
Introduction
Over the past five decades, a dramatic transition has occurred in global diet and activity levels. During the 1970s, the consumption of processed foods, the emergence of fast-food restaurants, and the global availability and use of cheap edible oils and sweetened drinks began to change the dietary habits of many population groups1. Increased consumption of energy-rich, nutrient-poor foods, reduction in physical activity, and increase in sedentary lifestyles has been associated with increased health problems related to obesity2. This has resulted in a significant global overweight and obesity burden, initially evident in high-income countries but more recently in low- and middle-income countries3. Global overweight and obesity levels have accelerated further due to economic and income growth, urbanisation, and globalisation4-6.
Eating a balanced and varied diet during adolescence is crucial for growth, developmental health, wellbeing and the prevention of obesity, with poor nutrition and lack of physical activity among adolescents contributing to the burden of preventable diseases and premature deaths in adulthood7,8. Further, the Commission on Ending Childhood Obesity stated that a healthy adolescent diet comprises limited or restricted high-calorie foods, fats, free sugars or salt, and plentiful fruit, vegetables, and dietary fibre (e.g., whole grains)9. One study has shown that ‘junk food’ accounts for 20% of variance in weight gain among youth10. Globally (i.e., more than 80 countries were sampled proportionally for each region except for Africa), school-going adolescents, on average, consume low number of servings per day of fruit (1.43 serves; 95% confidence interval 1.26–1.60) and vegetables (1.75 serves; confidence interval 1.58–1.92). In contrast, on average adolescents consumed sugary carbonated soft drinks about once a day11. However, this varied significantly between countries. Fruit consumption was particularly low in South and East Asia, and consumption of carbonated soft drinks was higher in Latin America.
Studies have indicated that children and adolescents in Arabic speaking countries, including the Kingdom of Saudi Arabia (KSA), experience inconsistent nutritional problems, with malnutrition and overnutrition simultaneously common12. One study in KSA reported that more than 50% of 14 to 18 year-old adolescents weigh above the 85th percentile13. This has been attributed to unhealthy dietary and lifestyle habits such as insufficient intake of vegetables and fruit as well as high consumption of sugary food (e.g. sweets, cakes, biscuits, chocolate, and some fizzy drinks and juice drinks) and ‘fast food (mass produced high energy food which tends to lack nutrients and is low in fibre and micronutrients and highly processed grains, high sodium, and sugar which is prepared with the sole purpose of serving quickly)’14,15.
Nutrition promotors have recognised that a wide variety of factors influence adolescents’ dietary behaviour such as adequate knowledge, recognition of healthy foods, their peers and environmental influences16. Nutrition knowledge and understanding the consequences of unhealthy eating play a vital role in predicting an individual’s dietary decisions17. Nutrition knowledge is essential for any individual to attain a healthy lifestyle and for the prevention of diet-related morbidities18,19. Studies have also demonstrated the significance of nutritional attitude in determining diet quality and promoting good nutritional practices, confirming the importance of accurate assessment of attitudes towards nutrition20,21. Adequate knowledge and understanding also lead to self-efficacy and self-control. Adolescents with self-control are more likely to develop a positive healthier attitude and make conscious health-related behavioural decisions such as healthy eating and drinking and avoiding poor eating habits22. The higher self-efficacy an individual develops as a result of adequate knowledge, the higher their intake of healthy food, resulting in the ability to manage their healthy diet even when under pressure or facing obstacles23. Knowledge and attitudes that predict adolescents daily practices are also influenced by their family members (such as parents), the options available in their neighbourhood, peer status and value and concern for their future health24. Thus, studying the correlation between knowledge, attitude and nutrition-related behaviour is important in this period of adolescent nutritional socialisation as they learn to make more individual decisions8.
The impact of COVID-19 on a diet in Saudi Arabia
As SARS-CoV-2 (COVID-19) cases were first reported in KSA, the government, with the Ministry of Health and public health officials’ advice, mandated a population-wide lockdown to control the spread of the virus25. During the lockdown, people were forced to change some of their lifestyle behaviours26. Physical activity plummeted as gyms, and other recreational facilities were closed27, while food consumption increased as a result of boredom and stress, and people started hoarding food as a result of uncertainty about food security28. The negative impact of the pandemic on poor dietary habits was also evident among children and adolescents in Saudi Arabia, where more than 39% reported difficulty maintaining a healthy lifestyle and balanced diet during the pandemic29.
This paper describes findings from a larger school-based study focusing on obesity prevention. Nutrition knowledge, attitude and behaviour30, among intermediate school adolescents in Saudi Arabia will be described. The association between knowledge, attitudes, behaviours and the COVID related nutritional changes among these adolescents and comparison by gender was also explored.
Study design, Population and Sampling Method
This cross-sectional study collected data from six intermediate schools. The six schools were randomly selected from the 262 intermediate government schools in Jeddah, KSA, and included three girls’ and three boys’ schools. All grade 7 to 9 students (11-15 years-of-age from these schools were invited. A random sample of six intermediate schools was generated from the six districts in Jeddah to enhance representativeness30.
Data collection
Consent for school participation was granted by the principal and individual online consent was obtained from both parents and students. A link to an online information sheet, consent and survey was emailed to potential participants by each school’s principal. The schools emailed 3483 students. Of those students, 815 (23.3%) participants (or their parents) did not provide assent or consent to participate resulting in an initial response rate of 76.6%. Of the surveys received, 1500 were complete, while 1168 (33.5%) were extensively incomplete (more than 50% incomplete items within the survey form). Incomplete questionnaires were excluded during the data cleaning process. The survey was conducted using the Qualtrics platform. The survey consisted of five sections: demographic characteristics, knowledge, attitudes, nutritional behaviours, and COVID-19 related nutritional changes.
Measures
Sociodemographic variables
Age, gender, grade and maternal and paternal level of education were requested. Parental level of education was categorised as primary, intermediate, high school, undergraduate and postgraduate.
Knowledge, Attitude and Behaviour
Questions to measure nutrition knowledge, attitudes and behaviours were adapted from previously validated items used in selected international studies31-33. Nutrition knowledge was assessed using eight questions which were adapted from a validated survey targeting urban South African adolescents33. Questions are described in Table 1 (responses: true, false, don’t know; score 0-8; correct answer = 1 point). Based on the total score, the range and median were identified.
Attitudes towards nutrition were measured using eight items (Likert scale with five responses: “strongly agree” to “strongly disagree”; score range 5-40 with higher scores representing more positive attitudes). Additionally, some items were negatively worded, strongly agreeing with the sentence opposing a healthy diet, and reverse coding was applied31. In order to simplify the analysis of the attitude questions, the responses were dichotomised into “agree” and “disagree” and cross-tabulated by gender (see Table 2)34,35. In this five-level Likert scale, neutral response were dichotomised with the least healthy answer to the question. The median cut-off point was used to categorise into higher vs lower scores24,36.
Nutrition-related behaviours were measured using nine questions adapted from an Australian school student survey32. The types and approximate quantities of food consumed regularly were self-reported. The items investigated the reported daily intake of fruit, vegetables, bread and cereal, fast food, energy-dense snacks, sugary drinks, milk and water consumption32. Nutritional behaviour categorisations were made on the basis of Australian and KSA dietary guidelines which recommend that the minimum servings of vegetables, fruit and cereal/bread are five, two and six per day, respectively37,38. The guidelines also recommend that fast food and sugary intake be limited; thus, “none” or “less than one intake per week” was considered ‘limited’. Two or more servings were regarded as a high weekly intake of unhealthy foods and drinks.
Nutritional Change During COVID-19
Nutritional behaviour changes during COVID-19 lockdowns were measured by asking participants about the changes in their food consumption habits. Response options included a five-level Likert scale ranging from “a lot less” to “a lot more”. The items related to nutritional “changes during COVID-19” were adapted from other surveys, including the Australian New South Wales32 pre-COVID survey questions32,39. The NSW survey was initially used as a cross-sectional population survey of schoolchildren age 5 to 16 years which assessed children’s dietary patterns and eating behaviours, physical activity and measures of fitness to identify factors related to overweight and obesity.
Ethics
Approval was granted from the Curtin University of Human Research Ethics Committee (HR2020-0337). Additionally, permission to collect data from intermediate schools in Jeddah KSA was granted by the KSA Ministry of Education (Ref. No.4181827686).
Statistical Analysis
All measures were characterised using descriptive analysis – frequency and percentage. Nutritional outcomes were grouped by gender, and the association was verified using Pearson’s chi-square “χ2“. Fisher’s exact test was used when the cell count was less than 5%. Correlation between continuous variables such as total scores of nutritional attitudes was identified using Pearson’s correlation coefficient. In order to determine the factors associated with nutritional change during COVID-19 lockdown, logistic regression was employed using the categorisation of nutritional change during COVID-19 restrictions versus no change in univariate and multivariate analyses.
The final model was fitted with all significant variables during univariate analysis: Odds Ratios (OR) and 95% Confidence Intervals (CI) were obtained. The significance level was set at p<0.05. The analysis was conducted on IBM SPSS Statistics 27 statistical software.
Results
A total of 1500 adolescent students from six intermediate schools (three boys’ and three girls’ schools) participated in this survey. The initial response rate was 76.6%, with more than 55% completed surveys. Participants ranged from 11 to 15 years and were in grades seven to nine. Just over half of participants, (54%; n=822/1500), were females, and 30% of participants fathers and 34% of their mothers were university educated.
Nutritional Knowledge by Gender
Approximately 66% (n=939/1389) of participants scored above the median of the total knowledge score (≥5 out of 8). Significantly more girls (69%; n=533/772) scored higher than the median compared to males (32%) (p =0.011). Significantly more females (86%; n= 667/772) than males (78%; n=507/648) were aware that drinking a lot of soft drink can cause weight gain (p<0.001). More female students (95%; n=736/772) correctly identified fruit and vegetables as part of a healthy diet compared to 89% (n=575/648) of male students (p<0.001). Only 42%; n=327/772 of female and 34%;n=222/648 of male students correctly answered that a small amount of dietary fibre was insufficient (p=0.002). Knowledge of healthy fibre and salt consumption was poor for both genders, with less than half (48%;n=290/772 female and 45%;n=370/648 male) of all participants correctly answering these questions but not statistically significant (see Table 1).
Table 1: Frequency of Nutrition related knowledge by Gender (N= 1420).
| Knowledge items | Total n(%) | Male n(%) | Female n(%) | Chi-square p-value |
| Scores with median cut-off | ||||
| 0-4 | 481(33.9) | 242(37.3) | 239(31.9) | 0.011 |
| 5-8 | 939(66.1) | 406(62.7) | 533(69.1) | |
| You should eat a lot of sugar to give you enough energy | ||||
| True | 370(26.1) | 178(27.5) | 192 (24.9) | 0.266 |
| False (correct response) | 1050(73.9) | 470(72.5) | 580 (75.1) | |
| If you are eating a healthy diet, there is no need to be physically active | ||||
| True | 299(21.1) | 137(21.1) | 162(21.0) | |
| False (correct response) | 1121(78.9) | 511(78.9) | 610(79.0) | 0.942 |
| Eating a lot of different kinds of foods is healthier than eating only a few types of foods | ||||
| False | 541(38.1) | 247(38.1) | 294(38.1) | |
| True (correct response) | 879(61.9) | 401(61.9) | 478(61.9) | 0.989 |
| Your body only needs a little bit of salt to be healthy | ||||
| False | 760(53.5) | 358(55.2) | 402(52.1) | 0.232 |
| True (correct response) | 660(46.5) | 290(44.8) | 370(47.9) | |
| Drinking a lot of soft drinks can cause weight gain | ||||
| False | 246(17.3) | 141(21.8) | 105(13.6) | <0.001 |
| True (correct response) | 1174(82.7 | 507(78.2) | 667(86.4) | |
| Fruit and vegetables are part of a healthy diet | ||||
| False | 109(7.7) | 73(11.3) | 36(4.7) | <0.001 |
| True (correct response) | 1311(92.3) | 575(88.7) | 736(95.3) | |
| For a healthy diet, you should eat a small amount of dietary fibre | ||||
| True | 871(61.3) | 426(65.7) | 445(57.6) | 0.002 |
| False (correct response) | 549(38.7) | 222(34.3) | 327(42.4) | |
| You can eat as much meat as you want every day | ||||
| True | 608(42.8) | 293(45.2) | 315(40.8) | 0.094 |
| False (correct response) | 812(57.2) | 355(54.8) | 457(59.2) |
Nutrition-related attitudes by gender
Approximately 51%;n=321/648 of males and 43%;n=329/772 of females agreed that they are too young to worry about consuming a healthy diet (p=0.007) (See Table 2). Females (81%;n=614/772) were more likely than males (75%;n=476/648) to agree that what they eat today may affect their future health (p=0.007). The majority of males (74%;n=469/648) and females (72%;n=541/772) liked the taste of healthy food, but this difference was not statistically significant. Generally, female students showed more positive nutrition-related attitudes when compared to male students, but no differences were statistically significant.
Table 2: Nutrition-related attitude categorised by gender (N=1420)
| Attitude items | Total | Male n(%) | Femalen(%) | Chi-square p-value |
| Scores with median cut-off | ||||
| 8-18 | 587(43.2) | 276(44.8) | 311(41.9) | 0.284 |
| 19-28 | 771(56.8) | 340(55.2) | 431(58.1) | |
| I like the taste of healthy food | ||||
| Agree | 1010(72.7%) | 469(74.1) | 541(71.6) | 0.292 |
| Disagree | 379(27.3%) | 164(25.9 | 215(28.4) | |
| I am too young to be worried about eating a healthy diet | ||||
| Agree | 650(46.8) | 321(50.7) | 329(43.5) | 0.007 |
| Disagree | 739(53.2) | 312(49.3) | 427(56.5) | |
| I understand and know what to eat to have a healthy diet | ||||
| Agree | 1097(79.0%) | 488(77.1) | 609(80.6) | 0.115 |
| Disagree | 292(21%) | 145(22.9) | 147(19.4) | |
| My health in the future may be affected by what I eat today | ||||
| Agree | 1090(78.7%) | 476(75.2) | 614(81.2) | 0.007 |
| Disagree | 299(22.3%) | 157(24.8) | 142(18.8) | |
| I know the number of calories or joules of energy in different foods | ||||
| Agree | 698(50.2%) | 331(52.3) | 367(48.5) | 0.164 |
| Disagree | 691 (49.8) | 302(47.7) | 389(51.5) | |
| There are no healthy food choices at school | ||||
| Agree | 1143(82.3) | 521(82.3) | 622(82.3) | 0.988 |
| Disagree | 246(17.7) | 112(17.7) | 134(17.7) | |
| I believe I eat a balanced healthy diet | ||||
| Agree | 665(47.9) | 310(49.0) | 355(47.0) | 0.454 |
| Disagree | 724(52.1) | 323(51.0) | 401(53.0) | |
| I am worried about being too fat | ||||
| Agree | 875(63.0) | 409(64.6) | 466(61.6) | 0.253 |
| Disagree | 514(37.0) | 224(35.4) | 290(38.4) |
* Total rows vary as a result of missing values
Nutrition-related behaviour
Figure 1 illustrates the proportion of students who reported that they met the recommended number of serves of different foods per day. Notably, 56% ate sufficient fruit per day, and 48% consumed less than one serving per day of fast food and sweetened drinks. However, nearly 10% (n=133) and 6% (n=85) of students reported not consuming vegetables and fruit every day, respectively. The majority of participants (86%; n = 1171) ate at least one fast-food meal during the last week, with 47% consuming two or more fast-food meals. Approximately three-quarters of participants (n=1027) reported consuming sweetened drinks at least once in the previous week, out of which 35.5% drank sweetened beverages at least twice a week. In addition, more than 37% of students reported consuming more than four servings of unhealthy snacks such as chocolate bars, cake or chips during the last week.
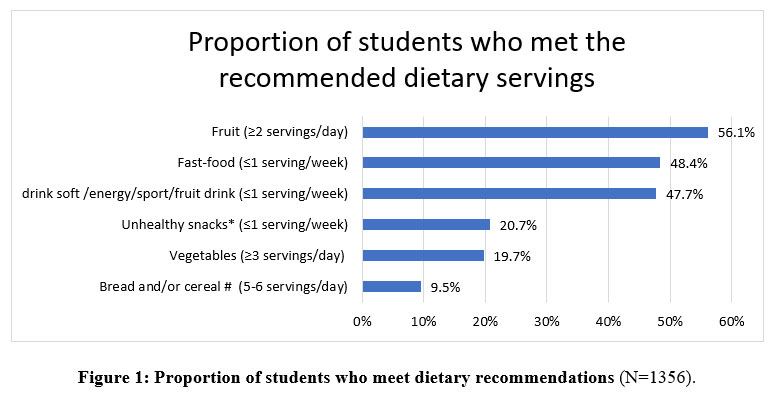 |
Figure 1. Proportion of students who meet dietary recommendations (N=1356). |
Fast-food: McDonald’s, ALBAIK, KFC, pizza, hamburgers, etc.
* For example, a chocolate bar, a piece of cake, a packet of chips /corn chips, ice cream, 3-4 sweet biscuits;
#1 slice of bread, ½ bread roll, ½ cup breakfast cereal, or ½ cup rice, pasta, or noodles
Nutrition-related Behaviour during COVID-19 restrictions by gender
Overall, approximately one-third of participants (27-38% across the four categories) reported little change in eating behaviours during the pandemic. Generally eating behaviours improved with reported decreased consumption of fast foods (54%), unhealthy snacks (42.4%) and sugary drinks (44.3%) with 35.3% reporting increases in fruit and vegetable consumption. About 18.7% of participants reported eating more fast-food meals, whereas more than 50% ate less fast-food meals during the COVID-19 restrictions with this distribution similar between male and female students (See Table 3). Approximately 25% of participants reported consuming more unhealthy snacks while 17.4% of participants reported they drank more sweetened drinks compared to before the pandemic and 44.3% reported they drank less. Additionally, 35% of participants reported eating more healthy foods such as fruits and vegetables, while 38% consumed the same amount, and 27% reported eating “a lot” or “a little less” healthy foods.
Students were also asked if the overall amount of food they ate had increased during the COVID-19 restrictions (See Table 5). While 42% of participants reported no change in the amount of food consumed, approximately 58% reported increased food consumption during COVID-19 restrictions.
Table 3: Changes in nutritional behaviour during COVID-19 restriction (n=38 (2.5%) missing)
| COVID Items | A lot less | A little less | About the same | A little more | A lot more |
| Eat fast food meals | 479(35.6) | 247(18.4) | 368(27.4) | 179(13.3) | 72(5.4) |
| Male | 227(37.3) | 107(17.6) | 163(26.8) | 79(13.0) | 32(5.3) |
| Female | 252(34.2) | 140(19.0) | 205(27.8) | 100(13.6) | 40(5.4) |
| Eat unhealthy snacks* | 267(19.9) | 303(22.5) | 434(32.3) | 229(17.0) | 112(8.3) |
| Male | 148(24.3 | 140(23.0) | 192(31.6) | 93(15.3) | 35(5.8) |
| Female | 119(16.1) | 163(22.1) | 242(32.8) | 136(18.5) | 77(10.4) |
| Drink soft/energy/sport/fruit drinks | 381(28.3) | 215(16.0) | 515(38.3) | 161(12.0) | 73(5.4) |
| Male | 178(29.3) | 95(15.6) | 235(38.7) | 72(11.8) | 28(4.6) |
| Female | 203(27.5) | 120(16.3) | 280(38.0) | 89(12.1) | 45(6.1) |
| Eat healthy food like fruit, vegetables, meat and milk | 170(12.6) | 193(14.3) | 507(37.7) | 311(23.1) | 164(12.2) |
| Male | 103(16.9) | 85(14.0) | 230(37.8) | 136(22.4) | 54(8.9) |
| Female | 67(9.1) | 108(14.7) | 277(37.6) | 175(23.7) | 110(14.9) |
*For example: chocolate bars, cake, a packet of chips /corn chips, ice cream, sweet biscuits
Correlation of continuous KAP scores
The total nutrition knowledge score was negatively, weakly (r=-0.219) and significantly (p<0.001) correlated with the total nutrition attitude score (See Table 4). The nutrition knowledge score was also very weakly associated with the nutrition-related behaviour pre-pandemic (r=0.027, p=0.319) and with nutrition-related behaviour during COVID-19 restrictions (r=0.075, p=0.006). However, nutrition attitude scores were negatively and significantly correlated with behaviours pre-pandemic (r=-0.109, p<0.001) and during COVID-19 restrictions (r=-0.209, p<0.001). Those who reported higher scores of healthy nutrition behaviours (i.e. favouring healthy eating and lower consumption of unhealthy meals, snacks and drinks) were positively related to higher scores of nutrition-related behaviours during COVID-19 restrictions (r= 0.158, p<0.001).
Table 4: Bivariate correlations of knowledge, attitude and behaviour scores.
| 1 | 2 | 3 | |
| 1. Knowledge nutrition score | 1 | ||
| 2. Attitude nutrition score | -0.219 *** | 1 | |
| 3. Behaviour nutrition score | 0.027 | -0.109*** | 1 |
| 4. Behaviour nutrition during COVID-19 score | 0.075** | -0.209*** | 0.158*** |
Impact of COVID-19 on Nutrition
Univariate analysis of the factors associated with the increase in food consumption during COVID-19 lockdown was conducted using binary logistic regression (see Table 5). About 58% (n=777) of participants reported increased food consumption during the COVID-19 restrictions. Higher proportions of older students (15 years) were more likely to report increased food consumption during COVID-19 restrictions when compared to younger students (11 years). Higher nutrition knowledge score (OR= 0.9, 95% CI 0.8-0.96) predicted students to be less likely to report increased food consumption during COVID-19 restrictions, whereas students with higher nutrition attitude scores were more likely to (OR= 1.05, 95% CI 1.02-1.08) increase food consumption during COVID-19 restrictions. Higher servings of unhealthy snacks (OR= 1.13, 95% CI 1.07-1.2), as well as higher servings of fruit (OR= 1.1, 95% CI 1.0-1.14), were associated with increased food consumption. Other factors such as gender, grade, parents’ level of education and servings of vegetables, fast-food and sweetened drinks were not related to the amount of food consumption during COVID-19 restrictions. After adjusting for variables included in Table 5, only higher levels of nutrition knowledge, nutrition attitude and previous high intake of unhealthy snack consumption were associated with a higher risk of increased food consumption during COVID-19 restrictions.
Table 5: Univariate and multivariate analysis of factors associated with nutritional change during COVID-19
| Variables | Increase in food consumption | Unadjusted OR | Adjusted OR | |
| Yesn=777 (57.9%) | Non=564(42.1%) | |||
| Age | ||||
| 11 | 6(20.7) | 23(79.3) | Ref. | 0.90(0.66-1.22) |
| 12 | 102(46.4) | 118(53.6) | 0.3(.1-.8)* | |
| 13 | 190(45.8) | 225(54.2) | 0.3(.1-.8)* | 0.76(0.59-0.98) |
| 14 | 226(38.1) | 367(61.9) | 0.4(.2-1.1) | Ref |
| 15 | 40(47.6) | 44(52.4) | 0.3(.1-.8)* | |
| Gender | ||||
| Male | 248(40.9) | 359(59.1) | Ref. | Ref |
| Female | 316(43.1) | 418(56.9) | 0.9(0.7-1.1) | 0.99(0.79-1.24) |
| Grade | ||||
| 7 | 190(44.2) | 240(55.8) | Ref. | |
| 8 | 228(40.1) | 340(59.9) | 1.2(.9-1.5) | 0.200 |
| 9 | 146(42.6) | 197(57.4) | 1.1(.8-1.4) | 0.652 |
| Maternal level of education | ||||
| < Primary | 102(41.3) | 145(58.7) | 1.0(.6-1.7) | 1.05(.57-1.94) |
| Intermediate | 67(39.4) | 103(60.6) | 1.1(.6-1.9) | 1.15(.62-2.13) |
| High school | 174(43.2) | 229(56.8) | 0.9(.6-1.6) | 1.01(.57-1.77) |
| Undergrad | 192(42.6) | 259(57.4) | 1.0(.6-1.6) | 1.01(.58-1.75) |
| Post-graduate | 29(41.4) | 41(58.6) | Ref. | Ref |
| Paternal level of education | ||||
| < Primary | 79(40.9) | 114(59.1) | 0.9(0.6-1.3) | 0.77(0.46-1.28) |
| Intermediate | 58(41.1) | 83(58.9) | 0.9(0.5-1.4) | 0.80(0.48-1.34) |
| High school | 175(43.3) | 229(56.7) | 0.8(0.5-1.1) | 0.76(0.50-1.17) |
| Undergrad | 197(43.3) | 258(56.7) | 0.8(0.5-1.1) | 0.80(0.53-1.22) |
| Post-graduate | 55(37.2) | 93(62.8) | Ref. | |
| Knowledge* | 4.97(1.57) | 5.24(1.59) | 0.9(0.8-0.96)** | 0.92(0.86-0.99)* |
| Attitude* | 19.7(4.12) | 19.0(3.98) | 1.05(1.02-1.08)** | 1.03(1.01-1.07)* |
| Nutritional change during COVID | ||||
| Bread and/or cereal | 2.83(2.08) | 2.60(2.11) | 1.1 (1-1.1)* | 1.03(.97-1.09) |
| Vegetables | 2.45(1.96) | 2.36(1.85) | 1.0(1.0-1.1) | 0.97(.91-1.04) |
| Unhealthy snacks | 3.80(2.06) | 3.27(2.11) | 1.13(1.07-1.2)*** | 1.13(1.07-1.20)*** |
| Sweetened drinks | 4.06(2.58) | 4.22(2.96) | .98(.94-1.02) | 0.96(0.92-1.01) |
| Fast-food | 3.11(2.33) | 3.15(2.64) | 1.0(1.0-1.1) | 0.97(0.93-1.02) |
| Fruit | 2.57(1.79) | 2.37(1.71) | 1.1 (1.0-1.14)* | 1.05(.98-1.14) |
*Mean (standard deviation)
Discussion
This study aimed to describe the level of nutritional KAB among school-going adolescents and the impact of COVID-19 restrictions on their eating habits in KSA. Intermediate school is potentially the most critical stage of adolescence to develop nutrition-related health behaviours due to the type and magnitude of age-related transitions (puberty) that affect adolescents’ body shape, weight status, and appearance occurring during this time40. During the COVID-19 restrictions, adolescents’ routine behaviours altered, influencing all aspects of life, including food buying behaviour, dietary habits and activity level41. Thus, it is noteworthy to identify KAB levels among this age group during the restrictions.
A good level of nutrition-related knowledge was demonstrated both by female and male students, with 66% of participants scoring above the median of the total knowledge score. Females were more likely to demonstrate higher nutrition-related scores compared to males. Just over half of participants (57%) also reported positive attitudes toward nutrition. Research has suggested that male and female adolescents rank differently on food literacy assessment tools42. International studies reveal that female adolescents are more likely to score higher on food and nutrition assessment tools because they care more about food, nutrition, and health and have more substantial physical appearance concerns than males43,44. Although appearance concerns are more frequently identified among girls, males are not immune to body image concerns during adolescent development as height, and muscular mass is perceived as ideal for manly maturity45. Nutritional knowledge assists adolescents to select healthy food options, to plan meals and provides awareness as to how food intake impacts wellbeing46. However, good nutrition-related knowledge does not always translate to good dietary practice47,48.
Nutritional behaviour before COVID-19 restrictions indicated that more than 50% of students were eating more than one serving of fast food and more than 80% of the students ate unhealthy snacks per week, respectively. This could be due to the decreasing quality of diet during adolescence, which may remain suboptimal until adulthood49. Adolescents’ dietary patterns are often characterised by skipping meals, unhealthy frequent snacking and fast-food consumption without notable concern for their health50. This study confirmed that unhealthy food consumption such as fast food, unhealthy snacks and sweetened drinks was high, and more than 15% of students reported increased consumption during the COVID-19 restrictions. However, 44.3% reported that they drank less sweetened drinks compared to before the pandemic. This could be due to access. For example, before the pandemic, they may have spent more time out with friends – shopping, attending movies and at other recreational activities with high availability of soft drinks, and unhealthy snacks. During the COVID-19 restrictions, participants spent most or all of their time at home, where the availability of. For some, unhealthy food may have been limited.
Similar to a study conducted in the United States of America51, this study found no significant correlation between knowledge and healthy practice. Notably, in this study unhealthy nutrition behaviours were consistent before and during the COVID-19 restrictions with 27% of males and 32% of females reporting similar consumption of fast-food meals and unhealthy snacks before and during COVID-19 restrictions respectively. The US study found prolonged time spent at home could contribute to higher COVID-19 specific stress which may have that caused a higher intake of unhealthy food and snacks. This then led to an increase in food consumption irrespective of the nutritional value during the COVID-19 restriction51.
Interestingly, participants with higher nutritional knowledge and attitude were more likely to increase their food intake during the COVID-19 restrictions. However, the survey question did not ask if this increase was in healthy or unhealthy foods. The students increased their food intake not only for the unhealthy options but also for fruit, vegetables, bread and cereals. These altered consumption behaviours could be due to their closer proximity to their kitchen and perhaps an increased interest in food preparation; increased consumption of relatively healthier food provided by their parents; and reduced purchasing of food from shops and the school canteen. Other international studies have found people to find enjoyment in cooking and eating, to have more time available time to prepare food, and to eat more family meals during COVID-19 restrictions52,53. While these changes have led to increased consumption of healthy food; there is also evidence of increased consumption of indulgence food during pandemic lockdowns54.
There are a number of strengths and limitations that should be considered when interpreting the findings of this study. The study has adequate sample sizes with participants recruited from Jeddah, one of the biggest cities in KSA; however, participants were from only one region in KSA, which may affect the results’ generalizability. However, the findings of this study adds to existing knowledge about nutritional changes during the unprecedented situation of the COVID-19 restrictions. The self-reported, online survey requiring adolescent dietary recall may have led to information bias and may have resulted in over or underestimating the nutritional information provided. Participants tend to respond with socially acceptable responses55 which may have influenced reporting of healthy food consumption. The study’s cross-sectional nature cannot establish the temporality between the amount of food consumption during the COVID-19 restrictions and the KAB of the nutrition among the participants prior to COVID-19 lockdowns. The final limitation is the outcome variable identifying an overall increase in food consumption that did not differentiate between healthy and unhealthy food (so students might be eating more, but it may be more healthy foods). For instance, increased fruit consumption was significantly associated with increased food consumption during the COVID-19 restrictions.
Despite these limitations, the strength of this study was the 77% response rate which is considered an excellent rate for an online survey56. Moreover, this study provides an overview of nutrition knowledge, attitude and behaviours of intermediate school students in Jeddah, KSA, and provides comparisons between male and female students. As schools in KSA are single-gender, gender-specific findings are imperative to inform school-based interventions.
Conclusion
Findings from the present study confirm that many students demonstrated good nutritional knowledge and attitudes. Female participants tended to have significantly higher nutritional knowledge and attitude levels than their male counterparts, even though no significant difference was shown in the amount of food consumption during the pandemic lockdown between both genders. However, unhealthy dietary habits among Saudi adolescents are a paramount public health concern. Their pre-pandemic nutrition-related unhealthy behaviours continued during the COVID-19 restriction period. The findings of this study provide updated and essential data informing school-based interventions aiming to promote healthy lifestyles and the wellbeing of Saudi adolescents. Future research is recommended using qualitative recall dietary diary and a universal tool that measures nutritional behaviours among adolescents and links this to their Body Mass Index (BMI). It is also crucial to develop and tailor interventional programs that prevent unhealthy lifestyles in adolescents in Saudi Arabia.
Acknowledgement
The author would like to thank the General Directorate of Education in Jeddah for their approval and cooperating during data collection.
Conflict of interests
No potential conflict of interest was reported by the authors
Funding Sources
This cross-sectional study did not receive any fund.
References
- Drewnowski A, Popkin BM. The nutrition transition: new trends in the global diet. Nutrition reviews. 1997;55(2):31-43. doi:10.1111/j.1753-4887.1997.tb01593.x
CrossRef - Romieu I, Dossus L, Barquera S, et al. Energy balance and obesity: what are the main drivers? Cancer causes & control. 2017;28(3):247-258. doi:10.1007/s10552-017-0869-z
CrossRef - Jones-Smith JC, Gordon-Larsen P, Siddiqi A, Popkin BM. Is the burden of overweight shifting to the poor across the globe Time trends among women in 39 low- and middle-income countries (1991-2008). INTERNATIONAL JOURNAL OF OBESITY. 2012;36(8):1114-1120. doi:10.1038/ijo.2011.179
CrossRef - Fox A, Feng W, Asal V. What is driving global obesity trends? Globalization or “modernization”? Globalization and health. 2019;15(1):32-32. doi:10.1186/s12992-019-0457-y
CrossRef - Okunogbe A, Nugent R, Spencer G, Ralston J, Wilding J. Economic impacts of overweight and obesity: current and future estimates for eight countries. BMJ Global Health. 2021;6(10):e006351. doi:10.1136/bmjgh-2021-006351
CrossRef - Popkin BM, Adair LS, Ng SW. Global nutrition transition and the pandemic of obesity in developing countries. Nutrition reviews. 2012;70(1):3-21. doi:10.1111/j.1753-4887.2011.00456.x
CrossRef - Patton GC, Sawyer SM, Santelli JS, et al. Our future: a Lancet commission on adolescent health and wellbeing. Lancet. Jun 11 2016;387(10036):2423-78. doi:10.1016/s0140-6736(16)00579-1
CrossRef - Salam RAMS, Hooda MMD, Das JKMDMBA, et al. Interventions to Improve Adolescent Nutrition: A Systematic Review and Meta-Analysis. Journal of adolescent health. 2016;59(4):S29-S39. doi:10.1016/j.jadohealth.2016.06.022
CrossRef - World Health Organization. Report of the commission on ending childhood obesity. World Health Organization; 2016.
- Levitsky DA, Halbmaier CA, Mrdjenovic G. The freshman weight gain: a model for the study of the epidemic of obesity. International Journal of Obesity. 2004;28(11):1435-1442. doi:10.1038/sj.ijo.0802776
CrossRef - Beal T, Morris SS, Tumilowicz A. Global Patterns of Adolescent Fruit, Vegetable, Carbonated Soft Drink, and Fast-Food Consumption: A Meta-Analysis of Global School-Based Student Health Surveys. Food and nutrition bulletin. 2019;40(4):444-459. doi:10.1177/0379572119848287
CrossRef - Musaiger AO, Hassan AS, Obeid O. The paradox of nutrition-related diseases in the Arab countries: The need for action. International journal of environmental research and public health. 2011;8(9):3637-3671. doi:10.3390/ijerph8093637
CrossRef - Al-Dossary SS, Sarkis PE, Hassan A, El Regal ME, Fouda AE. Obesity in saudi children: A dangerous reality. Eastern Mediterranean health journal. 2010;16(9):1003-1008. doi:10.26719/2010.16.9.1003
CrossRef - Al‐Hazzaa H, Al‐Sobayel H, Abahussain N, Qahwaji D, Alahmadi M, Musaiger A. Association of dietary habits with levels of physical activity and screen time among adolescents living in S audi A rabia. Journal of human nutrition and dietetics. 2014;27:204-213.
CrossRef - Almughamisi M, George T, Harding S. Prevalence of overweight and obesity among children and adolescents in Saudi Arabia. Proceedings of the Nutrition Society. 2017;76(OCE4)doi:10.1017/S002966511700369X
CrossRef - Pirouznia M. The association between nutrition knowledge and eating behavior in male and female adolescents in the US. International journal of food sciences and nutrition. 2001;52(2):127-132. doi:10.1080/09637480020027000-8
CrossRef - Black RE, Alderman H, Bhutta ZA, et al. Maternal and child nutrition: building momentum for impact. The Lancet (British edition). 2013;382(9890):372-375. doi:10.1016/S0140-6736(13)60988-5
CrossRef - Al-Almaie S. Knowledge of healthy diets among adolescents in eastern Saudi Arabia. Annals of Saudi medicine. 2005;25(4):294-298. doi:10.5144/0256-4947.2005.294
CrossRef - Al-Jawaldeh A, Taktouk M, Nasreddine L. Food consumption patterns and nutrient intakes of children and adolescents in the eastern mediterranean region: A call for policy action. Nutrients. 2020;12(11):1-28. doi:10.3390/nu12113345
CrossRef - Aggarwal AP, Monsivais PP, Cook AJP, Drewnowski AP. Positive Attitude toward Healthy Eating Predicts Higher Diet Quality at All Cost Levels of Supermarkets. Journal of the Academy of Nutrition and Dietetics. 2014;114(2):266-272. doi:10.1016/j.jand.2013.06.006
CrossRef - Sichert-Hellert W, Beghin L, De Henauw S, et al. Nutritional knowledge in European adolescents: results from the HELENA (Healthy Lifestyle in Europe by Nutrition in Adolescence) study. Public health nutrition. 2011;14(12):2083-2091. doi:10.1017/S1368980011001352
CrossRef - Szabó K, Pikó B. Examination and correlation of nutrition-related attitudes, behavior and information seeking with sociodemographic and psychological variables among adolescents. Orvosi Hetilap OH. 01 Dec. 2018 2018;159(51):2183-2192. doi:10.1556/650.2018.31194
CrossRef - Al-Ghanim L, Alkazemi D. Factors Associated with Self-Efficacy Toward Healthy Eating and Physical Activity among Kuwaiti Adolescent Girls. Current research in nutrition and food science. 2021;9(3):890-903. doi:10.12944/CRNFSJ.9.3.16
CrossRef - Bakhtiar M, Masud-ur-Rahman M, Kamruzzaman M, Sultana N, Rahman SS. Determinants of nutrition knowledge, attitude and practices of adolescent sports trainee: A cross-sectional study in Bangladesh. Heliyon. 2021;7(4):e06637-e06637. doi:10.1016/j.heliyon.2021.e06637
CrossRef - Algaissi AA, Alharbi NK, Hassanain M, Hashem AM. Preparedness and response to COVID-19 in Saudi Arabia: Building on MERS experience. Journal of infection and public health. 2020;13(6):834-838. doi:10.1016/j.jiph.2020.04.016
CrossRef - Alhusseini N, Alqahtani A. COVID-19 pandemic’s impact on eating habits in Saudi Arabia. Journal of Public Health Research. 2020;9(3):354-360. doi:10.4081/jphr.2020.1868
CrossRef - Shahidi SH, Stewart Williams J, Hassani F. Physical activity during COVID‐19 quarantine. Acta Paediatrica. 2020;109(10):2147-2148. doi:10.1111/apa.15420
CrossRef - Galanakis CM. The food systems in the era of the coronavirus (CoVID-19) pandemic crisis. Foods. 2020;9(4):523. doi:10.3390/foods9040523
CrossRef - Alshehri LM, Al Agha AE. Impact of Covid-19 Lockdown on the Unhealthy Dietary Habits and Physical Activity of Children and Adolescents Living in the Kingdom of Saudi Arabia. Annals of Medical and Health Sciences Research. 2021;
- Almutairi NS, Burns S, Portsmouth L. Identifying factors associated with overweight and obesity among intermediate school students aged 12–15 years in school settings: mixed-methodology protocol. BMJ open. 2021;11(5):e045877-e045877. doi:10.1136/bmjopen-2020-045877
CrossRef - Frobisher C, Maxwell SM. The attitudes and nutritional knowledge of a group of 11–12 year olds in Merseyside. International Journal of Health Promotion and Education. 2001;39(4):121-127.
CrossRef - NSW Health. School Students Behaviour Survey:. https://www.health.nsw.gov.au/surveys/student/Documents/student-health-survey-2017-quest.pdf
- Whati L, Senekal M, Steyn N, Nel J, Lombard C, Norris S. Development of a reliable and valid nutritional knowledge questionnaire for urban South African adolescents. Nutrition. 2005;21(1):76-85.
CrossRef - Jeong HJ, Lee W. The level of collapse we are allowed: Comparison of different response scales in Safety Attitudes Questionnaire. Biom Biostat Int J. 2016;4(4):00100.
CrossRef - Khokhar D, Nowson CA, Margerison C, Bolam B, Grimes CA. Knowledge and attitudes are related to selected salt-specific behaviours among australian parents. Nutrients. 2018;10(6):720. doi:10.3390/nu10060720
CrossRef - DeCoster J, Gallucci M, Iselin A-MR. Best Practices for Using Median Splits, Artificial Categorization, and their Continuous Alternatives. Journal of experimental psychopathology. 2011;2(2):197-209. doi:10.5127/jep.008310
CrossRef - Al-Dkheel M. Dietary guidelines for Saudis: The healthy food palm. Riyadh: Ministry of Health General Directorate of Nutrition. Retrieved from …; 2012.
- NHMRC N. Australian dietary guidelines. National Health and Medical Research Council, National Resource Management Ministerial Council. 2013;
- Di Renzo L, Gualtieri P, Pivari F, et al. Eating habits and lifestyle changes during COVID-19 lockdown: an Italian survey. Journal of Translational Medicine. 2020;18(1):1-15.
CrossRef - Lassi Z, Moin A, Bhutta Z. Nutrition in Middle Childhood and Adolescence. Disease Control Priorities, Third Edition (Volume 8): Child and Adolescent Health and Development. 2017:133-146.
CrossRef - Deschasaux-Tanguy M, Druesne-Pecollo N, Esseddik Y, et al. Diet and physical activity during the coronavirus disease 2019 (COVID-19) lockdown (March-May 2020): Results from the French NutriNet-Santé cohort study. The American journal of clinical nutrition. 2021;113(4):924-938. doi:10.1093/ajcn/nqaa336
CrossRef - Mirmiran P, Azadbakht L, Azizi F. Dietary behaviour of Tehranian adolescents does not accord with their nutritional knowledge. Public health nutrition. 2007;10(9):897-901. doi:10.1017/S1368980007246701
CrossRef - Brown R, Seabrook JA, Stranges S, et al. Examining the correlates of adolescent food and nutrition knowledge. Nutrients. 2021;13(6):2044. doi:10.3390/nu13062044
CrossRef - Naeeni MM, Jafari S, Fouladgar M, et al. Nutritional knowledge, practice, and dietary habits among school children and adolescents. International journal of preventive medicine. 2014;5(Suppl 2):S171-S178. doi:10.4103/2008-7802.157687
CrossRef - Voelker DK, Reel JJ, Greenleaf C. Weight status and body image perceptions in adolescents: current perspectives. Adolescent health, medicine and therapeutics. 2015;6(default):149-158. doi:10.2147/AHMT.S68344
CrossRef - Vidgen HA, Gallegos D. Defining food literacy and its components. Appetite. 2014;76:50-59. doi:10.1016/j.appet.2014.01.010
CrossRef - Alaunyte I, Perry JL, Aubrey T. Nutritional knowledge and eating habits of professional rugby league players: Does knowledge translate into practice? Journal of the International Society of Sports Nutrition. 2015;12(1):18-18. doi:10.1186/s12970-015-0082-y
CrossRef - Noronha DC, Santos MIAF, Santos AA, et al. Nutrition Knowledge is Correlated with a Better Dietary Intake in Adolescent Soccer Players: A Cross-Sectional Study. Journal of nutrition and metabolism. 2020;2020:3519781-7. doi:10.1155/2020/3519781
CrossRef - Lipsky LM, Nansel TR, Haynie DL, et al. Diet quality of US adolescents during the transition to adulthood: Changes and predictors. The American journal of clinical nutrition. 2017;105(6):1424-1432. doi:10.3945/ajcn.116.150029
CrossRef - Vaitkeviciute R, Ball LE, Harris N. The relationship between food literacy and dietary intake in adolescents: a systematic review. Public health nutrition. 2015;18(4):649-658. doi:10.1017/S1368980014000962
CrossRef - Jansen E, Thapaliya G, Aghababian A, Sadler J, Smith K, Carnell S. Parental stress, food parenting practices and child snack intake during the COVID-19 pandemic. Appetite. 2021;161:105119-105119. doi:10.1016/j.appet.2021.105119
CrossRef - Eftimov T, Popovski G, Petković M, Seljak BK, Kocev D. COVID-19 pandemic changes the food consumption patterns. Trends in Food Science & Technology. 2020;104:268-272. doi:10.1016/j.tifs.2020.08.017
CrossRef - Ronto R, Nanayakkara J, Worsley A, Rathi N. COVID-19 & culinary behaviours of Australian household food gatekeepers: A qualitative study. Appetite. 2021;167:105598-105598. doi:10.1016/j.appet.2021.105598
CrossRef - Sylvetsky AC, Kaidbey JH, Ferguson K, Visek AJ, Sacheck J. Impacts of the COVID-19 Pandemic on Children’s Sugary Drink Consumption: A Qualitative Study. Brief Research Report. Frontiers in Nutrition. 2022-March-16 2022;9doi:10.3389/fnut.2022.860259
CrossRef - Mann CJ. Observational research methods. Research design II: cohort, cross sectional, and case-control studies. Emergency medicine journal : EMJ. 2003;20(1):54-60. doi:10.1136/emj.20.1.54
CrossRef - Nulty DD. The adequacy of response rates to online and paper surveys: what can be done? Assessment and evaluation in higher education. 2008;33(3):301-314. doi:10.1080/02602930701293231
CrossRef

This work is licensed under a Creative Commons Attribution 4.0 International License.








