Adherence and Barriers to Medical Nutrition Therapy and the Effect on Glycemic Control among Individuals with Type 2 Diabetes in India
 and Arti S Muley1*
and Arti S Muley1* 1Nutrition and Dietetics Program, Symbiosis Institute of Health Sciences, Symbiosis International (Deemed University), Pune, India
2Clinical Nutrition and Dietetics, Indian Institute of Food Science and Technology, Aurangabad, India
Corresponding Author Email: arti@sihspune.org
DOI : http://dx.doi.org/10.12944/CRNFSJ.10.3.18
Download this article as:
![]()
Medical Nutrition Therapy (MNT) has a remarkable effect on glycemic control among individuals with Type 2 Diabetes. However, the extent of adherence to MNT isn't hundred percent. Therefore, we aim to determine the adherence level towards the MNT advised by a Registered Dietitian (RD); to identify the barriers and associated contributing factors and strategies to improve the compliance towards the MNT among people with Type 2 Diabetes. A cross-sectional study was conducted among people with Type 2 Diabetes visiting the out-patient diabetes clinic from Kolhapur city, India. A structured questionnaire was used to capture the adherence and non-adherence, reasons and barriers to adhering the MNT. Out of 293 participants, 41.6% were adhering to the MNT. There was a significant association between the non working group, presence of co-morbidities and diabetes duration. 10 years with the increased adherence level. Similarly, there was a significant reduction of 26.7%, 38.1%, and 30.9% in the fasting, postprandial blood glucose and HbA1c values respectively in adhering group post MNT advice. More than 50% of the participants in the adhering group gave ‘To Improve overall health’ and ‘To control sugar’ as reasons to adhere. ‘Habitual to what they eat’ (64.3%), ‘Does not satisfy hunger’ (42.1%) and ‘Lack of willpower’ (42.1%), were the common barriers identified in our study. Our study shows that the MNT advised by an RD is effective in reducing the socio-cultural barriers to adherence and improves glycemic control. Strategies like making the workplace more diabetes-friendly and adopting behavior changing techniques should be implemented to increase adherence.
KEYWORDS:Dietary Adherence, Dietary Barriers, Glycemic Control, Medical Nutrition Therapy, Type 2 Diabetes Mellitus
Introduction
Diabetes Mellitus (DM) has tripled in number over the past 20 years, and rapidly increasing the health challenges of the 21st century world wide1 . The scenario in India is not different. According to the National Non Communicable Disease Monitoring Survey (NNMS) of India, the prevalence of DM in adults in India is 9.3%², which is very high. Looking at the state wise prevalence, 6 million people from the total population of Maharashtra state are estimated to have Type 2 Diabetes³, which showcases the burden of DM in India.
If uncontrolled, it has serious consequences on the health and well-being. According to ‘Global report on Diabetes by World Health Organization (WHO)4, out of the etiological factors associated with Type 2 Diabetes, diet is the most important contributing and modifiable factor behind the continuous upward rise in prevalence of diabetes worldwide. Diet is also said to be the second most important factor after medication associated with glycemic control in people with Type 2 Diabetes.5 ‘American Diabetes Association (ADA)’ also refers the lifestyle management, with self-management education, medical nutrition therapy (MNT), physical activity, smoking cessation counseling, and psychosocial care, as intrinsic factors in diabetes care.6 Thereby, diet plays a pivotal role in the prevention as well as the management of Diabetes.
Diet given by a Registered Dietician (RD) is also known as Medical Nutrition Therapy (MNT). MNT is a diet that is individualized taking into account the personal and cultural background of the individual and not just generalized dietary recommendations. There are pieces of evidence for the effectiveness of MNT in diabetes care; by boosting the clinical outcome, improving quality of life, reducing diabetes complications, and is cost-effective.7-10 However, MNT being the foundational facet in diabetes care, a substantial proportion of people do not adhere to it and the success of MNT will be determined only when adhered to it. Poor adherence will only diminish the benefits and reduce its effectiveness. This has been proved by a study conducted by Agee et al. 11 in low-income individuals who encounter many barriers towards adherence to MNT. The extent of adherence studies in India varies. A study done in Delhi looked into the adherence to the self care practice like medication (82.4% & ), diet (84.6%), exercise (67.7%) and monitoring blood glucose (17.6%)12. Similarly, another study done in Surat city looked into the factors associated with the non adherence to the diet (24%) and physical activity (54.4%)13. One study done in Tamilnadu looked into the effects of non adherence to medical management (drugs, diet and exercise) on the glycemic control 14. However, not many studies have been done solely on the adherence level and barriers of MNT among people with Type 2 Diabetes in tertiary health facilities in India, and especially in Maharashtra. Therefore, this study aims to find the adherence level towards the MNT recommended by RD, identifying the barriers that affect the level of adherence, and show the favorable outcome of MNT among individuals with diabetes. The findings of this study will help the health care professionals to take appropriate actions for addressing the barriers to MNT which can be an effective addition to the existing diabetes care process, as the success of MNT can be counted on only when there is continued patient adherence.15
Study Methodology
Design and Setting
The study is a cross-sectional study and was conducted in an outpatient department (OPD) of Shri Mahalaxmi DIATONE Institute, from Kolhapur city, Maharashtra, India. It is a specialized center for Diabetes, Thyroid, Obesity, and Nutrition Education (DIATONE).
Study Population
People with Type 2 Diabetes above the age of 20 years, those advised MNT by a RD and those attending the clinic regularly were approached. Individuals having Type 1 Diabetes, who refused to give informed consent, who were recently been hospitalized, and pregnant/lactating women were excluded from the study.
Sample size, Technique and Procedure
The sample size of 300 was decided for the study using the single population proportion formula. Systematic random sampling with a fixed periodic interval was used to select the participants for the study. The interval was calculated based on the average number of individuals visiting the clinic in last one month and the estimated sample size. Accordingly every 5th individual coming to the outpatient department was screened and enrolled in the study, until the required sample size was achieved.
Data Collection
The data was collected by an interviewer with the help of a structured questionnaire. The questionnaire was created from the tools used in similar studies;16,17 it was then modified and validated as per the regional needs. The questionnaire was divided into 6 sections capturing information on socio-demographics, vitals, medical history, exercise routine, biochemical parameters, and adherence and barriers to MNT. The adherence to MNT was checked meal-wise and quantity-wise by 24hour diet recall and compared with the MNT advised given by an RD. People were classified into 2 groups i.e. Group A – “Adhering”- those who followed 3 or more meals; time and quantity-wise and Group B – “Not Adhering” – those who followed 2 or less than 2 meals; time and quantity-wise.
Data Analysis
Analyses were done using SPSS software for Windows (version 25, 2007, IBM Corporation, Armonk, New York, United State). Data presented as percentage or Mean ± SD. Cross tabs were computed for categorical variables when classified according to diet adherence and compared to the chi-square test. The paired sample t-test was used to see the difference in means of the two groups was significant or not. The value of p <0.05 was considered to be statistically significant.
Ethical Consideration
All the ethical standards under the 1964 Helsinki declaration and the institutional research committee were followed. The study was approved by the Independent Ethics Committee of Symbiosis International (Deemed University), Pune, Maharashtra, India. Reference No. SIU/IEC/229. Participants were informed about the purpose of the study, their voluntary involvement, and only after their consent, the data was collected.
Results
Total of 315 participants were approached, from which 310 gave consent and the analysis was done on the data from 293 participants. Participants were classified into Adhering and Not Adhering groups depending on the extent to which they followed the MNT recommended to them. 41.6% of the total participants were adhering to the prescribed MNT while 58.4% of the participants were not adhering.
Socio-demographic Information
The socio-demographic information of the participants shows that, more than half i.e. 51.2% of the participants were male as compared to females 48.8%. Even though not significant, females were more adhering to the MNT than males. The participants were grouped according to age and it was found that the maximum were in between 41-60 years. The mean age of participants in the ‘Adhering’ Group and ‘Not adhering’ Group was 56.3±10.3 and 55.0± 9.8 respectively. Almost 59.1% were living in the urban area with no significant association between the locality and the adherence level. The other factors like marital status, education, and income were not found to be significantly associated with the MNT adherence.
There was a significant association found between the occupation i.e. working and non-working status, duration of diabetes, and co-morbidities present with the MNT adherence as shown in Table 1. with (p<0.05). Non-working participants were 14% more adhering to the MNT as compared to the working participants. Almost 84.4% of the adhering participants had more than 2 co-morbidities present, indicating more adherence to the MNT. Dyslipidemia 65.1% and Hypertension 58.7% were the common co-morbidities among all participants. Participants with the duration of Diabetes of less than 10 years (54.9%), were seen to be more adherent than those having diabetes of more than 10 years. The duration of the MNT last advised was not found to be significantly associated with the MNT adherence level. However, it was observed that 50% of the participants from adhering group had received MNT between 0-3 years. The effect of adhering to the MNT advice given was also found to be significantly associated (p<0.05) with the glycemic control in terms of HbA1c levels. The glycemic control was classified as Good Control with HbA1c level up to 7 % and Poor control if the HbA1c level was above 7 %. Maximum participants 72.1% from the adhering group had their HbA1c levels under good control as compared to the not adhering group participants 58.5%.
Table 1: Socio Demographic Characteristics of the Participants.
| Adhering(n=122) | Not Adhering(n=171) | Total(n=293) | P value | |
| Occupation | ||||
| Working | 23.8 | 37.4 | 31.7 | 0.016* |
| Non Working | 76.2 | 62.6 | 68.3 | |
| Co morbidities | ||||
| No Co Morbidities | 15.6 | 21 | 18.8 | 0.030* |
| ≤ 2 Co Morbidities | 74.6 | 76 | 75.4 | |
| > 2 Co Morbidities | 9.8 | 3 | 5.8 | |
| Duration of Diabetes | ||||
| ≤ 10 years | 54.9 | 66.6 | 61.8 | 0.05* |
| > 10 years | 45.1 | 33.4 | 38.2 | |
| Glycemic Control | ||||
| HbA1c Good Control | 72.1 | 58.5 | 64.2 | 0.019* |
| HbA1c Poor Control | 27.9 | 41.5 | 35.8 | |
Data presented as percentage; * significant at p < 0.05; MNT – Medical Nutrition Therapy
Health Characteristic Information
The Health Parameters like weight, Body Mass Index (BMI), Blood Glucose – Fasting and Postprandial and HbA1c were collected before the MNT advised and at present and compared. There was no significant association (p >0.05) seen in the body weight and BMI before and after the MNT advice. However, a positive significant association (p < 0.05) was seen in the parameters like fasting and postprandial blood glucose and HbA1c levels before and after the MNT advice given as shown in Table 2. There was almost 26.7%, 38.1%, and 30.9% reduction in blood glucose – fasting and postprandial and HbA1c level respectively in the Adhering group. Whereas only 18.3%, 26.7 %, and 20.9 % reduction in blood glucose – fasting and postprandial and HbA1c level respectively in the Not Adhering group.
Table 2: The Health Parameters of the participants Before and After MNT advised.
| Adhering(n=122) | %reduction | Not Adhering(n=171) | %reduction | P value(paired t Test) | |
| Fasting Glucose (gm/dl) | |||||
| Before MNT Advice | 160.7±66.5 | 26.7 | 157.6±60.9 | 18.3 | 0.000* |
| After MNT Advice | 117.8±27.4 | 128.9±39.6 | |||
| Post prandial Glucose (gm/dl) | |||||
| Before MNT Advice | 249.7±94.0 | 38.1 | 246.8±90.7 | 26.7 | 0.000* |
| After MNT Advice | 154.7±42.4 | 181.0±65.7 | |||
| HbA1c (%) | |||||
| Before MNT Advice | 9.4±2.4 | 30.9 | 9.1±2.3 | 20.9 | 0.000* |
| After MNT Advice | 6.5±1.0 | 7.2±1.7 | |||
Data presented as Mean ± SD; * significant at p<0.05; MNT- Medical Nutrition Therapy
Reasons and Barriers for Adhering to MNT
The reasons for adhering to the prescribed MNT were asked to the participants in the Adhering Group. Figure 1.a gives reasons for diet adherence. The most common reason for adhering to the MNT was the improvement of overall health with 55.7%, to control blood sugar levels 53.2% followed by and to reduce complications with 31.9%. A very small percentage of participants 25.4% did adhere to the MNT, as it was recommended by the doctor to follow the diet.
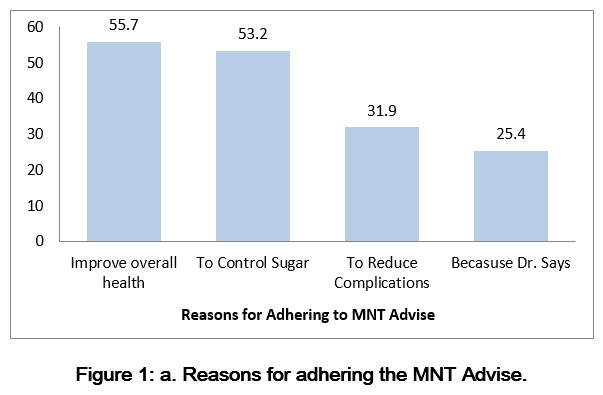 |
Figure 1: a. Reasons for adhering the MNT Advise. |
Data presented as percentage
Similarly, the Barriers for Adhering to MNT were also recorded among the participants in the Not Adhering Group. Figure1.b gives the barriers to adherence. Most participants gave the reason of being habitual to what they eat for the non-adherence, does not satisfy hunger and lack of will power with a frequency of 64.3%, 42.1%, 42.1% respectively. Work related reasons like time restriction at work and limited availability of food at work were also some of the other barriers with 16.3% for MNT adherence.
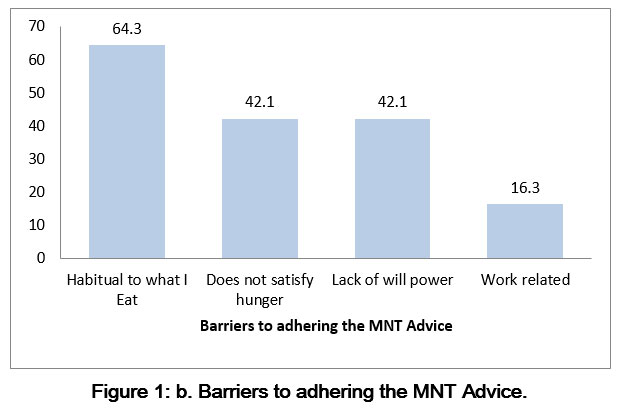 |
Figure 1: b. Barriers to adhering the MNT Advice.Click here to view Figure |
Data presented as percentage
Discussion
Our study aimed to assess the adherence of people with Type 2 Diabetes toward the MNT advised given by an RD. To our knowledge, there is no such study conducted in India so far. There are studies conducted in India on the same line but aiming at the self-care management of Diabetes, including medication adherence, Blood Glucose testing and not specifically MNT.18,12,14 Similarly, studies from other countries like Nepal, Saudi Arabia, and Ghana also studied the adherence of self-care practice among people with Type 2 Diabetes.19-21 Therefore our study is unique and highlights the importance of MNT in diabetes management.
The adherence level of the participants in our study was 41.6% and non-adherence of 58.4%. The percent of adherence to MNT was higher in our study as compared to the findings of other studies, where the adherence level was around 21% in Yemen,16 24.1% in Addis Ababa, Ethiopia,22 25.7% in Northwest Ethiopia,23 and 37.5% in Eastern Ethiopia.17 The reason for the higher adherence to the dietary recommendation in our study may be due to the culturally and personally tailored dietary advice given by the RD, suggesting that the people with Type 2 Diabetes must be referred to an RD for getting the dietary advice. Only one study conducted in Surat city, India13 and one study in other countries like Nepal showed a higher adherence level of 76% and 59%respectfully, but this difference can be a result of the method to assess the adherence level.24
Some studies have recognized the influential factors for dietary adherence, such as the social, cultural and religious background along with education or income level.25,26 However, our study findings showed no significant association of socio-demographic characteristics such as gender, locality, education, income to the adherence level towards the MNT. Again the results are against these study findings because all the dimensions of adherence to the diet like socio-economic, condition-related, therapy-related, and patient-related are been taken into consideration by an RD while planning the MNT for a person. There was a significant association seen between the working status, duration of diabetes, and co-morbidities present. It was seen that people who are not working like housewives, retired persons are more likely to adhere to the MNT given to them as compared to those working. One of the reasons given by the non-adhering participants in our study was work-related. A qualitative study conducted by Ruston et al.27 indicated that workplace environment impacted diabetes self-care management. These findings indicate that workplace environment is likely to hamper or assist in diabetes self-management. Therefore, it is suggested that diabetes-friendly work environment should be created, as Type 2 Diabetes is increasing in the working age group population 40-60 years.1 Similarly, those with the duration of diabetes less than 10 years were found to be more adhering than others. Our findings of the relation with duration of diabetes and adherence were not matching with the study conducted in Ethiopia.17 A systematic review was conducted to study the role of concordant co-morbidities and self-care behavior among people with Type 2 Diabetes. The review concluded that the presence of concordant co-morbidities may improve the self-care 28 and a study conducted in Nepal showed that poor adherence was associated with co-morbidities present.29 Our study findings show a significant association between the co-morbidities and adherence level. Participants having co-morbidities were found to be more adhering to the MNT. The fear of additional health issues apart from Diabetes will lead to serious complications; can be the reason for increased adherence.
Previous review articles done have proven that the diet plays an important role in improving glycemic control and significantly reduce the HbA1c levels.29,30 Our study also shows similar outcomes. It was seen that 72% of the participants in the adhering group were having good glycemic control defined by HbA1c levels up to 7% and showing the significant association of p-value <0.05. It was observed that the HbA1c levels reduced by 30% after MNT advice is given when compared to the HbA1c levels before the MNT advice in the adhering group. Even the blood glucose at fasting and postprandial state showed a significant reduction of 27% and 38 % respectively. These results are similar to the findings of various other studies.16,31,32 Our result findings yet again prove the importance of MNT in diabetes management.
‘Improving overall health’ and ‘To control blood glucose’ were the most common reasons given by the participants for adhering to the MNT advice. Other reasons given were ‘To reduce diabetes complications’ and ‘Because doctors says’. These results indicate that people with Type 2 Diabetes are aware of the consequences of uncontrolled diabetes and that they must be educated about the role of diet and the importance of good glycemic control for the overall management of diabetes from time to time. The results also indicate that doctors should insist the patients to have a proper diet consultation from an RD. There was only one study found to our knowledge looking into the reasons to follow the prescribed diet and had same reasons for the adherence.33 However, many studies are looking into the barriers to adhering to dietary advice.34-38 Our study also looked into the barriers to adhering to the given diet advice and were the same as these studies. It was seen that the most common barriers were – habitual to what they eat, does not satisfy hunger, lack of willpower. This indicates that only nutrition-related education is not enough. Behavioral counseling should also be implemented. Individual’s motivation for change and resistance to altering unhealthy habits must be considered when developing an effective approach to counseling.
Limitations
We have collected good amount of data and the study findings are to the best of our knowledge accurate but there may be chances of social desirability bias. Secondly, the data was collected from only one center of Kolhapur city, Maharashtra, India. Therefore, it cannot be used to make a generalized statement. Lastly, it being a cross sectional study, it is difficult to explore the relation between the outcome and the variables.
Conclusion
The results show the effectiveness of diet advised by an RD to overcome the socio–cultural barriers for adherence to the MNT. The study also indicates the need to make the workplace more diabetes friendly. Lastly, behavioral counseling with time to time reinforcement can be a key to long-term improvement of diabetes outcome, should be a part of the ongoing process of management of diabetes.
Acknowledgment
We thank Dr. Rajesh Deshmane and the entire staff of Shri Mahalaxmi DIATONE Institute, Kolhapur for allowing us to conduct the study in their clinic. No conflict of interest was reported in this study. We also thank Dr. Neha Sanwalkar for assisting in statistical analysis.
Conflict of Interest
The author(s) declares no conflict of interest.
Funding Sources
The author(s) received no financial support for the research, authorship, and or publication of this article.
References
- International Diabetes Federation. IDF Diabetes Atlas. 9th ed. https://www.diabetesatlas.org; 2019. Brussels, Belgium.
- Mathur P., Leburu S. and Kulothungan V. Prevalence, Awareness, Treatment and Control of Diabetes in India From the Countrywide National NCD Monitoring Survey. Front. Public Health. 2022; 10:748157. doi: 10.3389/fpubh.2022.748157
- Community based diabetes prevention in Maharashtra, India, WDF15-1288. World diabetes foundation. (2022, January 6). Retrieved July 6, 2022, from https://www.worlddiabetesfoundation.org/projects/india-wdf15-1288
- 4. World Health Organization. Global report on diabetes. http://www.who.int/diabetes/global-report/en/; 2017; February 23.
- Kakade A. A., Mohanty R.I., Rai S. Assessment of factors associated with poor glycemic control among patients with type II diabetes mellitus. Integr Obesity Diabetes. 2018;4(3):1-6.
- American Diabetes Association. Lifestyle management: Standards of Medical Care in Diabetes-2019. Diabetes Care. 2019 January;5;42 [suppl:1]:S46-S60. DOI: 10.2337/dc19-S005. PubMed: 30559231.
- Briggs E. K., Stanley K. Position of the Academy of Nutrition and Dietetics: therole of medicalnutritiontherapy and registereddietitiannutritionists in the prevention and treatment of prediabetes and Type 2diabetes. J Acad Nutr Diet. 2018 February;118(2):343-353. DOI: 10.1016/j.jand.2017.11.021. PubMed: 29389511.
- Franz M., MacLeod J., Evert A., Brown C., Gradwell E., Handu D., Reppert A. and Robinson M. Academy of Nutrition and Dietetics Nutrition Practice Guideline for Type 1 and Type 2 Diabetes in Adults: Systematic Review of Evidence for Medical Nutrition Therapy Effectiveness and Recommendations for Integration into the Nutrition Care Process. Journal of the Academy of Nutrition and Dietetics. 2017;117(10):1659-1679. DOI: 10.1016/j.jand.2017.03.022. Epub May 19 2017. PubMed: 28533169.
- MacLeod J., Franz M., Handu D., Gradwell E., Brown C., Evert A., Reppert A. and Robinson M. Academy of Nutrition and Dietetics Nutrition Practice Guideline for Type 1 and Type 2 Diabetes in Adults: Nutrition Intervention Evidence Reviews and Recommendations. Journal of the Academy of Nutrition and Dietetics. 2017;117(10):1637-1658. doi: 10.1016/j.jand.2017.03.023.Epub 2017 May 17. PMID: 28527747
- Sami W., Ansari T., Butt N.S., Hamid M.RA. Effect of diet on type 2 diabetes mellitus: a review. Int J Health Sci (Qassim). 2017;11(2):65-71. DOI: 10.1016/j.jand.2017.03.023. Epub May 17 2017. PubMed: 28539866.
- 11. AgeeD., Gates Z., Irwin P.M. Effect of medical nutrition therapy for patients with Type 2 diabetes in a low-/No-Cost clinic: A propensity score–matched cohort study. Diabetes Spectr. 2018;31(1):83-89. DOI: 10.2337/ds16-0077. PubMed: 29456430. PubMed Central: PMC5813315.
- 12. Basu, Garg S., Sharma N., Singh M.M., Garg S. Adherence to self-care practices, glycemic status and influencing factors in diabetes patients in a tertiary care hospital in Delhi. World J Diabetes. 2018;9(5):72-79. DOI: 10.4239/wjd.v9.i5.72. PubMed: 29988911. PubMed Central: PMC6033702.
- 13. JadawalaD., Pawar A.B., Patel P.B., Patel K.G., Patel S.B., Bansal R.K. Factors associated with non adherence to diet and physical activity among diabetes patients: A cross sectional study. Ntl. J Commun Med. 2017; 8(2):68-73.
- 14. S, and R.N. Non-adherence to diabetic treatment and its effect on glycemic control, study at A rural hospital of Tiruchirappalli, Tamil nadu,India. Internet J Health. 2011;13(1).
- 15. Viswanathan V., Krishnan D., Kalra S., Chawla R., Tiwaskar M., Saboo, B., Baruah M., Chowdhury S., Makkar B. and Jaggi S. Insights on Medical Nutrition Therapy for Type 2 Diabetes Mellitus: An Indian Perspective. Advances in Therapy. 2019;36(3):520-547. DOI: 1007/s12325-019-0872-8. Epub February 7 2019. PubMed: 30729455. PubMed Central: PMC6824451.
- 16. Alhariri, Daud F., and Saghir S.A.M. Factors associated with the adherence to diet and exercise among type 2 diabetes patients in Yemen. Diabetes Manag. 2017;7(3):264-271.
- 17. MohammedS., Adem F., Tadiwos Y., Woldekidan N.A., Degu A. Level of adherence to the dietary recommendation and glycemic control among patients with type 2 diabetes mellitus in Eastern Ethiopia: A cross-sectional study. Diabetes Metab Syndr Obes. 2020;13:2605-2612. DOI: 10.2147/DMSO.S256738. PubMed: 32801812. PubMed Central: PMC7384875.
- 18. KarthikC., Radhakrishnan A., Vikram A., Arumugam B., Jagadeesh S. Self-care practices among type II diabetics in rural area of Kancheepuram district, Tamil nadu. J Fam Med Prim Care. 2020;9(6):2912-2918. DOI: 10.4103/jfmpc.jfmpc_356_20. PubMed: 32984148. PubMed Central: PMC7491818.
- 19. Adhikari Baral I., Baral S. Self-care management among patients with type 2 diabetes mellitus in Tanahun, Nepal. Arch Community Med Public Health. 2021; 7(1):037-042. DOI: 17352/2455-5479.000131
- Alhaiti A., Senitan M., Dator W., Sankarapandian C., Baghdadi N., JONES L., Da Costa C. and Lenon G. Adherence of Type 2 Diabetic Patients to Self-Care Activity: Tertiary Care Setting in Saudi Arabia. Journal of Diabetes Research. 2020. Oct 6; 2020:4817637:1-7. DOI: 10.1155/2020/4817637. PubMed: 33083495. PubMed Central: PMC7559229.
- Mogre V., Abanga Z.O., Tzelepis F., Johnson N.A., Paul C. Adherence to and factors associated with self-care behaviours in type 2 diabetes patients in Ghana. BMC Endocr Disord. 2017;17(1):20. DOI: 10.1186/s12902-017-0169-3. PubMed: 28340613. PubMed Central: PMC5366118.
- Bonger Z., Shiferaw S., Tariku E.Z. Adherence to diabetic self-care practices and its associated factors among patients with type 2 diabetes in Addis Ababa, Ethiopia. Patient Preference Adherence. 2018;12:963-970. DOI: 10.2147/PPA.S156043. PubMed: 29922042. PubMed Central: PMC5995298.
- AyeleA., Emiru Y.K., Tiruneh S.A., Ayele B.A., Gebremariam A.D., Tegegn H.G. Level of adherence to dietary recommendations and barriers among type 2 diabetic patients: a cross-sectional study in an Ethiopian hospital. Clin Diabetes Endocrinol. 2018; 4(1):21. DOI: 10.1186/s40842-018-0070-7. PubMed: 30519484. PubMed Central: PMC6267803.
- 24. Ghimire S. Barriers to diet and exercise among Nepalese Type 2 diabetic patients. Int Sch Res Not. 2017;2017:1273084. DOI: 1155/2017/1273084. PubMed: 29349287. PubMed Central: PMC5733940.
- 25. Al-Sahouri, Merrell J., Snelgrove S. Barriers to good glycemic control levels and adherence to diabetes management plan in adults with Type-2 diabetes in Jordan: A literature review. Patient Preference Adherence. 2019;13:675-693. DOI: 10.2147/PPA.S198828. PubMed: 31118591. PubMed Central: PMC6507072.
- 26. Bekele, Asefa A., Getachew B., Belete A.M. Barriers and strategies to lifestyle and dietary pattern interventions for prevention and management of TYPE-2 diabetes in Africa, systematic review. J Diabetes Res. 2020;2020:7948712. DOI: 10.1155/2020/7948712. PubMed: 32766315. PubMed Central: PMC7374199.
- 27. Ruston, Smith A., Fernando B. Diabetes in the workplace—diabetic’s perceptions and experiences of managing their disease at work: a qualitative study. BMC Public Health. 2013 April 25;13:386. DOI: 10.1186/1471-2458-13-386. PubMed: 23617727. PubMed Central: PMC3649948.
- 28. Aga, Dunbar S.B., Kebede T., Gary R.A. The role of concordant and discordant comorbidities on performance of self-care behaviors in adults with type 2 diabetes: a systematic review. Diabetes Metab Syndr Obes. 2019;12:333-356. DOI: 10.2147/DMSO.S186758. PubMed: 31114271. PubMed Central: PMC6497834.
- 29. Mohamed, Staite E., Ismail K., Winkley K. A systematic review of diabetes self‐management education interventions for people with type 2 diabetes mellitus in the Asian western Pacific (AWP) region. Nurs Open. 2019;6(4):1424-1437. DOI: 10.1002/nop2.340. PubMed: 31660170. PubMed Central: PMC6805261.
- Ernawati U., Wihastuti T.A., Utami Y.W. Effectiveness of diabetes self-management education (DSME) in type 2 diabetes mellitus (T2DM) patients: systematic literature review. J Public Health Res. 2021;10(2). DOI: 10.4081/jphr.2021.2240. PubMed: 33855427. PubMed Central: PMC8129774.
- Rusdiana S.M., Savira M., Amelia R. The effect of diabetes self-management education on HbA1c level and fasting blood sugar in type 2 diabetes mellitus patients in primary health care in Binjai city of north Sumatera, Indonesia. Open Access Maced J Med Sci. 2018 April 12;6(4):715-718. DOI: 10.3889/oamjms.2018.169. PubMed: 29731946. PubMed Central: PMC5927509.
- Mottalib A., Salsberg V., Mohd-Yusof B., Mohamed W., Carolan P., Pober D., Mitri J. and Hamdy O. Effects of nutrition therapy on HbA1c and cardiovascular disease risk factors in overweight and obese patients with type 2 diabetes. Nutrition Journal, 2018 April 7;17(1):42. DOI: 1186/s12937-018-0351-0. PubMed: 29626933. PubMed Central: PMC5889846.
- Han C., Chan C., Lim S., Zheng X., Woon Z., Chan Y., Bhaskaran K., Tan K., Mangaikarasu K. and Chong M. Diabetes-related nutrition knowledge and dietary adherence in patients with Type 2 diabetes mellitus: A mixed-methods exploratory study. Proceedings of Singapore Healthcare, 2020;29(2):81-90. DOI: 1177/2010105820901742.
- Cheng L., Leung D., Sit J., Li X., Wu Y., Yang M., Gao C. and Hui R. Factors associated with diet barriers in patients with poorly controlled type 2 diabetes. Patient Preference and Adherence. 2016;10:37-44. DOI: 2147/PPA.S94275. PubMed: 26834464. PubMed Central: PMC4716765.
- Landa-AnellV., Melgarejo-Hernández M.A., García-Ulloa A.C., Del Razo-Olvera F.M., Velázquez-Jurado H.R., Hernández-Jiménez S. Barriers to adherence to a nutritional plan and strategies to overcome them in patients with type 2 diabetes mellitus; results after two years of follow-up. Endocrinol Diabetes Nutr (Engl Ed). 2020;67(1):4-12. DOI: 10.1016/j.endinu.2019.05.007. Epub August 3 2019. PubMed: 31387846.
- AduD., Malabu U.H., Malau-Aduli A.E.O., Malau-Aduli B.S. Enablers and barriers to effective diabetes self-management: A multi-national investigation. PLOS ONE. 2019;14(6):e0217771. DOI: 10.1371/journal.pone.0217771. PubMed: 31166971. PubMed Central: PMC6550406.
- Mostafavi‐Darani, Zamani‐Alavijeh F., Mahaki B., Salahshouri A. Exploring the barriers of adherence to dietary recommendations among patients with type 2 diabetes: A qualitative study in Iran. Nurs Open. 2020;7(6):1735-1745. DOI: 10.1002/nop2.558. PubMed: 33072357. PubMed Central: PMC7544840.
- Hushie M. Exploring the barriers and facilitators of dietary self-care for type 2 diabetes: a qualitative study in Ghana. Health Promot Perspect. 2019 August 6;9(3):223-232. DOI: 15171/hpp.2019.31. PubMed: 31508343. PubMed Central: PMC6717922.
Accepted on: 25 Jul 2022
Second Review by: Prabin Shrestha Nepal
Final Approval by: Dr Shih-Min Hsia





Web of Science Coverage
Emerging Sources Citation Index (ESCI)
2024 Journal Impact Factor: 1.1
Scopus Journal Metrics
CiteScore 2025: 2.6
CiteScore Details
Sustainable Nutrition: Food Systems, Nutrient Retention, and Public Health Impact
![]()
This journal is a member of, and subscribes to the principles of, the Committee on Publication Ethics (COPE)








