51. However, in the study that was conducted by Sun et al. (2014), the intake of dairy products was linked to a non-significant increase in the incidence of stomach cancer52. Furthermore, Tayyem et al. (2022) documented an association between a high-dairy diet and a reduced risk of gastric cancer mortality specifically among males53. The multivariate hazard ratios were 0.82 (95% CI: 0.61–1.10), 0.74 (95% CI: 0.54–1.01), and 0.72 (95% CI: 0.52–0.99)53. On the other hand, an Italian study found that a diet high in dairy products is associated with a higher risk of GC (OR, 2.13; 95% CI, 1.34–3.40)54. Moreover, Kwak et al. (2021) showed that dairy products have some components that could potentially increase the risk of GC and other components that could decrease it (e.g., calcium, potassium, magnesium, riboflavin, vitamin B12, and insulin-like growth factor I)55. There was a positive association between dairy product consumption and lower GC risk (RR=0.76; 95% CI, 0.64-0.91)55. The result found was explained by the fact that dairy products may alleviate symptoms such as indigestion55. In addition, Gunathilake et al. (2021) found a significant positive correlation between a high dairy pattern score and a low microbial dysbiosis index with a lower risk of GC in females (OR = 0.23; 95% CI: 0.07-0.76; p-interaction = 0.018)56. In response to metabolic imbalances and microbial dysbiosis, probiotic-containing dairy products reduce the levels of several cancer-related biomarkers and increase IFN-γ production resulting in anticancer effects56. As a result, a dairy product such as fermented milk should be consumed daily to decrease the risk of GC56. Controversially, Asfari et al. (2022) demonstrated that intake of dairy products was associated with GC development (OR=2.28)57. Cows are exposed to several carcinogens in feedstuffs such as bracken fern, which could lead to GC development. In addition, cows’ milk is contaminated with pesticides that are shown to be carcinogenic or tumour promoters.
Food and dietary patterns and GC
Nemati et al. (2012) showed that dietary habits and H. pylori infection were the two most important factors linked to stomach cancer16. Regular consumption of vegetables and fruits, especially citrus fruits, was found to lower the incidence of stomach cancer16. Unsaturated fat consumption has also been demonstrated to protect against the development of stomach cancer16. Drinking hot tea was linked to a nearly twice increase in the incidence of stomach cancer16. A study conducted by Abnet el al. (2015) showed that eating habits that included more fruits and vegetables, were linked to a lower risk of stomach cancer and gastric adenocarcinoma (OR, 0.63)58. The same study demonstrated that diet high in meat and nitrates was strongly linked to a greater incidence of stomach adenocarcinomas (OR, 2.40)58. Moreover, Kim et al. (2021) conducted a study including two dietary patterns: westernized and prudent patterns59. The westernized pattern consists of a high amount of meat and other animal items, and the prudent pattern contains a high amount of vegetables and fruits59. The prudent pattern was found to lower the incidence of GC59. As a result, adherence to a healthy dietary pattern, which is characterized by high consumption of fruits and vegetables, is beneficial in lowering the incidence of GC59.
Fat and sweets intake and GC
There are controversial findings about the association between dietary fat intake and GC. Several studies have found that high intake of total fat was positively correlated with GC7 8 60. Despite the fact that many case-control studies have indicated that a high dietary fat intake may increase the risk of stomach cancer8, other studies showed an inverse effect of dietary fat on GC7. Since cholesterol is ingested in conjunction with other substances such as salt, nitrates, multivitamins, minerals, and high-quality protein, the interplay of multiple nutrients precludes us from fully comprehending cholesterol’s particular effect. Total fat, saturated fat, and cholesterol intake were all found to be substantially linked to the risk of stomach cancer, with ORs of 1.58 (95 percent CI 1.13–2.20), 1.86 (95 percent CI 1.37–2.52), and 1.75 (95 percent CI 1.36–2.25) for the highest quartile against the lowest quartile, respectively60. In addition, it was reported that long-term high sugar or carbohydrate intake could lead to chronic hyperinsulinemia61-63. In fact, hyperglycemia may cause insulin release and consecutively lead to a hyperinsulinemia64. The risk of developing cancer will increase through insulin signaling pathway64. Moreover, foods or beverages high in sugar content are low in fiber and micronutrients that help with digestion65. Refined sugar causes acute fluctuations in blood sugar levels, which may lead to oxidative stress and modulate carcinogenic pathways63 66-68.
Alcohol consumption and GC
The association between alcohol consumption and the risk of GC has been proved by many studies69-73. Dong and Thrift (2017) stated that consumption of alcohol is a known high-risk factor GC69. Moreover, Li et al. (2021) explains that alcohol consumption has been linked to an increased risk of stomach cancer70. In addition, Ma et al. (2017) indicated that the findings of a meta-analysis back up the theory that drinking alcohol raises the risk of GC71. Moreover, Moy et al. (2010) found that alcohol consumption may have independent impacts on the development of GC in this high-risk population72. However, the apparent link between alcohol consumption, particularly hard liquor, and the incidence of stomach cancer may be due to nitrosamines found in alcoholic beverages72. A meta-analysis shows that there is no link between moderate alcohol consumption and the risk of GC73. However, heavy alcohol consumption was linked to a higher risk73. A study found that alcohol intake raises the incidence of GC (odds ratio (OR) of 1.39) (Ma et al., 2017)71. Tramacere et al. supported the relationship between the risk of stomach cancer and heavy alcohol consumption (four drinks per day)73. Moreover, a study found that people that consume more than 50g of alcohol per day had a 24% higher chance of developing stomach cancer than others that did not drink alcohol or consumed less74. Alcohol can help to induce a cancer-stimulating mechanism involving a chronic inflammatory response to the toxic effects of ethanol metabolites40 and stimulates cytokines secretion, thereby increasing nitrosamine intake40.
Smoking
Research showed the role of tobacco smoking in the development of stomach cancer. A study conducted in 2017 stated that smoking has been identified as a major risk factor for stomach cancer in previous research69. Additionally, a study demonstrated that male smokers have a 60% greater risk of GC, whereas female smokers have a 20% increased risk. Another study showed that among previous male smokers, a shorter time since quitting resulted in a higher risk, even after cigarette-years were taken into consideration. This builds on the evidence that there is a link between cigarette smoking and stomach cancer and it shows that smoking may be a risk factor for developing GC. Moreover, the link between cigarette smoking and the risk of stomach cancer is confirmed by the worldwide dataset. A study revealed that current smokers have a 25% higher risk of developing stomach cancer75. When compared to never smokers, the risk increased dramatically with cigarette smoking intensity and duration, reaching 32% for smokers who smoke more than 20 cigarettes per day and 33% for smokers who had smoked for more than 40 years76. In addition, Shah and Bentrem (2022) stated that cigarette smoking, like many other malignancies, is a risk factor for stomach cancer77. Smokers have a 1.5–1.8 times increased chance of developing stomach cancer than non-smokers77. There is ongoing study about the mechanisms underlying how smoking affects cancer in the stomach77. Cigarette smoke contains a range of carcinogenic components77. Possible mechanisms include DNA adduct production, stimulation of tumor angiogenesis, activation of nicotinic cholinergic receptors, and induction of cell proliferation77.
Physical activity (PA)
Most of the researchers found a relationship between PA and GC. Abioy et al. (2015) stated that regular physical activity may lower the risk of stomach cancer78. McTiernan et al. (2019) showed strong evidence that physical activity lowers cancer risk79. Moreover, Singh et al. (2015) indicated that the incidence of overall and site-specific GC is lower among the most physically active persons than among the least physically active people 80. In fact, it has been demonstrated that physical activity might reduce chronic inflammation by reducing interleukin-6 and tumour necrosis factor-α, partly through fat loss80. Additionally, Psaltopoulou et al. (2016) showed in their meta-analysis that physical activity can reduce the risk of stomach cancer, particularly in Asian populations81. Moreover, case-control study showed a relationship between GC and PA82. The study found that people with highest PA level were 78% less likely to have GC82.
Medication
There is an association between the intake of medication and the risk of developing GC. Seven randomized meta-analysis studies have found that treatment of H. pylori can reduce GC risk by 35%1. It has been reported that indirect effect of H. pylori on gastric epithelial cells through generating inflammation and direct action of the bacteria on epithelial cells are the two most common mechanisms. Results indicates H. pylori may directly regulate epithelial cell activity through bacterial compounds like cytotoxin-associated gene A (CagA).
Treating H. pylori can reduce the likelihood of future gastric cancer incidence in healthy, asymptomatic individuals infected with the bacterium83. In preventing development of subsequent gastric cancer, H. pylori eradication therapy was superior to placebo or no treatment (RR = 0.66; 95% CI 0.46 to 0.95)83. Studies have indicated that eradicating H. pylori can be advantageous in preventing the future development of GC 8. In individuals with H. pylori infection who had a family history of gastric cancer among first-degree relatives, undergoing H. pylori eradication treatment decreased the risk of developing gastric cancer84.
Additional observational studies suggest that the use of non-steroidal anti-inflammatory drugs (NSAIDs) and statins may decrease the incidence of stomach cancer. Furthermore, individuals diagnosed with type 2 diabetes who take metformin may have a reduced risk of gastric cancer. However, the use of sulfonylureas might be linked to an increased risk of gastric cancer85.
Non-modifiable risk factors associated with gastric cancer
Age
Many researches revealed that the impact of GC varies by age group86 87. Asaka et al. (2020) showed that preventing all cancers, not only GC, is extremely difficult in people over the age of 80, implying that cancer preventive methods should be evaluated separately for people under the age of 80 and those above the age of 8086. Furthermore, studies found that participants with a higher age had a higher susceptibility for screening87. Screening acceptance rises with age, with the highest rate of screening reported among those aged 50–59. As a result, age, education level, and household income are all factors that influence stomach cancer screening87. Moreover, Shah and Bentrem (2022) stated that with aging, the chance of stomach cancer rises77. Indeed, the increased risk of gastric cancer with age can be attributed to various factors. Prolonged exposure to potential carcinogens, along with heightened susceptibility to mucosal damage and delayed healing of gastric mucosa, are significant contributors. Additionally, older individuals may exhibit elevated levels of mucosal cancer stem cell markers, a greater prevalence of chronic active gastritis, intestinal metaplasia, and mucosal atrophy, particularly in those infected with H. pylori. These combined factors create a conducive environment for the development of gastric cancer as individuals age77.
Sex
The risk of GC is higher in men than women. Li et al. (2020) found that men had larger, more advanced, and higher-grade GC than women88. Furthermore, Rawla and Barsouk (2019) indicated that females have a significantly lower rate of GC than males89. It might be explained by the estrogen’s preventive impact reducing the risk of stomach cancer in women89. In addition, Shah and Bentrem (2022) showed that GC affects men twice as frequently as it affects women77. Studies attempting to explain the difference in incidence between men and women have yielded conflicting results77. These studies looked at sociodemographic traits, environmental factors, sex hormones, hormonal therapies, and smoking habits77. However, men tend to have a higher prevalence of H. pylori infection, which presumably plays a role in the difference of stomach cancer incidence observed in both genders77.
Family history (FH)
Many research have confirmed the link between FH and the risk of GC90-92. Man et al. (2021) stated that family history of early-onset cancer is strongly associated with the development of GC, with an OR ranging from 1.77 to 3.2790. Elevated GC risk is connected to genetic background characteristics such as IL-17 polymorphisms and cell proliferation-related genetic polymorphisms, which can explain part of the link between family history and an increased risk of GC90. Additionally, Yaghoobi et al. (2010) reported that a strong and constant risk factor for GC is a positive family history, but the molecular basis for the aggregation is mainly unknown92. In addition, Song et al. (2018) stated that specific subtypes of GC are closely linked to a family history of GC91.
Genetics
Many studies showed that genetic risk factors play a big role in developing GC89 93 94. Rawla and Barsouk (2019) indicated that certain inherited gene mutations, such as the GSTM1-null phenotype or the CDH1 gene, have been linked to an increased risk of stomach cancer. Hereditary differentiated GC (HDGC) is an autosomal dominantly inherited disorder in which malignant cells proliferate beneath the stomach lining and metastasize as a result of the loss of one of the CDH1 gene’s copies89. Additionally, Slavin et al. (2019) stated that many well-known genetic disorders carry a risk of GC94. These syndromes are frequently linked to a higher risk of non-gastric malignancies94. Furthermore, Lu et al. (2015) reported that the impact of DNA damage and repair in the development of stomach cancer cannot be overstated93. Additionally, Shah and Bentrem (2022) showed that there are many genetic syndromes affecting GC such as Hereditary diffuse GC, Hereditary nonpolyposis colorectal cancer, Familial adenomatous polyposis, Gastric adenocarcinoma and proximal polyposis of the stomach, MUTYH‐associated polyposis, Juvenile polyposis syndrome, Peutz–Jegher syndrome and Li–Fraumeni syndrome77.
Blood type
There is an association between the blood group A and the risk of GC. Zhang et al. (2014) indicate that blood group A is linked to a higher risk of cancer, while blood group O is linked to a lower risk of cancer95. Moreover, Goral (2016) stated that GC is more common in people with blood type A, but this is thought to be due to genes rather than blood type antigens96. In addition, Benbrahim et al. (2017) reported that people with blood group A had a 20% higher risk of stomach cancer than those with blood groups O, B, or AB97. Moreover, Shah and Bentrem (2022) demonstrated that compared to other blood types, group A blood carriers have a higher relative risk (1.11–1.21) of developing stomach cancer77. Multiple mechanisms have been proposed to explain this association, including alterations in gastric secretory function, intracellular adhesion receptors, membrane signaling, immune surveillance, inflammatory responses to H. pylori and cancer cells, and heightened susceptibility to pernicious anemia77.
Conclusion
In summary, this review showed that high consumption of fried and fast foods, salty foods and alcohol, smoking, advanced age, male sex, family history, genetics, and blood type A may increase the risk of GC; whereas physical activity, consumption of fruits and vegetables that are rich in antioxidants, fiber, and polyphenols might play a protective role against GC. Dietary patterns characterized by high consumption of red and processed meats was associated with an elevated risk of GC. Studies found controversial results related to body weight and body fat, medications, milk and dairy products, fat and sweets consumption with the risk of GC. Further research is needed to define the efficacy of diet and behavioral modifications in the prevention and treatment of gastric cancer as well as determine and clarify the underlying reasons behind gender differences in the relationship between dietary patterns and GC risk.
Acknowledgement
None
Funding Sources
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of Interest
The authors declare that they have no any competing or conflict of interest.
Author Contributions
All authors contributed to writing this review, all approved the final version to be published.
Ethics Policies
This research did not request ethical approval.
References
- Bosman FT, Carneiro F, Hruban RH, et al. WHO classification of tumours of the digestive system: World Health Organization 2010.
- Piazuelo MB, Correa P. Gastric cancer: overview. Colombia Medica 2013;44(3):192-201.
CrossRef - Jemal A, Center MM, DeSantis C, et al. Global patterns of cancer incidence and mortality rates and trends. Cancer Epidemiology and Prevention Biomarkers 2010;19(8):1893-907.
CrossRef - Smyth EC, Nilsson M, Grabsch HI, et al. Gastric cancer. Lancet 2020;396(10251):635-48.
CrossRef - Yusefi AR, Bagheri Lankarani K, Bastani P, et al. Risk Factors for Gastric Cancer: A Systematic Review. Asian Pac J Cancer Prev 2018;19(3):591-603.
- Ko K-P. Risk Factors of Gastric Cancer and Lifestyle Modification for Prevention. J Gastric Cancer 2024;24(1):99-107.
CrossRef - Goff DC, Lloyd-Jones DM, Bennett G, et al. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Journal of the American College of Cardiology 2014;63(25 Part B):2935-59.
CrossRef - Fuccio L, Zagari RM, Eusebi LH, et al. Meta-analysis: can Helicobacter pylori eradication treatment reduce the risk for gastric cancer? Annals of internal medicine 2009;151(2):121-28.
CrossRef - Lin X-J, Wang C-P, Liu X-D, et al. Body mass index and risk of gastric cancer: a meta-analysis. Japanese journal of clinical oncology 2014;44(9):783-91.
CrossRef - Nieman KM, Romero IL, Van Houten B, et al. Adipose tissue and adipocytes support tumorigenesis and metastasis. Biochimica et Biophysica Acta (BBA)-Molecular and Cell Biology of Lipids 2013;1831(10):1533-41.
CrossRef - Li Q, Zhang J, Zhou Y, et al. Obesity and gastric cancer. Frontiers in bioscience (Landmark edition) 2012;17:2383-90.
CrossRef - Liu AR, He QS, Wu WH, et al. Body composition and risk of gastric cancer: A population‐based prospective cohort study. Cancer medicine 2021;10(6):2164-74.
CrossRef - Bae J-M, Kim EH. Dietary intakes of citrus fruit and risk of gastric cancer incidence: an adaptive meta-analysis of cohort studies. Epidemiology and health 2016;38
CrossRef - Cover TL, Peek J, Richard M. Diet, microbial virulence, and Helicobacter pylori-induced gastric cancer. Gut microbes 2013;4(6):482-93.
CrossRef - Farmanfarma KK, Mahdavifar N, Hassanipour S, et al. Epidemiologic study of gastric cancer in iran: a systematic review. Clinical and Experimental Gastroenterology 2020;13:511.
- Nemati A, Mahdavi R, Baghi AN. Case-control study of dietary pattern and other risk factors for gastric cancer. Health promotion perspectives 2012;2(1):20.
- Schwingshackl L, Schwedhelm C, Galbete C, et al. Adherence to Mediterranean diet and risk of cancer: an updated systematic review and meta-analysis. Nutrients 2017;9(10):1063.
CrossRef - Wang Q, Chen Y, Wang X, et al. Consumption of fruit, but not vegetables, may reduce risk of gastric cancer: results from a meta-analysis of cohort studies. European Journal of Cancer 2014;50(8):1498-509.
CrossRef - Kim SR, Kim K, Lee SA, et al. Effect of red, processed, and white meat consumption on the risk of gastric cancer: an overall and dose–response meta-analysis. Nutrients 2019;11(4):826.
CrossRef - Tayyem RF, Nawaiseh H, Al‐Awwad N, et al. Meat and dairy products intake is associated with gastric cancer: Case–control study findings. Food Science & Nutrition 2023
CrossRef - Zhao Z, Yin Z, Zhao Q. Red and processed meat consumption and gastric cancer risk: A systematic review and meta-analysis. Oncotarget 2017;8(18):30563.
CrossRef - Huang Y, Cao D, Chen Z, et al. Red and processed meat consumption and cancer outcomes: Umbrella review. Food Chemistry 2021;356:129697.
CrossRef - Collatuzzo G, Etemadi A, Sotoudeh M, et al. Meat consumption and risk of esophageal and gastric cancer in the Golestan Cohort Study, Iran. International Journal of Cancer 2022
CrossRef - Vahid F, Davoodi SH. Nutritional factors involved in the etiology of gastric cancer: a systematic review. Nutrition and cancer 2021;73(3):376-90.
CrossRef - Poorolajal J, Moradi L, Mohammadi Y, et al. Risk factors for stomach cancer: a systematic review and meta-analysis. Epidemiology and health 2020;42
CrossRef - Wilunda C, Yamaji T, Iwasaki M, et al. Meat consumption and gastric cancer risk: the Japan Public Health Center–based Prospective Study. The American Journal of Clinical Nutrition 2022;115(3):652-61.
CrossRef - Corpet DE. Red meat and colon cancer: should we become vegetarians, or can we make meat safer? Meat science 2011;89(3):310-16.
CrossRef - Guo L, Liu S, Zhang M, et al. Multivariate analysis of the association between consumption of fried food and gastric cancer and precancerous lesions. Zhonghua yu Fang yi xue za zhi [Chinese Journal of Preventive Medicine] 2018;52(2):170-74.
- Wu X, Zhang Q, Guo H, et al. Dietary patterns and risk for gastric cancer: A case-control study in residents of the Huaihe River Basin, China. Frontiers in Nutrition 2023;10:1118113.
CrossRef - Koszucka A, Nowak A, Nowak I, et al. Acrylamide in human diet, its metabolism, toxicity, inactivation and the associated European Union legal regulations in food industry. Critical reviews in food science and nutrition 2020;60(10):1677-92.
CrossRef - Li L, Ni J, Sun S, et al. Clinical applicability of a new scoring system for population-based screening and risk factors of gastric cancer in the Wannan region. BMC gastroenterology 2022;22(1):1-9.
CrossRef - Duan F, Song C, Shi J, et al. Identification and epidemiological evaluation of gastric cancer risk factors: based on a field synopsis and meta-analysis in Chinese population. Aging (albany NY) 2021;13(17):21451.
CrossRef - Ghaffari HR, Yunesian M, Nabizadeh R, et al. Environmental etiology of gastric cancer in Iran: a systematic review focusing on drinking water, soil, food, radiation, and geographical conditions.
Environmental science and pollution research 2019;26(11):10487-95.
CrossRef - Sun X, Xiang CJ, Wu J, et al. Relationship between serum inflammatory cytokines and lifestyle factors in gastric cancer. Molecular and clinical oncology 2019;10(3):401-14.
CrossRef - Zhang T, Song SS, Liu M, et al. Association of Fried Food Intake with Gastric Cancer Risk: A Systemic Review and Meta-Analysis of Case–Control Studies. Nutrients 2023;15(13):2982.
CrossRef - Prasad S, Chetty AA. Nitrate-N determination in leafy vegetables: Study of the effects of cooking and freezing. Food Chemistry 2008;106(2):772-80.
CrossRef - Salehzadeh H, Maleki A, Rezaee R, et al. The nitrate content of fresh and cooked vegetables and their health-related risks. PLoS One 2020;15(1):e0227551.
CrossRef - Aljumaily M, Al-Naimi N, Al-Amer R, et al. Consumption of Fruits and Vegetables and Gastric Cancer Risk: Answers From Case-Control Study. American Journal of Lifestyle Medicine 2023:15598276231222880.
CrossRef - Markellos C, Ourailidou M-E, Gavriatopoulou M, et al. Olive oil intake and cancer risk: A systematic review and meta-analysis. PLoS One 2022;17(1):e0261649.
CrossRef - Yusefi AR, Lankarani KB, Bastani P, et al. Risk factors for gastric cancer: a systematic review. Asian Pacific journal of cancer prevention: APJCP 2018;19(3):591.
- Fang X, Wei J, He X, et al. Landscape of dietary factors associated with risk of gastric cancer: A systematic review and dose-response meta-analysis of prospective cohort studies. European Journal of Cancer 2015;51(18):2820-32.
CrossRef - Parkin D. 7. Cancers attributable to dietary factors in the UK in 2010. British Journal of Cancer 2011;105(2):S31-S33.
CrossRef - D’Elia L, Rossi G, Ippolito R, et al. Habitual salt intake and risk of gastric cancer: a meta-analysis of prospective studies. Clinical nutrition 2012;31(4):489-98.
CrossRef - Kim J, Park S, Nam B-H. Gastric cancer and salt preference: a population-based cohort study in Korea. The American journal of clinical nutrition 2010;91(5):1289-93.
CrossRef - Ge S, Feng X, Shen L, et al. Association between habitual dietary salt intake and risk of gastric cancer: a systematic review of observational studies. Gastroenterology research and practice 2012;2012
CrossRef - Umesawa M, Iso H, Fujino Y, et al. Salty food preference and intake and risk of gastric cancer: the JACC study. Journal of epidemiology 2016;26(2):92-97.
CrossRef - Kim SY, Kwak JH, Eun CS, et al. Gastric Cancer Risk Was Associated with Dietary Factors Irritating the Stomach Wall: A Case–Control Study in Korea. Nutrients 2022;14(11):2233.
CrossRef - Wu B, Yang D, Yang S, et al. Dietary salt intake and gastric cancer risk: a systematic review and meta-analysis. Frontiers in nutrition 2021;8
CrossRef - Yang L, Ying X, Liu S, et al. Gastric cancer: Epidemiology, risk factors and prevention strategies. Chinese Journal of Cancer Research 2020;32(6):695.
CrossRef - Wang S, Zhou M, Ji A, et al. Milk/dairy products consumption and gastric cancer: an update meta-analysis of epidemiological studies. Oncotarget 2018;9(6):7126.
CrossRef - Qin L-Q, Wang P-Y, Kaneko T, et al. Estrogen: one of the risk factors in milk for prostate cancer. Medical hypotheses 2004;62(1):133-42.
CrossRef - Sun Y, Lin L-J, Sang L-X, et al. Dairy product consumption and gastric cancer risk: a meta-analysis. World Journal of Gastroenterology: WJG 2014;20(42):15879.
CrossRef - Tayyem R, Al-Awwad N, Allehdan S, et al. Mediterranean Dietary Pattern is Associated with Lower Odds of Gastric Cancer: A Case–Control Study. Cancer Management and Research 2022;14:2017.
CrossRef - Bertuccio P, Edefonti V, Bravi F, et al. Nutrient Dietary Patterns and Gastric Cancer Risk in ItalyDietary Patterns and Gastric Cancer Risk. Cancer epidemiology, biomarkers & prevention 2009;18(11):2882-86.
CrossRef - Kwak JH, Park CH, Eun CS, et al. Dietary intake of soy products, vegetables, and dairy products and gastric cancer survival according to histological subtype: a long-term prospective cohort study. Journal of Gastric Cancer 2021;21(4):403.
CrossRef - Gunathilake M, Lee J, Choi IJ, et al. Effect of the Interaction between Dietary Patterns and the Gastric Microbiome on the Risk of Gastric Cancer. Nutrients 2021;13(08):2692.
CrossRef - Asfari MM, Hamid O, Sarmini MT, et al. The Association of Lactose Intolerance With Colon and Gastric Cancers: Friend or Foe? Cureus 2022;14(5).
CrossRef - Abnet CC, Corley DA, Freedman ND, et al. Diet and upper gastrointestinal malignancies. Gastroenterology 2015;148(6):1234-43. e4.
CrossRef - Kim JH, Lee J, Choi IJ, et al. Dietary patterns and gastric cancer risk in a Korean population: A case–control study. European journal of nutrition 2021;60(1):389-97.
CrossRef - Hu J, La Vecchia C, Negri E, et al. Macronutrient intake and stomach cancer. Cancer causes & control 2015;26(6):839-47.
CrossRef - Petrick JL, Li N, McClain KM, et al. Dietary risk reduction factors for the Barrett’s esophagus-esophageal adenocarcinoma continuum: a review of the recent literature. Current nutrition reports 2015;4(1):47-65.
CrossRef - Lahmann PH, Ibiebele TI, Webb PM, et al. A case-control study of glycemic index, glycemic load and dietary fiber intake and risk of adenocarcinomas and squamous cell carcinomas of the esophagus: the Australian Cancer Study. BMC cancer 2014;14(1):1-12.
CrossRef - Kubo A, Corley DA, Jensen CD, et al. Dietary factors and the risks of oesophageal adenocarcinoma and Barrett’s oesophagus. Nutrition research reviews 2010;23(2):230-46.
CrossRef - Warburg O. On the origin of cancer cells. Science 1956;123(3191):309-14.
CrossRef - Li N, Petrick JL, Steck SE, et al. A pooled analysis of dietary sugar/carbohydrate intake and esophageal and gastric cardia adenocarcinoma incidence and survival in the USA. International journal of epidemiology 2017;46(6):1836-46.
CrossRef - Herrigel DJ, Moss RA. Diabetes mellitus as a novel risk factor for gastrointestinal malignancies. Postgraduate medicine 2014;126(6):106-18.
CrossRef - Kaaks R, Lukanova A. Energy balance and cancer: the role of insulin and insulin-like growth factor-I. Proceedings of the nutrition society 2001;60(1):91-106.
CrossRef - Willett W, Manson J, Liu S. Glycemic index, glycemic load, and risk of type 2 diabetes. The American journal of clinical nutrition 2002;76(1):274S-80S.
CrossRef - Dong J, Thrift AP. Alcohol, smoking and risk of oesophago-gastric cancer. Best practice & research Clinical gastroenterology 2017;31(5):509-17.
CrossRef - Li Y, Eshak ES, Shirai K, et al. Alcohol consumption and risk of gastric cancer: The Japan Collaborative Cohort study. Journal of epidemiology 2021;31(1):30-36.
CrossRef - Ma K, Baloch Z, He T-T, et al. Alcohol consumption and gastric cancer risk: a meta-analysis. Medical science monitor: international medical journal of experimental and clinical research 2017;23:238.
CrossRef - Moy KA, Fan Y, Wang R, et al. Alcohol and tobacco use in relation to gastric cancer: a prospective study of men in Shanghai, China. Cancer Epidemiology and Prevention Biomarkers 2010;19(9):2287-97.
CrossRef - Tramacere I, Negri E, Pelucchi C, et al. A meta-analysis on alcohol drinking and gastric cancer risk. Annals of oncology 2012;23(1):28-36.
CrossRef - Bagnardi V, Rota M, Botteri E, et al. Alcohol consumption and site-specific cancer risk: a comprehensive dose–response meta-analysis. British journal of cancer 2015;112(3):580-93.
CrossRef - Ladeiras-Lopes R, Pereira AK, Nogueira A, et al. Smoking and gastric cancer: systematic review and meta-analysis of cohort studies. Cancer causes & control 2008;19(7):689-701.
CrossRef - Praud D, Rota M, Pelucchi C, et al. Cigarette smoking and gastric cancer in the Stomach Cancer Pooling (StoP) Project. European Journal of Cancer Prevention 2018;27(2):124-33.
CrossRef - Shah D, Bentrem D. Environmental and genetic risk factors for gastric cancer. Journal of surgical oncology 2022;125(7):1096-103.
CrossRef - Abioye AI, Odesanya MO, Abioye AI, et al. Physical activity and risk of gastric cancer: a meta-analysis of observational studies. British journal of sports medicine 2015;49(4):224-29.
CrossRef - McTiernan A, Friedenreich CM, Katzmarzyk PT, et al. Physical activity in cancer prevention and survival: a systematic review. Medicine and science in sports and exercise 2019;51(6):1252.
CrossRef - Singh S, Varayil JE, Devanna S, et al. Physical activity is associated with reduced risk of gastric cancer: a systematic review and meta-analysis. Cancer Prevention Research 2014;7(1):12-22.
CrossRef - Psaltopoulou T, Ntanasis-Stathopoulos I, Tzanninis I-G, et al. Physical activity and gastric cancer risk: a systematic review and meta-analysis. Clinical Journal of Sport Medicine 2016;26(6):445-64.
CrossRef - Fagundes MA, Peres SV, Assumpção PP, et al. Physical activity and gastric cancer risk: a case-control study in the Amazon region of Brazil. European Journal of Cancer Prevention 2021;30(6):437-41.
CrossRef - Ford AC, Forman D, Hunt R, et al. Helicobacter pylori eradication for the prevention of gastric neoplasia. Cochrane database of systematic reviews 2015(7)
CrossRef - Choi IJ, Kim CG, Lee JY, et al. Family history of gastric cancer and Helicobacter pylori treatment. New England Journal of Medicine 2020;382(5):427-36.
CrossRef - Miao Z-F, Xu H, Xu Y-Y, et al. Diabetes mellitus and the risk of gastric cancer: a meta-analysis of cohort studies. Oncotarget 2017;8(27):44881.
CrossRef - Asaka M, Kobayashi M, Kudo T, et al. Gastric cancer deaths by age group in Japan: outlook on preventive measures for elderly adults. Cancer science 2020;111(10):3845-53.
CrossRef - Hatamian S, Etesam S, Mazidimoradi A, et al. The Barriers and Facilitators of Gastric Cancer Screening: a Systematic Review. Journal of Gastrointestinal Cancer 2021;52(3):839-45.
CrossRef - Li H, Wei Z, Wang C, et al. Gender differences in gastric cancer survival: 99,922 cases based on the SEER database. Journal of Gastrointestinal Surgery 2020;24(8):1747-57.
CrossRef - Rawla P, Barsouk A. Epidemiology of gastric cancer: global trends, risk factors and prevention. Przeglad gastroenterologiczny 2019;14(1):26.
CrossRef - Man J, Ni Y, Yang X, et al. Healthy Lifestyle Factors, Cancer Family History, and Gastric Cancer Risk: A Population-Based Case-Control Study in China. Frontiers in nutrition 2021;8
CrossRef - Song M, Camargo MC, Weinstein SJ, et al. Family history of cancer in first-degree relatives and risk of gastric cancer and its precursors in a Western population. Gastric Cancer 2018;21(5):729-37.
CrossRef - Yaghoobi M, Bijarchi R, Narod S. Family history and the risk of gastric cancer. British journal of cancer 2010;102(2):237-42.
CrossRef - Lu Y, Lu F, Zeng S, et al. Genetics and gastric cancer susceptibility. International Journal of Clinical and Experimental Medicine 2015;8(6):8377.
- Slavin TP, Weitzel JN, Neuhausen SL, et al. Genetics of gastric cancer: what do we know about the genetic risks? Translational gastroenterology and hepatology 2019;4
CrossRef - Zhang B-L, He N, Huang Y-B, et al. ABO blood groups and risk of cancer: a systematic review and meta-analysis. Asian Pacific Journal of Cancer Prevention 2014;15(11):4643-50.
CrossRef - Goral V. Etiopathogenesis of gastric cancer. Asian Pacific Journal of Cancer Prevention 2016;17(6):2745-50.
CrossRef - Benbrahim Z, Mekkaoui AE, Lahmidani N, et al. Gastric cancer: an epidemiological overview. Epidemiology (Sunnyvale) 2017;7(304):2161-1165.1000304.

This work is licensed under a Creative Commons Attribution 4.0 International License.








