The Effectiveness of Aloe-based Drink in Reducing Glycated Albumin and Insulin Resistance of Metabolic Syndrome: A Randomized Clinical Trial
 , Nyoman Suci Widyastiti3, Kusmiyati-Tjahjono4 and Diana Nur Afifah1*
, Nyoman Suci Widyastiti3, Kusmiyati-Tjahjono4 and Diana Nur Afifah1* 1Department of Nutrition Science, Faculty of Medicine, Diponegoro University,
Semarang, Indonesia.
2Department of Internal Medicine, Faculty of Medicine, Diponegoro University,
Semarang, Indonesia.
3Department of Clinical Pathology, Faculty of Medicine, Diponegoro University,
Semarang, Indonesia.
4Department of Biochemistry, Faculty of Medicine, Diponegoro University,
Semarang, Indonesia.
Corresponding Author Email: d.nurafifah.dna@fk.undip.ac.id
DOI : http://dx.doi.org/10.12944/CRNFSJ.10.2.13
Download this article as:
![]()
Insulin resistance (IR) has an important role in the pathology that forms the metabolic syndrome (MetS). Glycated Albumin (GA) has a role as an index of glycemic control associated with MetS. Aloe vera (Aloe barbadensis Miller) is a plant that has anti-diabetic and anti-hypercholesterolemic function. This study aims to investigate the effect of Aloe-based drink on GA and IR in MetS. This study was a true experimental using pre-post randomized control group design. Thirty-eight MetS subjects were divided into two groups: treatment group (n=19) which was provided by 165 g/d of Aloe-based drink for 4 weeks; and the control group (n=19). Both groups were given education regarding of management of MetS. GA was measured by using an ELISA method and IR calculated by HOMA-IR of both groups and statistically analyzed at baseline and the end of treatment. The data were analyzed using paired t-test and independent t-test. At the end of the study, the treatment group showed reduction of GA and HOMA-IR statistically significant (∆GA=-4.3±2.35%; ∆HOMA-IR=-1.6 ±1.87; p=0.001). Compared to control group, the change of GA and HOMA-IR in intervention group were also significantly different. Aloe-based drink was proven to reduce GA and IR in the MetS.
KEYWORDS:Aloe-Based Drink; Glycated Albumin; Insulin Resistance; Metabolic Syndrome
Introduction
Metabolic syndrome (MetS) is a group of risk factors related to cardiovascular disease which consists of visceral obesity, hypertension, high level of fasting blood glucose, and dyslipidemia1–3. World Health Organization (WHO) data showed a high prevalence of obesity (26%), diabetes (9%) and hypertension (22%) in adults in the world which were included in the risk component of MetS4.
Insulin resistance, the main pathogenesis of type 2 diabetes mellitus (DMT2) and directly consequences of hyperglycemia by disrupting the action of insulin, has an important role in the pathology that forms MetS5,6. Homeostasis Model Assessment of Insulin Resistance (HOMA-IR) is one of biomarkers for IR assessment7. Glycated Albumin (GA) has high accuracy of glycemic control over periods and is considered as a good indicator as GA is not influenced by the lifespan of erythrocyte8.
GA is a product of glucose formation which reacts non-enzymatically with reactive amino protein groups to form the Schiff base group. Schiff base then forms Amadori products to form intermediate compounds like α-oxalaldehyde8,9. Further oxidation of the formation of Schiff base and Amadori result in advanced glycation end products (AGE) formation. The formation of AGE is a major contributor to the development of diabetes type 2 which can cause glycosylation process related to free radical formation10–12. Oxidative stress can be considered as a characteristic that unites the components of MetS during aerobic metabolism13,14.
Aloe vera possesses a number of polyphenols, polysaccharides, and amino acids and has biological activities such as anticancer, antioxidant, anti-inflammatory, immunomodulatory, hepatoprotective, antiulcer, antihyperglycemic, antihypercholesterolemic and antidiabetic15–18. The antioxidant contents of Aloe vera are flavonoids, tannins, α-tocopherol (vitamin E), ascorbic acid (vitamin C), and carotenoids18. The previous study stated that extract of Aloe vera has antioxidant activities for phenolic 2.07-40.5 mg Gallic acid equivalent (GAE)/g19. The main polyphenols in Aloe vera are quercetin (94.80 mg/kg), myricetin (1283.50 mg/kg), and kaempeferol (257.7 mg/kg)20.
The study related to the administration of Aloe vera gel in women with MetS aged 46.8±9.7 years stated that Aloe vera concentrated 5:1 (5 L Aloe vera to obtain 1 L of total aloe) in daily ingestion during 4 weeks can reduce blood glucose levels by reducing the pro-inflammatory state and reduction of glucose intolerance21. Another RCT was performed in women with MetS aged ≥20 years administered the Aloe vera gel complex orally (two capsule after breakfast and two after dinner, for 8 weeks) reduced body weight, body fat mass and insulin resistance22. Another study in a double-blind randomized controlled trial investigated the effect of two Aloe vera doses (300 mg and 500 mg, 1 capsule twice a day over an 8-week period) on fasting blood glucose, HbA1C, and lipid profile in prediabetic subjects. They detected a significant decrease in the levels of fasting blood glucose and HbA1C in the treatment group23. Due to the unavailability of the data related to the effect of Aloe-based drink on the levels of GA and HOMA-IR values on MetS subjects, this study aims to investigate the effect of Aloe-based drink on the levels of GA and insulin resistance expressed by HOMA-IR values in MetS.
Materials and Methods
Study design and recruitment of participants
This study was a true experimental using pre-post randomized control group design. The study was conducted in April – June 2018 on employees and members of the Central Java Regional police. Inclusion criteria, subjects were aged 35-56 years who met three or more risk factors for MetS according to NCEP ATP III criteria, not have hyperthyroidism history, hyperthyroidism, nephrotic syndrome, Cushing’s syndrome, glucocorticoid supplementation, liver cirrhosis, pregnancy/ lactation, taking drugs for blood glucose levels or hypertension, smoking ≥ 20 cigarettes / day, and consuming alcohol. Out of 143 employees in total, 47 met the selection criteria, all of whom agreed to participate and provided informed consent. Subjects were randomized into 2 groups: intervention group (n=23) and control group (n=24). There was a loss of 4 subjects in the intervention group and 5 in the control group due they could not be followed up, leaving 19 subjects in each intervention group and control group shown in Figure 1.
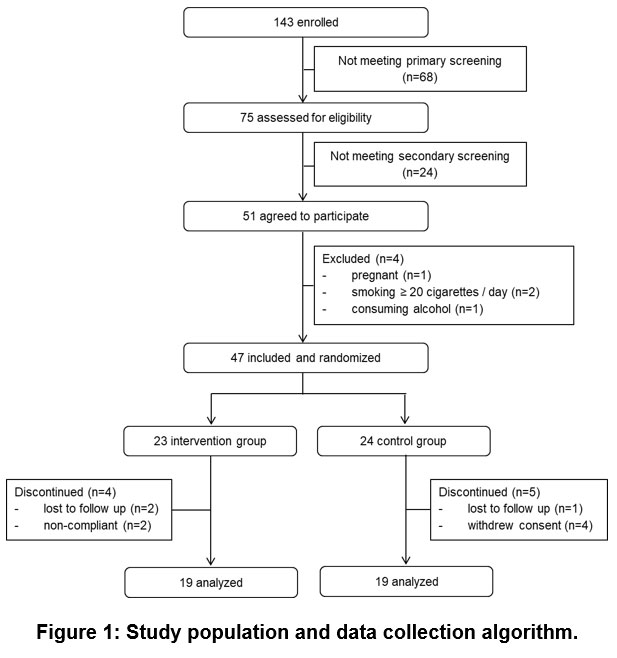 |
Figure 1: Study population and data collection algorithm. |
This experimental design was reviewed and approved by Faculty of Medicine of Diponegoro University-Dr.Kariadi Semarang Hospital research committee proved by ethical clearance certificate number 238/EC/FK-RSDK/IV/2018.
Laboratory, anthropometric and clinical data collection
Baseline data of body weight (assessed by Omron Digital Personal Scale HN289; to nearest 0.1 kg), body height (assessed by GEA Stature Meter SH-2A; to nearest 0.1 cm), blood profiles included fasting blood levels, triglyceride levels, and HDL-C levels (assessed by using enzymatic colorimetric techniques with automatic analyzer Bio Maxima Chemistry BM-100), blood pressure (assessed by Polygreen Automatic Upper Arm Blood Pressure Monitor KP-7550), GA concentration in the plasma sample (analyzed by ELISA method using Elabscience Catalog No: E-EL-H1993, USA kit), and fasting insulin (analyzed by ELISA method using Calbiotech Catalog No. IN374S, USA kit) were collected. The HOMA-IR was calculated using the following formula24:

All the compilation of the intervention period measures were repeated at the end of study. The outcome measures were GA and HOMA-IR. Serum samples were collected by qualified staff from Sarana Medika Laboratory. All subjects fasted overnight for 12 hours before the day of taking blood sample. Furthermore, the blood sample were stored at -250C before examined and analyzed in the same day after all subjects had completed study days. The blood samples were analyzed twice in first day before being given intervention and a day after 4-weeks intervention period for blood glucose, triglyceride levels, and HDL-C levels in Sarana Medika Laboratory, Semarang while serum GA and insulin were analyzed in GAKY Laboratory Diponegoro University, Semarang.
Preparation Aloe-based Drink
Aloe vera were obtained in Kulon Progo farm, Yogyakarta, while the processing of Aloe vera was carried out by the researchers and assisted by Aloe vera cultivators in Yogyakarta. Aloe vera in a similar ripening stage were selected for the Aloe-based drink processing. First, the Aloes were washed and were peeled off to get the Aloe vera leaf extract (a transparent inner gel). Then they were cut into cubes of 1 cm size. The sufficiently 1 tablespoon salt and ½ teaspoon citrate acid were added to the Aloes cubes then were washed after 10 minutes in sequence. The Aloe cubes were blanched for 3-5 minutes in warm water (60-700C) which had been added by with two pieces of Pandan leaves for aroma. A portion of Aloe cubes (165 g) were added to 30 mL low calorie liquid syrup solution.
Study design
The intervention group were provided with 165 g of Aloe-based drink to be taken each day in beverage form of 300 mL in addition to the normal diet and provided with an education to have a good diet for MetS. The control group was provided nutrition education to consume balanced, healthy diet, maintain body weight and follow active lifestyle for control of MetS. The intervention was given for 4 weeks. Adherence was confirmed through checking with the respondent and other family members.
Statistical methods
The characteristics of the participants were analyzed by using Shapiro-Wilk test. Differences in anthropometry data (body weight, body height and waist size), triglyceride, food intake data (total energy, fat and carbohydrate) between groups were tested with Independent t-test. Meanwhile, Mann-whitney was used for analyzing differences of age, clinical examination (blood pressure systolic and blood pressure diastolic), fasting blood glucose levels, HDL-C and protein intake between groups. Paired t-test was used for bivariate analysis of HOMA-IR data, whereas Wilcoxon test was used for GA, fasting blood glucose levels, and insulin levels. The data were processed by SPSS 21 program. The data were considered as significant level at p<0.05 two-tailed.
Results
Baseline Data
Seventy-five people were found to be above normal weight based on screening, out of them some subjects dropped out as they refused to provide blood samples. The remaining 47 respondents were randomized and divided into two groups: intervention (n=23) and control (n=24). In the end of study, 4 respondents of intervention group and 5 respondents of control group dropped out due they could not be followed up. The final respondent rate was 80.85% which consisted of 19 respondents of intervention and 19 respondents of control group.
Table 1 provides the characteristics data of two groups.
There were no differences in the characteristics of the subjects between the treatment and control groups (p>0.05) (age, body weight, body height, BMI, waist size, clinical/physical examination, fasting blood glucose, triglycerides, and HDL-C). It can be concluded that the subjects had the same characteristics at the baseline shown in Table 1 respectively.
Table 1 also showed that there were no significant differences in the energy intake (p=0.176), protein (p=0.549), and fat (p=0.841) between the treatment and control groups, while in carbohydrate intake (p = 0.023), there was a significant difference between the treatment and control groups.
Table 1: The baseline characteristics of the subjects based on the age, anthropometry, clinical examination, biochemical parameters, and food intake in both groups.
| Treatment (n=19) | Control (n=19) | p | |||
| X ± SD | Median (Min – Max) | X ± SD | Median(Min – Max) | ||
| Age (y) | 47±7.67 | 52(36-56) | 45±8.22 | 45(35-55) | 0.508b |
| Anthropometry | |||||
| Body Weight (kg) | 76.9±9.41 | 75.60(62.00-99.20) | 83.2±9.87 | 81.6(65.40-100) | 0.560a |
| Body Height (cm) | 160.3±10.71 | 160.9(140.60-176.30) | 164.5±7.70 | 165.6(150.1-180.2) | 0.177a |
| BMI | 30±2.97 | 29.02(25.53-37.28) | 30.5±2.68 | 30.39(26.25-36.47) | 0.448a |
| Waist Size (cm) | 94.4±6.12 | 93.00(83-107) | 95.5±7.75 | 94.9(81-109) | 0.619a |
| Clinical examination | |||||
| Blood Pressure systolic (mm Hg) | 130±13 | 130(110-160) | 127±16 | 130(100-150) | 0.523b |
| Blood Pressure diastolic (mm Hg) | 85±6 | 90 (70-90) | 85±6 | 90(70-93) | 0.974b |
| Biochemical Parameters | |||||
| Fasting blood glucose (mg/dL) | 135±56.98 | 119(86-332) | 121.84±45.06 | 109(84-268) | 0.199b |
| Triglyceride (mg/dL) | 199.4±100.94 | 174(48-403) | 193.7±69.39 | 192(53-337) | 0.842a |
| HDL-C (mg/dL) | 52.8±9.27 | 54(39-70) | 53.10±13.36 | 51(35-89) | 0.568b |
| Food Intakes | |||||
| Energy intake (kkal) | 2539±300 | 2506(2079-3036) | 2685±353 | 2787(2148-3487) | 0.176a |
| Protein Intake (g) | 85±14 | 81(60-116) | 91±15 | 89(73-122) | 0.549b |
| Fat Intake (g) | 97±19 | 98(54-128) | 99±27 | 92(54-162) | 0.841a |
| Carbohydrate Intake (g) | 317±51 | 317(235-421) | 362±65 | 358(256-475) | 0.023a |
a Independent t-test, b Mann-Whitney, significant if p-value<0,05
Glycated Albumin and HOMA-IR
Table 2 describes the changes in glucose levels, fasting insulin level, GA, and HOMA-IR in both groups. There was a significant difference between the treatment and control groups on the changes of fasting blood glucose, fasting insulin level, GA, and HOMA-IR (p=0.001; p<0.001; p<0.001; p<0.001). Fasting blood glucose, insulin, GA, and HOMA-IR before and after the administration of Aloe-based drink showed a significant change (p=0.001; p=0.006; p<0.001; p=0.001). All of the fasting blood glucose of the respondent in the intervention group improved, but 2 respondents had steady fasting blood glucose. One participant in the intervention group exhibited the fasting blood glucose improvement by 100 mg/dL. None got worse in the control, across the 4 weeks there was variation of fasting blood glucose in control group.
Table 2: The changes in FBG, fasting insulin, GA, and HOMA-IR before and after the administration of Aloe-based drink.
| Variables | Treatment (n=19) | Control (n=19) | p | ||
| X ± SD | Med (Min – Max) | X ± SD | Med (Min – Max) | ||
| FBG/Fasting Blood Glucose (mg/dL) | |||||
| pre | 135.7±56.98 | 119.00(86.00-332.00) | 121.8±45.06 | 109.00(84.00-268.00) | 0.001a |
| post | 133.3±42.22 | 99.00(80.00-239.00) | 125.7±40.28 | 118.00(72.00-254.00) | |
| ∆ | -22.5±24.08 | -16.00(-93.00-19.00) | 3.8 ±20.47 | 2.0(-37.00-51.00) | |
| p | 0.001b | 0.316b | |||
| Fasting insulin level (µIU/mL) | |||||
| pre | 10.7±4.87 | 10.95(0.14-18.72) | 8.3±2.97 | 8.85(3.88-16.94) | 0.000c |
| post | 7.4±4.51 | 5.80(2.21-16.86) | 9.9±4.12 | 9.04(4.27-20.54) | |
| ∆ | -22.5 ±24.08 | -2.73(-9.17-7.48) | 1.6 ±1.79 | 1.29(-0.90-4.98) | |
| p | 0.006b | 0.003b | |||
| GA (%) | |||||
| pre | 19.3±1.73 | 19.40(16.35-21.78) | 19.2±1.79 | 19.32(16.67-22.27) | 0.000a |
| post | 14.9±2.22 | 15.11(11.22-19.77) | 18.7±1.99 | 18.57(14.40-21.49) | |
| ∆ | -4.3±2.35 | -4.32(-9.00-(-1.20)) | -0.3±1.79 | -0.18(-4.22-2.88) | |
| p | 0.000d | 0.346d | |||
| HOMA-IR | |||||
| pre | 3.6±2.04 | 3.47(0.04-7.92) | 2.6±1.44 | 2.27(0.82-6.61) | 0.000a |
| post | 1.9±1.13 | 1.81(0.47-4.54) | 3.2±1.81 | 2.64(0.90-6.81) | |
| ∆ | -1.6 ±1.87 | -1.58(-4.66-1.77) | 0.6 ±0.93 | 0.37(-0.77-3.22) | |
| p | 0.001d | 0.014d | |||
a Independent t-test, b Wilcoxon, c Mann-Whitney, d Paired t-test, significant if p-value<0,05
Discussion
There was a significant difference in carbohydrate consumption at baseline, however this was considered not clinically significant. The screening results from this study in Central Java Regional Police were obtained that the subjects of treatment group and control group had the range age of 36-56 years and 35-55 years respectively. Age is one of the factors that could possibly affect the tissue function related to change of metabolism in the body25. The study by Sihombing (2015) stated that 18.2% the proportion of MetS had the age range by 35-44 years old and had the risk factors by 1.84 times than the subjects with the age of range by 25-34 years old26.
All participants in intervention group had insulin improvement, but 2 participants had steady insulin. The highest insulin improvement in intervention group was 9.17 µIU/mL. Look at the control group, insulin increased significantly (p=0.003). All participants in intervention group exhibited GA reduction, except for one participant. GA of one participant in intervention group exhibited the best improvement by 7.73%. There was no participant got worse of GA at the end of study either in intervention group or in control group. The intervention group showed a decrease of HOMA-IR, but three participants in intervention group had no change in HOMA-IR. At the end of study, control group had an elevation by 0.6 ±0.93 of HOMA-IR.
GA induces superoxide formation and stimulates NADPH oxidase activity. NADPH oxidase is the most major source of ROS production in non-phagocytic cells, including vascular smooth muscle cells9. The decrease of GA in the treatment group showed that there was a hyperglycemic improvement, while insignificant decrease of GA was concomitant with insignificant improvement of FBG in the control group. At the hyperglycemic state, albumin will be glycated so that the function of albumin as anti-inflammatory is disturbed. The disruption of the inflammatory system in the body will stimulate the formation of ROS. In this study, the consumption of Aloe-based drink was assumed to increase antioxidant status that resulted oxidative stress reduction, consequences for decreasing GA27. The study of Cardenas-Ibarra’s stated that the administration of Aloe vera could reduce fasting hyperglycemia in a new case of diabetes type 221. In an another study conducted by Radha, the administration of Aloe-based drink made from Aloe vera gel has many benefits such as acts as an antihypercholesterolemic and antihyperglycemic for patients with DMT218.
This study revealed Aloe-based drink decreasing HOMA-IR. Aloe-emodin is an anthraquinone compound, extracted from Aloe vera gel that can reduce fat accumulation, suppress the pro-inflammatory cytokines induced inflammation and insulin secretion reduction19. The administration of Aloe-based drink was in accordance with the study by Choi (2013) about the administration of 700 mg Aloe vera that could reduce body weight, body fat mass, and insulin resistance in obesity with untreated pre-diabetes22. Aloe vera gel improves insulin sensitivity and has hypoglycemic and hypolipidemic effects as well as decreases adipocyte size. Aloe vera can improve insulin sensitivity by activating AMP-activated muscle protein kinase, which is important in glucose regulation and lipid metabolism22.
In this study, we obtained new finding that the administration of Aloe can reduce the levels of GA and improve the state of insulin resistance. Further study is needed to analyze the effectiveness in giving Aloe-based drink to patients with MetS who routinely consume the diabetic drugs with the composition and amount of diet that has been determined.
Conclusion
In conclusion, Aloe-based drink administration with a dose of 165 g / day for 30 days has proven to reduce glycated albumin and insulin resistance in people with MetS. Aloe-based drink can be used as an alternative functional food in people with MetS.
Acknowledgment
The authors would like to thank the Head of Community Resources of the Central Java Regional Police and the Members of the Central Java Regional Police who had participated in this study voluntarily. This study did not receive any grant from external funding agencies.
Conflicts of Interest
Authors declare that there are no conflicts of interest regarding the publication of this paper.
Funding Sources
Thank you to Diponegoro University for helping with the cost of publishing this research.
References
- Prasad M, Flowers E, Mathur A, Sridhar V, Molina C, Turakhia M. Effectiveness of a community screening program for metabolic syndrome and cardiovascular risk factor identification in young South Asians adults. Diabetes Metab Syndr Clin Res Rev. 2014;402(4):1–5.
CrossRef - Viscogliosi G, Andreozzi P, Chiriac IM, Cipriani E, Servello A, Ettorre E, et al. Screening cognition in the elderly with metabolic syndrome. Metab Syndr Relat Disord. 2012;10(5):358–62.
CrossRef - Wong Y, Roderick P, Somani B. Metabolic syndrome and kidney stone disease : a systematic review of literature. J Endourol. 2016;30(3):246–53.
CrossRef - WHO. Global status report on noncommunicable diseases. Geneva; 2014. 1–280 p.
CrossRef - Aydin S, Aksoy A, Aydin S, Kalayci M, Yilmaz M, Kuloglu T, et al. Today ’s and yesterday ’s of pathophysiology : biochemistry of metabolic syndrome and animal models. Nutrition. 2014;30(1):1–9.
CrossRef - Chan CL, Pyle L, Morehead R, Baumgartner A, Cree-green M, Nadeau KJ. The role of glycemia in insulin resistance in youth with type 1 and type 2 diabetes. Int Soc Pediatr Adolesc Diabetes. 2016;18(6):1–8.
CrossRef - Kurto S, Hatipo N, Maz M, Kendirci M. Insulin resistance in obese children and adolescents: HOMA-IR cut-off levels in the prepubertal and pubertal periods. J Clin Res Pediatr Endocrinol. 2010;2(3):100–6.
CrossRef - Yazdanpanah S, Rabiee M, Tahriri M, Rajab A, Jazayeri HE, Tayebi L. Evaluation of glycated albumin (GA) and GA / HbA1c ratio for diagnosis of diabetes and glycemic control: a comprehensive review. Crit Rev Clin Lab Sci. 2017;54(4):1–14.
CrossRef - Qi W, Niu J, Qin Q, Qiao Z, Gu Y. Astragaloside IV attenuates glycated albumin-induced epithelial-to- mesenchymal transition by inhibiting oxidative stress in renal proximal tubular cells. Cell Stress Chaperones. 2014;19(1):105–14.
CrossRef - Raghav A, Ahmad J. Glycated serum albumin : a potential disease marker and an intermediate index of diabetes control. Diabetes Metab Syndr Clin Res Rev. 2014;8(4):245–51.
CrossRef - Patche J, Girard D, Catan A, Boyer F, Dobi A, Planesse C, et al. Diabetes-induced hepatic oxidative stress: a new pathogenic role for glycated albumin. Free Radic Biol Med. 2016;102(11):1–45.
CrossRef - Goldin A, Beckman JA, Schmidt AM, Creager MA. Advanced glycation end products sparking the development of diabetic vascular injury. Am Hear Assoc. 2006;8(8):597–605.
CrossRef - Panahi Y, Sadat M, Khalili N, Naimi E. Antioxidant and anti-inflammatory effects of curcuminoid-piperine combination in subjects with metabolic syndrome: a randomized controlled trial and an updated meta-analysis. Clin Nutr. 2015;34(6):1101–8.
CrossRef - Habib SA, Saad EA, Elsharkawy AA, Attia ZR. Pro-inflammatory adipocytokines, oxidative stress, insulin, Zn and Cu: interrelations with obesity in egyptian non-diabetic obese children and adolescents. Adv Med Sci. 2015;60(2):179–85.
CrossRef - Salah F, El Y, Mahdhi A, Majdoub H, Jarroux N, Sakli F. Effect of the deacetylation degree on the antibacterial and antibiofilm activity of acemannan from Aloe vera. Ind Crop Prod. 2017;103:13–8.
CrossRef - Kang M, Young S, Taek Y, Kim E, Lee S, Ko S, et al. In vitro and in vivo antioxidant activities of polysaccharide purified from aloe vera ( Aloe barbadensis ) gel. Carbohydr Polym. 2014;99:365–71.
CrossRef - Sánchez-machado DI, López-cervantes J, Sendón R, Sanches- A. Aloe vera: ancient knowledge with new frontiers. Trends Food Sci Technol. 2017;61(12):94–102.
CrossRef - Radha MH, Laxmipriya NP. Evaluation of biological properties and clinical effectiveness of aloe vera: a systematic review. J Tradit Complement Med. 2015;5:21–6.
CrossRef - Kammoun M, Miladi S, Ali Y Ben, Damak M, Gargouri Y, Bezzine S. In vitro study of the PLA2 inhibition and antioxidant activities of Aloe vera leaf skin extracts. Lipids Health Dis. 2011;10(1):1–7.
CrossRef - Riyanto, Wariyah C. Stabilitas sifat antioksidatif lidah buaya (Aloe vera var. chinensis) selama pengolahan minuman lidah buaya. AGRITECH. 2012;32(1):73–8.
- Cardenas-Ibarra L, Villarreal-Perez JZ, Lira-Castillo JC, Nava-Aleman A. Randomized double blind crossover trial of Aloe vera, Cnidoscolus chayamansa and placebo for reducing hyperglycemia in women with early metabolic syndrome. Clin Nutr Exp. 2017;14(5):1–12.
CrossRef - Choi H, Kim S, Son K, Oh B, Cho B. Metabolic effects of aloe vera gel complex in obese prediabetes and early non-treated diabetic patients: randomized controlled trial. Nutrition. 2013;29(9):1110–4.
CrossRef - Devaraj S, Yimam M, Brownell LA, Jialal I, Singh S, Jia Q. Effects of aloe vera supplementation in subjects with prediabetes/metabolic syndrome. Metab Syndr Relat Disord. 2013;11(1):35–40.
CrossRef - Oladosu WO, Onwah AL, Oladosu RO, Ahmed A, Osinubi MO, Gbotosho OA, et al. Homeostatic model assessment of insulin activity and iron profile among regular blood donors at a tertiary health centre, South‑West Nigeria. Int J Appl Basic Med Res. 2020;10:252–5.
CrossRef - Ghezzi AC, Cambri LT, Botezelli JD, Ribeiro C, Dalia RA, Alice M, et al. Metabolic syndrome markers in wistar rats of different ages. Diabetol Metab Syndr. 2012;4(16):1–7.
CrossRef - Sihombing M, Tjandrarini H. Faktor risiko sindrom metabolik pada orang dewasa di kota Bogor (risk factors metabolic syndrome among adults in Bogor). Penelit Gizi dan Makanan. 2015;38(1):21–30.
CrossRef - Ikezaki H, Furusyo N, Ihara T, Hayashi T, Ura K, Hiramine S, et al. Glycated albumin as a diagnostic tool for diabetes in a general Japanese population. Metabolism. 2015;64(6):698–705.
CrossRef
Accepted on: 09 June 2022
Second Review by: Poonam Jethwani India
Final Approval by: Prof. Suhad Maatoug Bahijri





Web of Science Coverage
Emerging Sources Citation Index (ESCI)
2024 Journal Impact Factor: 1.1
Scopus Journal Metrics
CiteScore 2025: 2.6
CiteScore Details
Sustainable Nutrition: Food Systems, Nutrient Retention, and Public Health Impact
![]()
This journal is a member of, and subscribes to the principles of, the Committee on Publication Ethics (COPE)








