
Introduction
Iron is recognized as an essential micronutrient for almost all living organisms since ancient times. Iron as a micronutrient is considered to be a double-edged sword which, in limits help in oxygen transport, DNA synthesis, cellular regeneration, and respiration. But, is toxic in overload states causing oxidative stress and cellular damage.1 70% of iron reserves in humans are found in blood haemoglobin and muscle myoglobin. Since the last decade, nutritional disorders associated with the dearth of iron in humans were reported affecting all age groups. Thus iron is considered to be the most common form of micronutrient malnutrition (MM) globally.2,3 Iron deficiencies are the most common MM considered to be a serious public issue affecting over 1.2 billion people globally, especially in pregnant women and children of low- and middle-income countries (Figure1).4,5,6,7 World Health Organization (WHO) estimates that two billion people are anaemic and attribute approximately 50% of all anaemics to Iron deficiency & Iron deficiency anaemia (ID & IDA).8 Mounting evidence suggests that the prevalence of iron deficiencies are characterized based on age groups (pediatrics, geriatrics), and gender (mostly women) (Figure 1).9,10,11,12,13,14 Iron deficiencies not only cause anemia but also leads to premature births, low birth weight babies, and affects overall physical and mental health.15,16,17 It is well documented that ID could be controlled by food along with a balanced diet in healthy humans. Poor health, increased vulnerability to various diseases, and a significant reduction in annual Gross Domestic Product (GDP), up to 11% in Asia and Africa, are all consequences of inadequate consumption of a healthy diet.18
The recommended daily intake of iron varies among different age groups including infants (11 mg), premenopausal women (18 mg), pregnancy (27 mg), and adult men (8 mg).19 The present review emphasizes a detailed note on the importance of iron, iron physiology and pathophysiology, the current nutrikinetic status of iron in different food interventions, and their future in dealing with iron malnutrition.
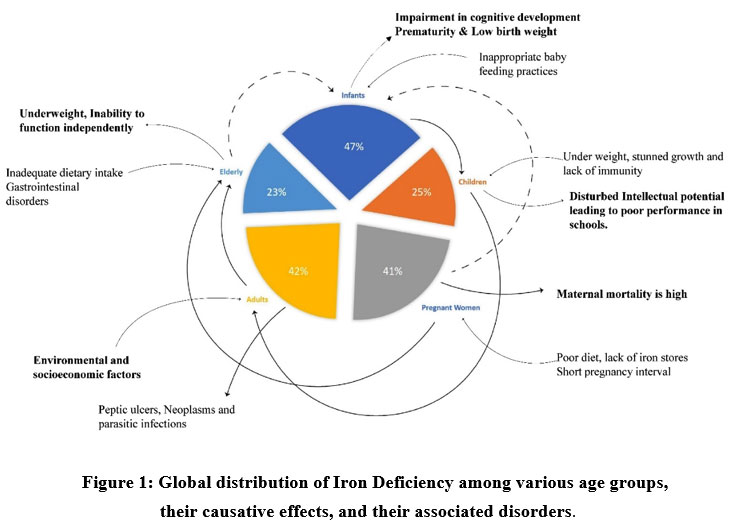 |
Figure 1: Global distribution of Iron Deficiency among various age groups, their causative effects, and their associated disorders. |
In the present systematic review, we have collected published articles from databases including a.) Web of Science b.) Elsevier c.) Scopus. Search engines like Google scholar, PubMed, INFLIBNET were used. Data was collected from research and review articles published between 1991 and 2021. Search keywords includes food fortification, bio fortification, iron fortification, iron nutrikinetics, iron bioavailability, and iron bio accessibility etc. The articles were chosen based on the relevance to the current review, with topics including iron malnutrition, iron deficiency anemia, WHO food interventions, socioeconomic status etc.
Physiological and Pathological Role of Iron
Iron from the diet is either sequestered as heme or nonheme forms. Non-heme forms are poorly absorbed whereas heme forms are most absorbed from basal membranes. In the intestine, nonheme iron, especially in ferrous state (Fe2+), gets absorbed into blood circulation via divalent metal transporter 1 (DMT-1). As the dietary iron is in ferric state (Fe3+), it gets transported across enterocyte basolateral membrane via FPN1 thereby getting reduced from Fe3+ to Fe2+ by the enzyme copper-dependent iron oxidase hephaestin (Figure 2).20 The absorbed iron bounds to plasma transferrin for further distribution to the utilization sites. Most of the transported iron is utilized by newly formed red blood cells in the bone marrow. Senescent red blood cells get phagocytosed by macrophages, causing catabolism of hemoglobin for releasing heme form which is transported to bone marrow.21 Hepcidin, a liver-derived peptide, regulates body iron demand for intake and distribution to enterocytes, macrophages, and other body cells. Free iron (Fe3+) gets sequestered with ferritin, an iron storage protein, then mixing with peptide hemosiderin, for storage and reuse in physiological functions. Defective transporters (i.e., DMT-1, FPN1, transferrin), deficiency of oxidizing enzymes, and lack of iron storage proteins are the key pathological factors that cause iron deficiencies.22
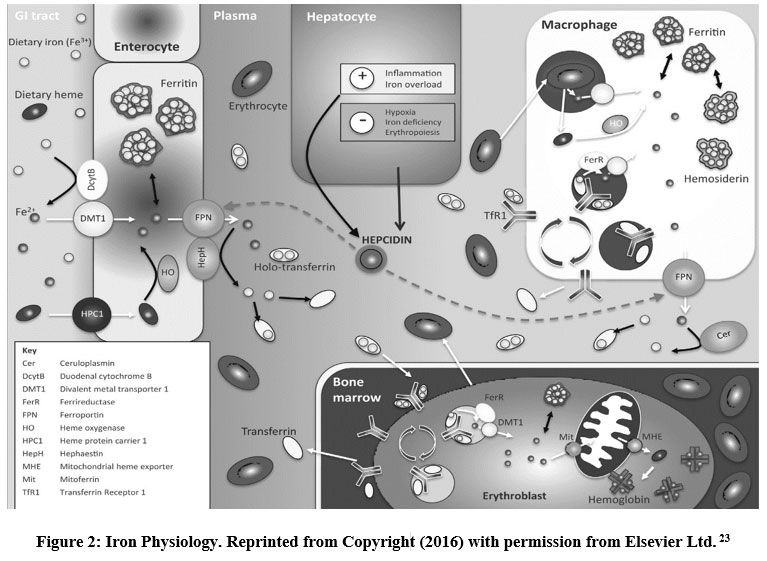 |
Figure 2: Iron Physiology. Reprinted from Copyright (2016) with permission from Elsevier Ltd. 23 |
Strategies for Enriching Iron Levels in Tackling ID and IDA
Heme and non-heme iron are the two forms available in food sources with different absorption rates in humans. Meat, fish, and seafood are the best sources of heme iron with 15-35% of the absorption rate. Seeds, grains, nuts, and green leafy vegetables majorly contribute to the non-heme iron but have a less absorption rate of 2-20%.24,25,26 To combat ID and IDA, governing bodies of various countries have taken different initiatives viz., iron supplements in the form of tablets, capsules, and syrups, dietary diversification including iron-rich foods. Also, initiatives for enhancement of iron absorption, fortified iron-rich foods, bio fortification of staple crops are encouraged.27
Iron supplementation with ferrous ion salts is considered a first-line treatment and is a provision for large doses of micronutrients, usually in the form of tablets, capsules, or syrups. It is considered the fastest means to control the micronutrient deficient population groups due to its low cost, high bioavailability, and effectiveness. The maternal and child nutrition report in the Lancet series documented that the iron supplementation trial reduced 67% of IDA in pregnant women.28 In another study, non-pregnant women of reproductive age showed a 27% reduced risk of anaemia by intermittent iron supplementation.29 Despite different success stories, a substantial proportion of the population consuming ferrous ion salts suffer from gastrointestinal side effects like nausea, epigastric pain, and constipation due to the higher iron doses administered leading to poor compliance.30,31 Adding to this, routine iron supplementation could lead to potential adverse effects on children in malaria-endemic areas followed by iron overload.32
Dietary diversification is also a potent approach that reinforces diet quality by targeting multiple nutrients and emphasizing food groups and food synergy. In rural India, an intervention study was carried out and found that green leafy vegetables consumption more than twice weekly improved the iron content significantly from 44.7% to 60.6%, as did the consumption of seasonal fruits.33 Lack of evidence-based and measurable endpoints, issues of affordability, poor access to prenatal care, lack of public awareness, poor literacy and insufficient counselling made this approach difficult during implementation. 34,35
As per WHO, fortification of iron is referred to the practice of elevating the iron content intentionally in food for improving the nutritional quality for public health.34 Iron fortification technique has gained immense importance in high-income countries for its proven, safe and cost-effective strategy improving human diets and preventing ID and IDA. Mass fortification, open market (commercial) fortification, targeted (high-risk groups) fortification, household fortification, and community fortification methods are five WHO recommended types of iron fortification.36The solubility factor of the iron fortificants play an important role in the bioavailability of iron in humans. Iron often reacts with the food components causing organoleptic changes and leading to the oxidation of fats. Therefore, less soluble compounds which are recognized by the generally recognized as safe (GRAS) are often chosen for the fortification. Reduced iron, ferric phosphate, ferric pyrophosphate, etc., are the compounds that are generally recognized by the GRAS for iron fortification purposes which are closer to the physiological requirement.37 Food staples, condiments, and commercially processed items are the three categories where micronutrients are administrated through food fortification, aimed by improving the nutritional status.38 Iron fortification criteria for wheat and maize flours have now been widely accepted due to its wide consumption by larger populations.39
In recent years, bio fortification of staple crops seeks to be a rural-based potent, feasible and cost-effective strategy to combat ID and IDA.40,41 Iron bio fortification is the process of increasing the iron density of food crops through conventional plant breeding and/or improved agronomic practices/modern biotechnology with no loss in consumer or farmer-preferred characteristics. Bio fortification aims to increase the nutrient content from the plant germination phase rather than during processing of food crops. These cultivars have a positive influence over agro-economical, nutritional and functional health outcomes.42 Agronomic, conventional and transgenic are the common approaches to biofortification.43,44 Ferritin, a protein that is nontoxic and present in plants had been expressed through genetic modifications to combat iron deficiencies.45 For instance, overexpression of the OsIRT1 gene (a divalent metal transporter) in rice increased iron concentration levels by 1.1 folds in rice grains.46 Similarly in cassava tubers, combined overexpression of IRT1 and Fer1 gene increased iron by 5.5 folds.47 The countries where poor staple crop dominate the diets, they are being successfully bio fortified with iron for contending ID and IDA.48,49 Considering the benefits and limitations, bio fortification has many advantages over fortification in many aspects. i.e., cost-effectiveness, sustainability, major impact on remote and rural areas, providing long-term means of delivering micronutrients followed by less toxic effects.
Nutrikinetic Profiling of Iron-enriched Food Varieties: In vitro, Pre-clinical and Clinical Evidences
Nutrition plays a crucial role in the healthy growth, development (physical and cognitive), and socioeconomic status of humans. Though many studies have witnessed the effects of specific bioactive nutrients relative to specific complications, a holistic food-based approach containing essential nutrients remains to be a key strategy to alleviate malnutrition.50
Functional foods such as whole, fortified, bio fortified, enriched, or enhanced foods provide health benefits when consumed at efficacious levels on a regular basis.51 Poor absorption, food-food interactions, and the poor bioavailability of iron upon consumption remain the major failure of functional foods.52 Nutrikinetics is considered to be a new approach that mainly focuses on human nutritional ADME, involving identification, time-course analysis, and parameterization of food compounds in human bio fluids. Nutrikinetic assessment for these functional foods help in overcoming the limitations and also lowers the risk of malnutrition.53 Enhancing the nutrition profile of staple foods through fortification and bio fortification are found to be a promising approach in managing the lacuna of micronutrient deficiencies. In fortification, synthetic forms of iron such as ferrous sulphate, ferrous pyrophosphate, sodium feredetate, ferric sodium ethylene diaminetetra acetate (NaFeEDTA), etc. are supplemented and mixed with staples under controlled supervision in the food industry whereas, in bio fortification, a purposeful increase of these micronutrients through conventional breeding or biotechnological methods are employed. Thus, there may be variation in the release profile of these micronutrients since fortification is a process of physical mixture of iron with staples and bio fortification is a process of enrichment of micronutrients during germination and growth phase of the cultivars. This variation may have an impact that can cause the difference in the release kinetics leading to variation in the bioavailability and bio accessibility of micronutrients. In high-phytate diets, absorption of iron from fortified NaFeEDTA is 2-3 times greater than the absorption from ferrous sulfate.54
To date, many bio accessibility and bioavailability studies are been carried out independently utilizing different fortified and bio fortified foods with different methods viz., solubility/digestibility, cell line studies (Caco2 cell lines and combination of Caco2 along with HepG2 cell models), haemoglobin repletion methods, and in vivo studies (Wistar rats, domestic chicken, rabbits).55,56,57,58
A recent bioavailability study on iron-fortified chickpea was carried out and concluded that iron bioavailability in cooked chickpeas (soup and desi chapatti) was increased (5.8-10.5, 15.3-25.0, and 4.8-9.0 ng ferritin/ mg protein) than the raw products and non-fortified product.59 The bioavailability and bio accessibility of iron bio fortified cowpea study were carried and compared with cooking and raw (germinated) conditions which concluded that the iron absorption was higher in germinated (raw) when compared to cooked conditions through in vitro iron bio accessibility studies.60 Therefore, it is of prime importance to establish a comparative data regarding the bio accessibility and bioavailability of these micronutrients available as fortified foods & bio-fortified cultivars to reach the anticipated target effect.61,62
In vitro Evidences
Due to their significance and broad applicability, in vitro models of human tissues are gaining popularity. A combination of cell culture and in vitro digestive models provides an alternative to human and animal research which is sometimes difficult to undertake due to ethical considerations. Many in-vitro studies have been performed to understand the iron bioavailability from various fortified and bio fortified food varieties such as soybean, rice, wheat, chickpeas, etc. Fumiyuki Goto et al.,63 and colleagues had expressed soybean ferritin in rice seeds through Agrobacterium mediated transformations which leads to an increase by three folds of iron content in the grain which was furtherly conformed with southern blot analysis. Diane M. Della Valle et al.,64 have investigated 23 bio fortified lentil genotypes from different localities for iron concentration, and bioavailability using in vitro cell lines and established a baseline for future improvements in iron bioavailability. In addition, an in-vitro study was carried out on sixty-seven marketed beans and 150 bio fortified varieties in East Africa. The author concluded that the approach of high iron bean bio fortification approach couldn’t meet the malnutrition requirements and many bio fortified varieties remained no different from normal variety.65 Tammanna A Jaan and colleagues59 studied and examined chickpea potentiality by fortifying iron with (FeSO4.7H20) and NaFeEDTA through spraying and drying methods. Under various cooking conditions, cooked split desi seeds (soup), desi chapatti, and Kabuli chapatti were made with iron-fortified chickpea, their respective iron bioavailability was increased by .5.8-10.5, 15.3-25.0, and 4.8-9.0. ng ferritin/mg protein. In another study, a simple in vitro technique was developed to improve iron and zinc content in chickpeas i.e., by soaking chickpeas in fortified water. This method was reported to improve micronutrient mineral content, and higher bio accessibility even under cooking conditions.66 Rateesh and colleagues67 investigated the inhibitory factor variations in 13 bio fortified pearl millets and found that the inhibitors are majorly affecting the bio accessibility of micronutrients. Further, the grains when subjected to soaking or fermentation before consumption might lead to improvement in the bio accessibility of the micronutrients. Selection of food variety for fortification plays a crucial role in reducing malnutrition. For instance, in a study, biscuits which are fortified with iron showed good bioavailability but upon storage, damaged the shelf life and lead to lipid oxidation.68Apart from traditional methods, novel fortification techniques like cold plasma treatment, iron binding peptides, iron nanoparticles, and iron polymeric liposome encapsulation have also been successfully employed to improve bio accessibility in different food varieties.69,70,71,72
Pre-clinical Evidences
Preclinical studies are considered to be an appropriate model for evaluating the bioavailability and bio accessibility of enriched foods using animal models. In a study, Cintia Tamez Sunt Ana et al.,60 demonstrated that pro-vitamin A had no discernible impact on the bioavailability of iron in the bio fortified cowpea and cassava mixture according to in vivo methods, which also revealed a 19.5 percent increase in iron content in the bio fortified variety. Few research studies were performed to assess the toxicity of excessive and prolonged intake of fortified dietary iron in male wister rats. The results had shown significant evidence for toxicity, and oxidative stress which may cause colon-related problems in humans. Studies also proved that excessive storage of iron (Iron overload) would lead to cardiomyopathy and is considered a major factor of morbidity and mortality among humans.73,74
Clinical Evidences
Despite of expensiveness and ethical considerations, human trials are considered to be more accurate and precise for evaluating iron from enriched varieties. Sumitra Muthayya et al.,75 had carried out randomized efficacy trials on iron-deficient school-going children in India with fortified wheat and found that in the treatment group, the prevalence of ID and ID anaemia decreased significantly from 62 to 21 percent and 18 to 9 percent, respectively. They also reported improving results in reducing iron deficiency and body iron stores. Another study was performed to find the role of citric acid in iron-fortified fish sauce on 10 adult women and reported that iron absorption was higher in the presence of citric acid with 14.1% when compared to 12.0% in its absence.76
Pauline and their colleagues77 conducted a randomized study on 516 iron-deficient children by dividing them into three groups. The first group received high dose of NaFeEDTA fortified maize flour (56 mg/kg), the second group received a low dose (28 mg/kg) and the third group received elemental iron (56 mg/kg). According to the study’s findings, consuming high doses of NaFeEDTA helped children’s iron status indicators by lowering ID and IDA.
Randomized efficacy trials have also been carried out in different age groups with bio fortified cultivars like rice, beans, and pearl millets. In these studies, it was evidenced to be a promising approach against iron deficiencies.78,79,80,81 For example, in a study, the authors investigated to what extent the iron is bioavailable in both post-harvest fortified and bio fortified pearl millets and found that post-harvest iron-fortified millet meals (10.4 percent) had higher fractional iron absorption when compared to regular-iron bio fortified millet meals.82 Similar studies on pearl millets was carried out in the same year on young children and found enhancing concentrations of bioavailable iron when consumed as primary staple food.81 Petry et.al.,83 conducted an iron absorption study in cooked composite meals with bio fortified beans which resulted 54 percent higher concentration of iron than in the same meals with control beans. To compare the iron absorption from meals containing bio fortified beans (8.8 mg Fe/100 g) and control beans (5.4 mg Fe/100 g), a crossover design study involving 22 Rwandese women was conducted. This study also demonstrated high levels of Fe absorption. Iron absorption inhibitors such as phytic acid constrained the bioavailability of the iron in bio fortified beans.
Few research studies suggested that a combinational approach i.e., combining iron with vitamin A could potentiate the bioavailability in both fortified and bio fortified food varieties. For instance, an in vivo study described the effect of combinations of bio fortified beans and rice with high carotenoid content. This showed an increase in iron bioavailability, favourably influenced by increased plasma antioxidant capacity and protein genes involved in iron metabolism.84 Similar work was carried out by one of the authors in fortified pearl millet weaning foods bio fortified with iron along with vitamin A and also investigated the role of vitamin A in iron absorption. However, the results obtained were highly promising and maintained iron homeostasis and hepatic iron stores in animals with low levels of iron as well as significantly increased the digestive and metabolic utilisation of iron.85 Laura and their colleagues86 carried out a randomized intervention study on iron bio fortified beans with 150 low iron status women and concluded that consumption of iron-bio fortified beans improved cognitive performance in young adult women.
Table 1: Few Examples on Food Strategies that were Employed for Iron Malnutrition.
| S.No. | Type of food vehicle | Food intervention | Outcome | Study Design | Reference |
| 1. | Beans | Biofortification | The bio fortified beans had improved cognitive performance in young adult women | Clinical | 86 |
| 2. | Chick peas | Fortification | Fe bioavailability > by 5.8–10.5, 15.3–25.0, and 4.8–9.0 ng ferritin/mg protein | In vitro approach | 59 |
| 3. | Wheat Biscuits | Fortification | Food fortification with iron and EDTA – decreased blood lead concentrations.NaFeEDTA should be the iron fortifier of choice. | Clinical | 93 |
| 4. | Wheat | Fortification | Decreased anaemia from 62 to 21 percent and 18 to 9 percent in children | Clinical | 75 |
| 5. | Peral Millets | Fortification & Biofortification | The fractional iron absorption of post-harvest iron-fortified millet meals was higher (10.4 percent) than that of regular and iron-bio fortified millet meals. | Clinical | 82 |
| 6. | Polished Rice | Fortification | The bio fortified rice had more bioavailable iron than the unfortified rice. | In vitro | 94 |
| 7. | Beans | Biofortification | Fe-bio fortified beans had a lower bioavailability than regular beans. | In vivo approach | 95 |
| 8. | Pearl Millet | Fortification | The liver’s iron stores returned to normal levels as iron bioavailability increased. | In vivo approach | 85 |
Limitations of Fortified and Bio fortified Food Interventions
Despite their advantages, still there exist some challenges for fortified and bio fortified food varieties such as iron overload, labour-intensive effort, improper selection of food vehicles, stability issues, and involvement of expensive technologies, etc.48,87 Digestibility, stability, bio accessibility, and bioavailability of the functional foods are highly influenced by cooking procedures, food matrix, and the presence of micronutrient enhancers and inhibitors.88
The nutritional and anti-nutritional factors considerably improve or inhibit iron absorption when ingested in different forms. Phenolic compounds and phytates are some of the anti nutritional compounds present in plant-based foods that hinder iron absorption in humans. Animal proteins such as milk, soybean, and albumin also reduce iron absorption. Black tea and coffee consumption has also been shown to significantly reduce the amount of iron that is absorbed from composite meals, with coffee having about half the inhibitory effect of tea.89 On the other hand, research revealed that vitamin C significantly promotes the absorption and bioavailability of iron and is shown to be more effective at increasing iron status. In vegetarians, the effect of vitamin C, which is itself an antioxidant, acts significantly to counteract the effect of phytic acid.90 Additionally, consumption of meat, fish, and poultry increases the absorption of nonheme iron.24 Moreover, further research focus on this optimal intake, reducing levels of anti nutrients in functional foods could be the smart approach for improving iron absorption and bioavailability.91,92
Conclusion
Overall, the above-mentioned strategies provide us with in-depth knowledge on the application of functional foods for improving iron levels. A significant barrier to food fortification with stable and bioavailable nutrients without compromising organoleptic qualities is the current lack of accessible, low-cost technology. Lastly, fortification failed to bridge the low-income and suburban areas. Similarly, the major drawback in bio fortification is the kinetic correlation between consumption and bioavailability among affected population. Further research should focus on developing comparative nutrikinetic aspects in the same or diverse functional food varieties (fortified vs fortified; bio fortified vs bio fortified; bio fortified vs fortified) which could provide new insights into assessing and evaluating health outcomes, cost-effectiveness, bioavailability, bio accessibility, and toxicity.
Acknowledgement
All the authors would like to thank Indian Council of Medical Research (ICMR). Mr. Kalyan Chekraverthy. We would like to thank ICMR for providing Senior Research Fellow
Conflict of Interest
The authors state that there is no conflict of interest.
Funding Sources
This work is funded by Indian Council of Medical Research (ICMR) – ADHOC project (Letter no. F.N.5/9/1323/2020-Nut), ICMR Senior Research Fellow (Letter no. F.N.3/1/2/188/2020(Nut).
References
- Gozzelino R., Poli M., Arosio P. Iron as Therapeutic Target in Human Diseases. Pharmaceuticals. 2019;12(4):178.
CrossRef - Allen L. Guidelines on Food Fortification with Micronutriens. World Health Organization : Food and Agriculture Organization of the United Nations; 2006.
- Van Der Straeten D., Bhullar N. K., De Steur H., Gruissem W., MacKenzie D., Pfeiffer W., Qaim M., Slamet-Loedin I., Strobbe S., Tohme J., Trijatmiko K. R., Vanderschuren H., Van Montagu M,, Zhang C., Bouis He. Multiplying the efficiency and impact of biofortification through metabolic engineering. Nat Commun. 2020;11(1):5203.
CrossRef - Rathi K., Kamboj P., Bansal P., Toteja G. A review of selected nutrition & health surveys in India. Indian J Med Res. 2018;148(5):596.
CrossRef - Muthayya S., Rah J. H., Sugimoto J. D., Roos F. F., Kraemer K., Black R. E. The Global Hidden Hunger Indices and Maps: An Advocacy Tool for Action. PLoS ONE. 2013;8(6):e67860.
CrossRef - Abu-Ouf N. M., Jan M. M. The impact of maternal deficiency and iron deficiency anemia on child’s health. Saudi Med J. 2015;36(2):146-149.
CrossRef - Griffin I. J., Rogido M. Temporal Trends in Iron Intake, Iron Fortification, and Iron Deficiency. J Nutr. 2021;151(7):1686-1687.
CrossRef - Zimmermann M. B., Hurrell R. F. Nutritional iron deficiency. The Lancet. 2007;370(9586):511-520.
CrossRef - Kumari R. Prevalence of Iron Deficiency and Iron Deficiency Anaemia in Adolescent Girls in a Tertiary Care Hospital. J Clin Diagn Res. Published online 2017.
CrossRef - Rammohan A, Awofeso N, Robitaille MC. Addressing Female Iron-Deficiency Anaemia in India: Is Vegetarianism the Major Obstacle? Siffel C, Alderete E, eds. ISRN Public Health. 2011;2012:765476.
CrossRef - Onyeneho N. G., Ozumba B. C., Subramanian S. V. Determinants of Childhood Anemia in India. Sci Rep. 2019;9(1):16540.
CrossRef - Ahankari A. S., Myles P. R., Fogarty A. W., Dixit J. V., Tata L. J. Prevalence of iron-deficiency anaemia and risk factors in 1010 adolescent girls from rural Maharashtra, India: a cross-sectional survey. Public Health. 2017; 142:159-166.
CrossRef - Mitrache C., Passweg J. R., Libura J., Petrikkos L., Seiler W. O., Gratwohl A., Stähelin H.B., Tichelli A. Anemia: an indicator for malnutrition in the elderly. Ann Hematol. 2001;80(5):295-298.
CrossRef - Cappellini M. D., Musallam K. M., Taher A. T. Iron deficiency anaemia revisited. J Intern Med. 2020;287(2):153-170.
CrossRef - Iron Deficiency Anemia [Internet]. idi. [cited 2020 Apr 14]. Available from: http://www.irondisorders.org/iron-deficiency-anemia
- Sultana T., Jahan I., Sarker M. J. A., Ferdous K., Shamsuddin A. K., Ahmed M. R. Assessment of Knowledge about Iron Deficiency Anemia among the Adult Women in Selected Hospitals of Dhaka City. J Adv Med Med Res. Published online February 22, 2021:78-84.
CrossRef - Muleviciene A., Sestel N., Stankeviciene S., Sniukaite-Adner D., Bartkeviciute R., Rascon J., Jankauskiene A. Assessment of Risk Factors for Iron Deficiency Anemia in Infants and Young Children: A Case–Control Study. Breastfeed Med. 2018;13(7):493-499.
CrossRef - FAO, IFAD, UNICEF, WFP and WHO. The State of Food Security and Nutrition in the World. 2020;
- Institute of Medicine (U.S.), Panel on Micronutrients. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc. National Academy Press; 2002.
- Anderson G. J., Frazer D. M. Current understanding of iron homeostasis. Am J Clin Nutr. 2017;106(Supplement 6):1559S-1566S.
CrossRef - Waldvogel-Abramowski S., Waeber G., Gassner C., Buser A., Frey B. M., Favrat B., and Tissot J. D. Physiology of Iron Metabolism. Transfus Med Hemotherapy. 2014;41(3):213-221.
CrossRef - Siah CW, Ombiga J, Adams LA, Trinder D, Olynyk JK. Normal iron metabolism and the pathophysiology of iron overload disorders. Clin Biochem Rev. 2006; 27(1):5-16.
- Ratcliffe L. E. K., Thomas W., Glen J., Padhi S., Pordes B. A., Wonderling D., Connell R., Stephens S., Mikhail A. I., Fogarty D. G., Cooper J. K., Dring B., Devonald M. A., Brown C., Thomas M. E Diagnosis and Management of Iron Deficiency in CKD: A Summary of the NICE Guideline Recommendations and Their Rationale. Am J Kidney Dis. 2016; 67(4):548-58.
CrossRef - Hurrell R., Egli I. Iron bioavailability and dietary reference values. Am J Clin Nutr. 2010; 91(5):1461S-1467S.
CrossRef - Theil E. C. Iron Homeostasis and Nutritional Iron Deficiency. J Nutr. 2011;141(4):724S-728S.
CrossRef - Hooda J., Shah A., Zhang L. Heme, an Essential Nutrient from Dietary Proteins, Critically Impacts Diverse Physiological and Pathological Processes. Nutrients. 2014; 6(3):1080-1102.
CrossRef - WHO Micronutrient deficiencies Available from: www.who.int/nutrition/topics/ida/en/ html. 2020.
- Bhutta Z. A., Das J. K., Rizvi A., Gaffey M. F., Walker N., Horton S., Webb P., Lartey A., Black R. E Evidence-based interventions for improvement of maternal and child nutrition: what can be done and at what cost? Lancet Lond Engl. 2013; 382(9890):452-477.
CrossRef - Fernández-Gaxiola A. C., De-Regil L. M. Intermittent iron supplementation for reducing anaemia and its associated impairments in adolescent and adult menstruating women. Cochrane Developmental, Psychosocial and Learning Problems Group, ed. Cochrane Database Syst Rev. 2019;31;1:CD009218 Published online January 31, 2019.
CrossRef - Tolkien Z., Stecher L., Mander A. P., Pereira D. I. A., Powell J. J. Ferrous Sulfate Supplementation Causes Significant Gastrointestinal Side-Effects in Adults: A Systematic Review and Meta-Analysis. Strnad P, ed. PLOS PLoS ONE. 2015;10(2): e0117383.
CrossRef - Bloor S. R., Schutte R., Hobson A. R. Oral Iron Supplementation—Gastrointestinal Side Effects and the Impact on the Gut Microbiota. Microbiol Res. 2021;12(2):491-502.
CrossRef - Pasricha S. R., Drakesmith H., Black J., Hipgrave D., Biggs B. A. Control of iron deficiency anemia in low- and middle-income countries. Blood. 2013;121(14):2607-2617.
CrossRef - Rao S., Joshi S., Bhide P., Puranik B., Asawari K. Dietary diversification for prevention of anaemia among women of childbearing age from rural India. Public Health Nutr. 2014;17(4):939-947.
CrossRef - Allen L. Guidelines on Food Fortification with Micronutriens. World Health Organization : Food and Agriculture Organization of the United Nations; 2006.
- Nair M. K., Augustine L. F., Konapur A. Food-Based Interventions to Modify Diet Quality and Diversity to Address Multiple Micronutrient Deficiency. Front Public Health. 2016;3.
CrossRef - Liyanage C., Hettiarachchi M. Food fortification. Ceylon Med J. 2011;56(3):124.
CrossRef - Nutrition C for FS and A. Generally Recognized as Safe (GRAS). FDA.
- Das J. K., Salam R. A., Kumar R., Bhutta Z. A. Micronutrient fortification of food and its impact on woman and child health: a systematic review. Syst Rev. 2013;2(1):67.
CrossRef - World Health Organization. Meeting Report: WHO Technical Consultation: Nutrition-Related Health Products and the World Health Organization Model List of Essential Medicines – Practical Considerations and Feasibility: Geneva, Switzerland, 2021 September 2018. World Health Organization; 2019.
- Bouis H. E., Hotz C., McClafferty B., Meenakshi J. V., Pfeiffer W. H. Biofortification: A New Tool to Reduce Micronutrient Malnutrition. 2011 Mar;32(1 Suppl): S31-40.
CrossRef - Osendarp S. J. M., Martinez H., Garrett G. S., . Large-Scale Food Fortification and Biofortification in Low- and Middle-Income Countries: A Review of Programs, Trends, Challenges, and Evidence Gaps. Food Nutr Bull. 2018;39(2):315-331.
CrossRef - WHO. Biofortification of staple crops. www.who.int/health-topics/food-fortification/ html.
- Saltzman A., Andersson M. S., Asare-Marfo D. Biofortification Techniques to Improve Food Security. In: Reference Module in Food Science. Elsevier; 2016: B978008100596503078X.
CrossRef - Hotz C. Biofortification. In: Encyclopedia of Human Nutrition. Elsevier; 2013:175-181.
CrossRef - Kumar S., Palve A., Joshi C., Srivastava R. K., Rukhsar. Crop biofortification for iron (Fe), zinc (Zn) and vitamin A with transgenic approaches. Heliyon. 2019;5(6):e01914.
CrossRef - Lee S., An G. Over-expression of OsIRT1 leads to increased iron and zinc accumulations in rice. Plant Cell Environ. 2009;32(4):408-416.
CrossRef - Okwuonu I. C., Narayanan N. N., Egesi C. N., Taylor N. J. Opportunities and challenges for biofortification of cassava to address iron and zinc deficiency in Nigeria. Glob Food Secur. 2021; 28:100478.
CrossRef - La Frano M. R., de Moura F. F., Boy E., Lönnerdal B., Burri B. J. Bioavailability of iron, zinc, and provitamin A carotenoids in biofortified staple crops. Nutr Rev. 2014;72(5):289-307.
CrossRef - Khush G. S., Lee S., Cho J. I., Jeon J. S. Biofortification of crops for reducing malnutrition. Plant Biotechnol Rep. 2012;6(3):195-202.
CrossRef - Forouhi N. G., Unwin N. Global diet and health: old questions, fresh evidence, and new horizons. The Lancet. 2019;393(10184):1916-1918.
CrossRef - Hasler C. M. Functional Foods: Benefits, Concerns and Challenges—A Position Paper from the American Council on Science and Health. J Nutr. 2002;132(12):3772-3781.
CrossRef - De Vos W. M., Castenmiller J. J., Hamer R. J., Brummer R. J. M. Nutridynamics – studying the dynamics of food components in products and in the consumer. Curr Opin Biotechnol. 2006;17(2):217-225.
CrossRef - Van Duynhoven J. P. M., van Velzen E. J. J., Westerhuis J. A., Foltz M., Jacobs D. M., Smilde A. K. Nutrikinetics: Concept, technologies, applications, perspectives. Trends Food Sci Technol. 2012;26(1):4-13.
CrossRef - Uauy R., Hertrampf E., Reddy M. Iron Fortification of Foods: Overcoming Technical and Practical Barriers. J Nutr. 2002;132(4):849S-852S.
CrossRef - Tako E., Rutzke M. A., Glahn R. P. Using the domestic chicken (Gallus gallus) as an in vivo model for iron bioavailability. Poult Sci. 2010;89(3):514-521.
CrossRef - Kloots W, Op den Kamp D, Abrahamse L. In vitro iron availability from iron-fortified whole-grain wheat flour. J Agric Food Chem. 2004 Dec 29;52(26):8132-6.
CrossRef - Scheers N. M., Almgren A. B., Sandberg A. S. Proposing a Caco-2/HepG2 cell model for in vitro iron absorption studies. J Nutr Biochem. 2014;25(7):710-715.
CrossRef - Wawer A. A., Sharp P. A., Perez-Moral N., Fairweather-Tait S. J. Evidence for an Enhancing Effect of Alginate on Iron Availability in Caco-2 Cells. J Agric Food Chem. 2012;60(45):11318-11322.
CrossRef - Jahan T. A., Vandenberg A., Glahn R. P., Tyler R. T., Reaney M. J. T., Tar’an B. Iron Fortification and Bioavailability of Chickpea (Cicer arietinum L.) Seeds and Flour. Nutrients. 2019;11(9):2240.
CrossRef - Sant’ Ana C. T., Antunes P. T., Reis T. C. Ddos., Váz‐Tostes M. D.das G., Meira E. F., Costa N. M. B. Bioaccessibility and bioavailability of iron in biofortified germinated cowpea. J Sci Food Agric. 2019;99(14):6287-6295.
CrossRef - Bouis H. E., Welch R. M. Biofortification-A Sustainable Agricultural Strategy for Reducing Micronutrient Malnutrition in the Global South. Crop Sci. 2010;50:S-20-S-32.
CrossRef - Blanco-Rojo R., Vaquero M. P. Iron bioavailability from food fortification to precision nutrition. A review. Innov Food Sci Emerg Technol. 2019; 51:126-138.
CrossRef - Goto F., Yoshihara T., Shigemoto N., Toki S., Takaiwa F. Iron Fortification of Rice Seed by Soybean Ferritin Gene. Nat Biotechnol. 1999;17:282-286.
CrossRef - DellaValle D. M., Thavarajah D., Thavarajah P., Vandenberg A., Glahn R. P. Lentil (Lens culinaris L.) as a candidate crop for iron biofortification: Is there genetic potential for iron bioavailability? Field Crops Res. 2013; 144:119-125.
CrossRef - Glahn R. P., Wiesinger J. A., Lung’aho M. G. Iron Concentrations in Biofortified Beans and Nonbiofortified Marketplace Varieties in East Africa Are Similar. J Nutr. 2020;150(11):3013-3023.
CrossRef - Oghbaei M., Prakash J. Effect of dehulling and cooking on nutritional quality of chickpea (Cicer arietinum L.) germinated in mineral fortified soak water. J Food Compos Anal. 2020; 94:103619.
CrossRef - Krishnan R., Meera M. S. Assessment of inhibitory factors on bioaccessibility of iron and zinc in pearl millet (Pennisetum glaucum (L.) R. Br.) cultivars. J Food Sci Technol. 2017;54(13):4378-4386.
CrossRef - Rebellato A. P., Pacheco B. C., Prado J. P., Lima Pallone J. A. Iron in fortified biscuits: A simple method for its quantification, bioaccessibility study and physicochemical quality. Food Res Int. 2015; 77:385-391.
CrossRef - Akasapu K. An innovative approach for iron fortification of rice using cold plasma. Food Res Int. 2020; 136:109599.
CrossRef - Cheng J., Kenaan A., Zhao D., Qi D., Song J. Photo-polymerizable ferrous sulfate liposomes as vehicles for iron fortification of food. Nanomedicine Nanotechnol Biol Med. 2020; 30:102286.
CrossRef - De Oliveira C.L., Brychkova G., Esteves-Ferreira A.A., McKeown P., de Souza Gomes M., Maluf W.R., Gomes L. A. A., Spillane C. Thermal disruption of the food matrix of biofortified lettuce varieties modifies absorption of carotenoids by Caco-2 cells. Food Chem. 2020; 308:125443.
CrossRef - Mirlohi S. In Vitro Evaluation of Iron-Induced Salivary Lipid Oxidation Associated with Exposure to Iron Nanoparticles: Application Possibilities and Limitations for Food and Exposure Sciences. Int J Environ Res Public Health. 2020;17(10):3622.
CrossRef - Lekawanvijit S., Chattipakorn N. Iron overload thalassemic cardiomyopathy: Iron status assessment and mechanisms of mechanical and electrical disturbance due to iron toxicity. Can J Cardiol. 2009;25(4):213-218.
CrossRef - Lund E. K., Fairweather-Tait S. J., Wharf S. G., Johnson I. T. Chronic Exposure to High Levels of Dietary Iron Fortification Increases Lipid Peroxidation in the Mucosa of the Rat Large Intestine. J Nutr. 2001;131(11):2928-2931.
CrossRef - Muthayya S., Thankachan P., Hirve S., Amalrajan V., Thomas T., Lubree H., Agarwal D., Srinivasan K., Hurrell R. F., Yajnik C. S, Kurpad A. V.. Iron Fortification of Whole Wheat Flour Reduces Iron Deficiency and Iron Deficiency Anemia and Increases Body Iron Stores in Indian School-Aged Children. J Nutr. 2012;142(11):1997-2003.
CrossRef - Walczyk T., Tuntipopipat S., Zeder C., Sirichakwal P., Wasantwisut E., Hurrell R. F. Iron absorption by human subjects from different iron fortification compounds added to Thai fish sauce. Eur J Clin Nutr. 2005;59(5):668-674.
CrossRef - Andang’o P. E., Osendarp S. J., Ayah R., West C. E., Mwaniki D. L., De Wolf C. A., Kraaijenhagen R., Kok F. J., Verhoef H. Efficacy of iron-fortified whole maize flour on iron status of schoolchildren in Kenya: a randomised controlled trial. The Lancet. 2007;369(9575):1799-1806.
CrossRef - Haas J. D., Beard J. L., Murray-Kolb L. E., del Mundo A. M., Felix A., Gregorio G. B. Iron-Biofortified Rice Improves the Iron Stores of Nonanemic Filipino Women. J Nutr. 2005;135(12):2823-2830.
CrossRef - Vaz-Tostes M. d., Verediano T. A., de Mejia E. G., Brunoro Costa N. M.Vaz-Tostes M das G, Verediano TA, de Mejia EG, Brunoro Costa NM. Evaluation of iron and zinc bioavailability of beans targeted for biofortification using in vitro and in vivo models and their effect on the nutritional status of preschool children: Iron and zinc bioavailability of beans targeted for biofortification. J Sci Food Agric. 2016;96(4):1326-1332.
CrossRef - Nambiar V. S., Desai R., Dhaduk J. J. Iron status of women of reproductive age living in pearl millet consuming areas of Banaskantha, Gujarat. 2015;27:8.
- Kodkany B. S., Bellad R. M., Mahantshetti N. S., Westcott J. E., Krebs N, F., Kemp J. F., Hambidge K. M. Biofortification of pearl millet with iron and zinc in a randomized controlled trial increases absorption of these minerals above physiologic requirements in young children. J Nutr. 2013;143(9):1489-1493.
CrossRef - Cercamondi C. I., Egli I. M., Mitchikpe E., Tossou F., Zeder C., Hounhouigan J. D., Hurrell R. F.. Total Iron Absorption by Young Women from Iron-Biofortified Pearl Millet Composite Meals Is Double That from Regular Millet Meals but Less Than That from Post-Harvest Iron-Fortified Millet Meals. J Nutr. 2013;143(9):1376-1382.
CrossRef - Petry N., Egli I., Gahutu J. B., Tugirimana P. L., Boy E., Hurrell R. Phytic Acid Concentration Influences Iron Bioavailability from Biofortified Beans in Rwandese Women with Low Iron Status. J Nutr. 2014;144(11):1681-1687.
CrossRef - Dias D. M., De Castro Moreira M. E., Gomes M. J. C., Lopes Toledo R. C., Nutti M. R., Pinheiro Sant’Ana H. M., Martino H. S. D.Dias D, de Castro Moreira M, Gomes M, . Rice and Bean Targets for Biofortification Combined with High Carotenoid Content Crops Regulate Transcriptional Mechanisms Increasing Iron Bioavailability. Nutrients. 2015;7(11):9683-9696.
CrossRef - Sihag M. K., Sharma V., Goyal A., Arora S., Kapila R. In vivo assessment of iron bioavailability from fortified pearl millet based weaning food: Iron bioavailability from millet based weaning food. J Sci Food Agric. 2016;96(13):4410-4415.
CrossRef - Murray-Kolb L. E., Wenger M. J., Scott S. P., Rhoten S. E., Lung’aho M. G., Haas J. D. Consumption of Iron-Biofortified Beans Positively Affects Cognitive Performance in 18- to 27-Year-Old Rwandan Female College Students in an 18-Week Randomized Controlled Efficacy Trial. J Nutr. 2017;147(11):2109-2117.
CrossRef - Detzel P., Wieser S. Food Fortification for Addressing Iron Deficiency in Filipino Children: Benefits and Cost-Effectiveness. Ann Nutr Metab. 2015;66(Suppl. 2):35-42.
CrossRef - Motilva M. J., Serra A., Rubió L. Nutrikinetic studies of food bioactive compounds: from in vitro to in vivo approaches. Int J Food Sci Nutr. 2015;66(sup1):S41-S52.
CrossRef - Dasa F., AberaF D, T A. Factors Affecting Iron Absorption and Mitigation Mechanisms: A review. Int J Agric Sci Food Technol. Published online December 24, 2018:024-030.
CrossRef - Siegenberg D., Baynes R. D., Bothwell T. H., Macfarlane B. J., Lamparelli R. D., Car N. G., MacPhail P., Schmidt U., Tal A., Mayet F.. Ascorbic acid prevents the dose-dependent inhibitory effects of polyphenols and phytates on nonheme-iron absorption. Am J Clin Nutr. 1991;53(2):537-541.
CrossRef - Shubham K., Anukiruthika T., Dutta S., Kashyap A. V., Moses J. A., Anandharamakrishnan C. Iron deficiency anemia: A comprehensive review on iron absorption, bioavailability and emerging food fortification approaches. Trends Food Sci Technol. 2020;99:58-75.
CrossRef - La Frano M. R., de Moura F. F., Boy E., Lönnerdal B., Burri B. J. Bioavailability of iron, zinc, and provitamin A carotenoids in biofortified staple crops. Nutr Rev. 2014;72(5):289-307.
CrossRef - Bouhouch RR, El-Fadeli S, Andersson M, et al. Effects of wheat-flour biscuits fortified with iron and EDTA, alone and in combination, on blood lead concentration, iron status, and cognition in children: a double-blind randomized controlled trial. The American Journal of Clinical Nutrition. 2016;104(5):1318-1326.
CrossRef - Trijatmiko KR, Dueñas C, Tsakirpaloglou N, et al. Biofortified indica rice attains iron and zinc nutrition dietary targets in the field. Sci Rep. 2016;6(1):19792.
CrossRef - Tako E, Beebe SE, Reed S, Hart JJ, Glahn RP. Polyphenolic compounds appear to limit the nutritional benefit of biofortified higher iron black bean (Phaseolus vulgarisL.). Nutr J. 2014;13(1):28.
CrossRef

This work is licensed under a Creative Commons Attribution 4.0 International License.








