The Association of Higher Composite Biomarker Score of Antioxidant Vitamins with Lower Cardiovascular Diseases Risk: A Cross-Sectional Study
Thaer M. M. Al-Rammahi1*
and Ammar Waham Ashor2, 3 1Department of Chemistry, College of Science, University of Kerbala, Karbala, Iraq.
2Department of Internal Medicine, College of Medicine, Mustansiriyah University, Baghdad, Iraq.
3Natioanl Diabetes Center, Mustansiriyah University, Baghdad, Iraq.
Corresponding Author Email: thaer.alramahi@uokerbala.edu.iq
DOI : http://dx.doi.org/10.12944/CRNFSJ.9.3.21
Download this article as:
![]()
Biomarkers for the dietary system, which includes a mixed fruit and vegetable (FV), are needed to understand the association of FV intake with a reduction in cardiovascular diseases risk. This is a cross-sectional study that aims to find the potential relationship between a high composite score comprised of antioxidant vitamins and a lower incidence of cardiovascular diseases (CVD). A total of 94 (42 males and 52 females) participants (mean age ± SD: 51.7 ± 9.4 years) completed a specific questionnaire including a quick food scan, which has designed by the American National Institutes of Health. The vitamins A, C, and E were determined using high-performance liquid chromatography (HPLC). An enzymatic colorimetric method was used to determine other biomarkers [fasting blood sugar (FBS), haemoglobin A1c (HbA1c), and lipid profile]. A Composite Biomarker Score (CBS) comprising of the plasma vitamins (A, C, and E) have been derived. The results showed that male participants demonstrated significantly higher atherosclerotic cardiovascular disease (ASCVD) risk than female participants. Female participants with greater ASCVD risk were associated with significantly higher age, total cholesterol, and triglyceride concentrations. Additionally, there is a significant relationship between the CBS with lower ASCVD risk. Consequently, it can be concluded that higher concentrations of serum antioxidant vitamins are related to a reduction in cardiovascular diseases risk.
KEYWORDS:Antioxidants; Atherosclerosis; HbA1C; Vitamins
Introduction
Cardiovascular disease (CVD) is considered the main reason for death and disability in many countries. In 2018, the recording data of the World Health Organization exhibited that CVD is the first reason of death globally, about 31% (17.9 million people die every year) worldwide. In addition, these data mentioned about 32,463 (18%) Iraqis were died due to CVD.1 Consequently, CVD represents a global health issue for healthcare systems, especially for low- and middle-income states. Generally, CVD can be diagnosed by a group of disorders, which are related to intricate interactions among the risk factors affecting such as smoking, dyslipidemia, hypertension, and other diseases.2
The ASCVD risk score was developed by the American Heart Association/American College of Cardiology in 2013. The risk score evaluates variables including sex, age, ethnicity, total cholesterol (T Ch), high-density lipoprotein (HDL), blood pressure, diabetes mellitus, and smoking.3 The ASCVD risk score estimates the 10-year risk of developing major cardiovascular diseases in the general population in primary prevention settings.4
In the twentieth century, the connotation of oxidative stress as a trigger of disease and death was assumed. 5 In addition, the relationship between cardiovascular diseases (CVD) and the markers of oxidative stress was proven.6-11 As a result, oxidative stress has a key role in the pathogenesis of chronic diseases.12-14 Hence, the oxidative load is increased by diminishing the antioxidant defense system of the body.15 Consequently, oxidative stress is likely seemed to be a significant factor in CVD.
The antioxidant defense system involves both the exogenous (diet) derived compounds such as vitamin A (beta-carotene), vitamin C (ascorbic acid), vitamin E (alpha-tocopherol), flavonoids and trace metals (selenium, manganese, zinc); and the endogenous (e.g., superoxide dismutase (SOD), glutathione peroxidase (GPx) and catalase).16-18 Vitamins consist of main micronutrients with antioxidant potential, which can provide a harmonious treatment for patients with chronic diseases.19 Vitamins can be found in various types of fruits and vegetables. As a result, a diet with a high value of fruits and vegetables may have a significant role to reduce the risk of CVD. This work will present the association of antioxidant vitamins level with the reduction of the risk of cardiovascular disease (CVD).
Methods
Study Design
This cross-sectional study was carried out at the Department of Chemistry, College of Science, University of Kerbala, Karbala, Iraq, and cooperation with Imam Hussain (AS) Medical City, Karbala, Iraq. The work was carried out from November 2018 to March 2020. The study involved ninety-four participants (mean age ± SD: 51.7 ± 9.4 years). The protocol of work was in accordance with the Helsinki Declaration and confirmed by the Council of College of Science, University of Kerbala (Approval Code: No. 109 in 29.11.2018). In this study, all participants were clearly informed and verbal consent was taken. Demographic data include gender (male, female), age, smoking status, hypertension, duration of diabetes, coronary artery diseases, stroke, and other diseases, were recorded. In addition, information regarding such as the family history of cardiovascular diseases and the medication were considered.
Anthropometry and Blood Pressure Measurements
Standing measurements of weight, height, and waist circumference were measured for all participants who were wearing light clothing and no shoes. Body mass index (BMI in Kg/m2) and fat percentage were determined using a bioimpedance monitor “Lloyds Pharmacy Handheld Body Composition Monitor, Lloyd’s Pharmacy Limited, Coventry, United Kingdom”. Blood pressure was evaluated using an automated Blood Pressure Monitor “Omron Healthcare Co., Ltd. Kyoto, Japan”. Two blood pressure measurements (mean systolic and mean diastolic blood pressure) were recorded one minute apart.
Monitoring of Fruit and Vegetable Intake
All participants in this work were administered by using screeners of fruit and vegetable (FV_ Screener), which are designed to monitor the amount of fruit and vegetable in the daily dietary system for one month.20 The cumulative score, ranging from 0 to 94, was determined to assess the adherence to a healthy dietary index (i.e., higher scores indicate a greater adherence).21
Blood Sample Processing and Biochemical Assays
Participants were fasting for at least 8 hours before their visit. Venous blood samples were collected in the morning by 12.00 p.m. in Imam Hussain (AS) hospital, Holy Karbala City, Iraq. Blood samples were placed in EDTA and SSGT tubes to obtain plasma and serum after centrifugation at 4000 g for 10 minutes. After that aliquot of plasma and serum were stored in a freezer (-25 C°) for further analyses. Biochemical markers, which include fasting blood sugar (FBS), glycated hemoglobin (HbA1c), and lipid profile (total cholesterol, triglyceride, LDL, and HDL) were determined by using an enzymatic colorimetric method by using Cobas biochemical analyzer (Roche, Bern, Switzerland). High-performance liquid chromatography (HPLC) (Shimadzu Corporation, Japan) was used to determine vitamins A, C, and E.22,23
A Composite Biomarker Score (CBS) was derived from plasma vitamin A, C, and E concentrations as antioxidant capacity.24 The composite biomarker score (CBS) was measured by summing standardized values for the levels of vitamin A, C and E in plasma. Variables were standardized as follows; (i) the individual mean was subtracted from the sample mean and then divided by the SD, and (ii) the score was divided by three to account for the number of individual biomarkers included in the score.25
Statistical Study
The Statistical Package for the Social Sciences (SPSS) software for Windows, Version 25.0. Armonk, NY: IBM Corp” was used to analyze the data. All data were examined for normal distribution and appropriate statistical analysis was applied. Data were summarized and displayed as mean ± standard deviation. Student T-test for independent samples was applied to compare groups. Pearson’s correlation test was applied to examine correlations between CBS, FV screeners, and metabolic markers. In addition, GraphPad Prism version 8 “GraphPad software, CA, USA” was utilized to construct the graphs. Statistical significance was considered at P < 0.05.
Results
The relationship between the level of antioxidant vitamins (A, C, and E), and the decrease of cardiovascular diseases risk is supported by various biomarkers such as (HbA1c, FBS, and other lipid profile tests). Table 1 display the baseline characterization of participants (n= 94) in completing the study (42 males, 52 females) during the period (2018 to 2020).
Table 1: Characteristics of the Participants in the Study.
| Male | Female | |||||
| Low ASCVD risk | High ASCVD risk | P-Value | Low ASCVD risk | High ASCVD risk | P-Value | |
| Number | 8 | 34 | 38 | 14 | ||
| Age (years) | 44.00±4.14 | 56.91±6.77 | 0.001 | 49.58±6.63 | 58.29±4.66 | 0.001 |
| Weight (kg) | 83.63±7.96 | 85.71±18.57 | 0.76 | 78.84±16.63 | 75.93±9.38 | 0.43 |
| Waist circumference (cm) | 96.69±6.13 | 103.23±12.59 | 0.16 | 102.58±11.10 | 102.79±9.03 | 0.95 |
| Body mass index (Kg/m2) | 28.56±3.43 | 29.27±5.33 | 0.72 | 31.37±5.74 | 31.31±3.69 | 0.96 |
| Fat mass % | 28.74±4.53 | 32.05±6.35 | 0.17 | 43.68±6.77 | 45.71±3.99 | 0.29 |
| Systolic BP (mmHg) | 139.13±10.93 | 143.00±19.37 | 0.59 | 130.61±14.65 | 144.71±13.93 | 0.003 |
| Diastolic BP (mmHg) | 85.88±5.44 | 82.21±8.96 | 0.27 | 77.76±7.74 | 81.36±9.55 | 0.17 |
| HbA1C % | 6.18±2.16 | 8.53±2.19 | 0.01 | 8.53±2.56 | 8.97±1.43 | 0.54 |
| FBS (mg/dl) | 142.61±62.26 | 199.76±66.93 | 0.03 | 208.33±94.56 | 201.09±59.29 | 0.79 |
| Total Cholesterol (mg/dl) | 169.49±41.23 | 183.50±55.55 | 0.51 | 184.25±44.99 | 222.85±52.22 | 0.01 |
| LDL (mg/dl) | 111.06±35.25 | 119.87±37.55 | 0.55 | 127.87±41.67 | 153.84±48.76 | 0.06 |
| HDL (mg/dl) | 39.56±10.44 | 37.91±6.13 | 0.56 | 43.56±11.30 | 44.64±9.91 | 0.76 |
| Triglycerides (mg/dl) | 185.80±80.68 | 191.46±91.67 | 0.87 | 181.03±109.75 | 269.91±176.33 | 0.03 |
| Handgrip strength | 34.75±6.57 | 33.29±6.24 | 0.56 | 19.83±5.24 | 19.69±4.97 | 0.93 |
| FV_Screener | 4.67±1.31 | 5.27±2.97 | 0.09 | 4.62±1.96 | 4.15±1.9 | 0.98 |
The statistical analysis has shown that the male participants demonstrated significantly greater ASCVD risk than female participants (P < 0.001), as illustrated in Figure 1. Furthermore, the male participants with a higher ASCVD risk showed significantly higher age and HbA1c than male participants with a lower ASCVD risk. However, female participants with greater ASCVD risk were associated with significantly higher age, total cholesterol, and triglyceride concentrations than female participants with lower ASCVD risk.
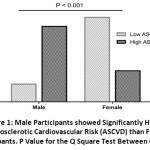 |
Figure 1: Male Participants showed Significantly Higher Atherosclerotic Cardiovascular Risk (ASCVD) than Female Participants. P-Value for the Q Square Test Between Groups. |
The analysis data of biomarkers composite score has exhibited that there is a significant relationship between the level of vitamins as antioxidants with lower ASCVD risk for all participants (male and female), Figure 2.
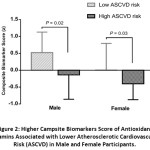 |
Figure 2: Higher Campsite Biomarkers Score of Antioxidant Vitamins Associated with Lower Atherosclerotic Cardiovascular Risk (ASCVD) in Male and Female Participants. |
On the other hand, FV_ Screeners appears that there is no significant difference between higher and lower ASCVD for both groups (male and female) as shown in Figure 3.
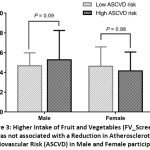 |
Figure 3: Higher Intake of Fruit and Vegetables (FV_Screener) was not associated with a Reduction in Atherosclerotic Cardiovascular Risk (ASCVD) in Male and Female participants. |
Discussion
The current study investigates the impact of antioxidant status vitamins on lowering cardiovascular disease risk. We found, daily consumption of fruit and vegetable enhanced nutrition status and significantly raised circulating levels of vitamins (A, C, and E). The composite biomarker score (CBS) was measured by summing standardized values for plasma levels of vitamin A, C and E. The results of the work show that all participants with higher CBS scores were associated with lower ASCVD risk than those with lower concentrations of vitamins.
Numerous studies have shown the essential role of reactive oxygen species (ROS) in endothelial dysfunction and the progressive deterioration of cardiovascular health. The ROS impair vasodilator capacity and induce local injury and attraction of inflammatory cells. This local inflammatory response significantly contributes to the onset of atherosclerosis in the wall of blood vessels.26
Fruits and vegetables are regarded as a fundamental source of vitamin A and C in the diet. Moreover, these vitamins can be considered as potential biomarkers of fruit and vegetable intake. Using a composite score of the blood concentrations of these vitamins may better reflect the mixed intake of fruits and vegetables.27
Previously conducted meta-analyses showed that antioxidant vitamins significantly improved biological markers of cardiovascular diseases e.g., endothelial function, blood pressure, lipid profile, and glycaemic indices.28-32
Moreover, a meta-analysis of cohort studies demonstrated that antioxidant vitamins significantly reduce the risk of coronary artery disease.33
This fact is corresponding with previous suggestions, which referred to the relationship between the intake of various vitamins and the level of lipids such as total cholesterol, LDL-C, and HDL-C. Consequently, an increase in of intake fruits and vegetable has a significant impact on reduce of the risk of cardiovascular diseases.34-36
Our findings also show that the antioxidant vitamins decrease the level of cholesterol, decrease the level of HbA1C, blood pressure, etc. These findings are associated with the results of recent studies.37-39
The biostatistical analysis for the fruit and vegetable screeners demonstrate no significant effect of fruit and vegetable intake on ASCVD because questionnaires are less accurate in reflecting dietary intake than measuring the concentrations of vitamins in the blood.
Our study has limitations. The sample size was small in comparison with similar studies. However, we included only eligible participants and we measured the relevant markers related to cardiovascular disease risk. Additionally, our study is a cross-sectional study rather than randomised controlled trial. Randomised controlled trials (RCTs) have better evidence than cross-sectional studies. However, the RCTs need more time and effort to be conducted. Finally, we could not measure relevant biomarkers of oxidative stress and correlate these with the intake of antioxidant vitamins.
Conclusions
In this study, we tried to clarify the role of antioxidant vitamins in reduce of cardiovascular diseases risk. Vitamins (A, C and E) are important micronutrients, which have important roles in healthy. As discussed above, evidence strongly suggests that a higher intake of antioxidants significantly reduces the risk of cardiovascular disease in the Iraqi population.
Regarding fruit and vegetable intake, no significant difference between lower and higher ASCVD groups was noticed. However, the biomarker composite score of antioxidant vitamins concentrations showed significantly higher concentrations in male and female participants with lower ASCVD risk.
An increase in sample size is really recommended to obviously investigate the association of ASCVD with intake of fruit and vegetable as main natural sources of antioxidant vitamins.
Acknowledgments
The authors would like to thank the department of chemistry, the college of science, the university of Kerbela for all their support.
Funding Sources
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of Interest
The authors declare no conflict of interest.
References
- World Health Organization. Noncommunicable diseases country profiles 2018. World Health Organization Press; Geneva, Switzerland. September 2018; https://www.who.int/nmh/publications/ncd-profiles-2018/en/ (Accessed on 31 May 2021).
- Hobbs F.D.R. Cardiovascular disease: Different strategies for primary and secondary prevention. 2004; 90(10): 1217-1223. DOI: 10.1136/hrt.2003.027680.
CrossRef - Goff D. C., Lloyd-Jones D. M., Bennett G., Coady S., D’Agostino R. B., Gibbons R., Greenland P., Lackland D. T., Levy D., O’Donnell C. J., Robinson J. G., Schwartz J. S., Shero S. T., Smith S. C., Sorlie P., Stone N. J., Wilson P. W. F. 2013 ACC/AHA Guideline on the Assessment of Cardiovascular Risk. Circulation. 2014; 129(25): S49-S73. DOI: 10.1161/01.cir.0000437741.48606.98.
CrossRef - Azevedo T. A., Moreira M. L. V., Nucera A. P. C. S. Cardiovascular Risk Estimation by the ASCVD Risk Estimator Application in a University Hospital. International Journal of Cardiovascular Sciences. 2018; 31(5): 492-498. DOI: 10.5935/2359-4802.20180052.
CrossRef - Harman D., Aging. a theory based on free radical and radiation chemistry. Gerontol. 1956; 11(3): 298–300. DOI: 10.1093/geronj/11.3.298.
CrossRef - Munzel T., Gori T., Bruno R.M., Taddei S. Is oxidative stress a therapeutic target in cardiovascular disease? Heart J. 2010; 31(22): 2741–2748. DOI: 10.1093/eurheartj/ehq396.
CrossRef - Karbach S., Wenzel P., Waisman A., Munzel T., Daiber A. eNOS uncoupling in cardiovascular diseases–the role of oxidative stress and inflammation. Pharmaceut.Des. 2014; 20(22): 3579–3594. DOI: 10.2174/13816128113196660748.
CrossRef - Daiber A., Oelze M., Daub S., Steven S., Schuff A., Kroller-Schon S., Hausding M., Wenzel P., Schulz E., Gori T., Munzel T. Vascular redox signaling, redox switches in endothelial nitric oxide synthase and endothelial dysfunction, in I. Laher (Ed.), Systems Biology of Free Radicals and Antioxidants. Springer-Verlag, Berlin Heidelberg. 2014; 1177–1211. DOI: 10.1007/978-3-642-30018-9_48.
CrossRef - Daiber A., Di Lisa F., Oelze M., Kroller-Schon S., Steven S., Schulz E., Munzel T. Crosstalk of mitochondria with NADPH oxidase via reactive oxygen and nitrogen species signaling and its role for vascular function. J. Pharmacol. 2017; 174(12): 1670–1689. DOI: 10.1111/bph.13403.
CrossRef - Cuadrado A., Manda G., Hassan A., Alcaraz M. J., Barbas C., Daiber A., Ghezzi P., Leon R., Lopez M. G., Oliva B., Pajares M., Rojo A. I., Robledinos-Anton N., Valverde A. M., Guney E., Schmidt H. Transcription factor NRF2 as a therapeutic target for chronic diseases: a systems medicine approach. Rev. 2018; 70(2): 348–383. DOI: 10.1124/pr.117.014753.
CrossRef - Casas A.I., Nogales C., Mucke H.A.M., Petraina A., Cuadrado A., Rojo A.I., Ghezzi P., Jaquet V., Augsburger F., Dufrasne F., Soubhye J., Deshwal S., Sante M. Di, Kaludercic N., Di Lisa F., Schmidt H. On the clinical pharmacology of reactive oxygen species. Rev. 2020; 72(4): 801–828. DOI: 10.1124/pr.120.019422.
CrossRef - Johansen J. S., Harris A. K., Rychly D. J., Ergul A. Oxidative stress, and the use of antioxidants in diabetes: linking basic science to clinical practice. Cardiovasc Diabetol. 2005; 4(5): 1-11. DOI: 10.1186/1475-2840-4-5.
CrossRef - Ceriello A, Testa R, Genovese S. Clinical implications of oxidative stress and potential role of natural antioxidants in diabetic vascular complications. Nutr Metab Cardiovasc Dis. 2016; 26(4): 285-292. DOI: 10.1016/j.numecd.2016.01.006.
CrossRef - Abdulrazzaq V. M., Al-Rammahi T. M. M., and Ashor A. W. Association of handgrip strength with cardiometabolic markers in type 2 diabetes mellitus. AIP Conference Proceedings. 2020; 2290(030041): 1-10. DOI: 10.1063/5.0027494.
CrossRef - Manna P, Jain S. K. Obesity, oxidative stress, adipose tissue dysfunction, and the associated health risks: causes and therapeutic strategies. Metab Syndr Relat Disord. 2015; 13(10): 423-444. DOI: 10.1089/met.2015.0095.
CrossRef - Diane L. T. Antioxidant consumption and risk of coronary heart disease: emphasis on vitamin C, vitamin E, and beta-carotene. 1999; 99(4): 591–595. DOI: 10.1161/01.CIR.99.4.591.
CrossRef - Luciak M. Antioxidants in the treatment of patients with renal failure. Rocz Akad Med Bialymst. 2004; 49: 157–161. https://pubmed.ncbi.nlm.nih.gov/15631333/ (Accessed on 31 May 2021).
- Pham-Huy L. A., He H., Pham-Huy C. Free radicals, antioxidants in disease and health. Int J Biomed Sci. 2008; 4(2): 89–96. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3614697/ (Accessed on 31 May 2021).
- Maria E. B., Fernanda S. T., Antonio M. M., Helena H. B., Astrid W., Fernando Fernandez‑Limos, Roberto P. Antioxidant effects of vitamins in type 2 diabetes: a meta-analysis of randomized controlled trials. Diabetol Metab Syndr. 2018; 10(18): 1-12. DOI: 10.1186/s13098-018-0318-5.
CrossRef - Frances E. T., Amy F. S. Dietary Assessment Methodology. In: Coulston A., Boushey C., Ferruzzi M., Delahanty L. Nutrition in the Prevention and Treatment of Disease. ELSEVIER; 2017: 5-30. DOI: 10.1016/B978-0-12-802928-2.00001-1.
CrossRef - Emadian A., England C. Y., Thompson J. L. Dietary intake and factors influencing eating behaviours in overweight and obese South Asian men living in the UK: a mixed-method study. BMJ Open. 2017; 7(7): 1-11. DOI: 10.1136/bmjopen-2017-016919.
CrossRef - Talwar D., Ha T. K. K., Cooney J., Brownlee C., St Jo’Reilly D. A routine method for the simultaneous measurement of retinol, α-tocopherol and five carotenoids in human plasma by reverse-phase HPLC. Clinica Chimica Acta. 1998; 270(2): 85-100. DOI: 10.1016/s0009-8981(97)00224-6.
CrossRef - Kim Y., Kim M. G. HPLC-UV method for the simultaneous determinations of ascorbic acid and dehydroascorbic acid in human plasma. Translational and Clinical Pharmacology. 2016; 24(1): 37-42. DOI: 10.12793/tcp.2016.24.1.37.
CrossRef - Valdés-Ramos R., Guadarrama-López A. L., Martínez-Carrillo B. E., Benítez-Arciniega A. D. Vitamins and type 2 diabetes mellitus. Endocr Metab Immune Disord Drug Targets. 2015; 15(1): 54-63. DOI: 10.2174/1871530314666141111103217.
CrossRef - Cooper A. J., Forouhi N. G., Ye Z., Buijsse B., Arriola L., Balkau B., Barricarte A., Beulens J. W., Boeing H., Büchner F. L. Fruit and vegetable intake and type 2 diabetes: EPIC-InterAct prospective study and meta-analysis. Eur J Clin Nutr. 2012; 66(10):1082-1092. DOI: 10.1038/ejcn.2012.85.
CrossRef - Bielli A., Scioli M. G., Mazzaglia D., Doldo E., Orlandi A. Antioxidants and vascular health. Life Sciences. 2015; 143: 209–216. DOI: 10.1016/j.lfs.2015.11.012.
CrossRef - Cooper A. J., Sharp S. J., Luben R. N., Khaw K. T., Wareham N. J., Forouhi N. G. The association between a biomarker score for fruit and vegetable intake and incident type 2 diabetes: the EPIC-Norfolk study. Eur J Clin Nutr. 2015; 69(4): 449-54. DOI: 10.1038/ejcn.2014.246.
CrossRef - Ashor A. W., Siervo M., Lara J., Oggioni C., Afshar S., Mathers J. C. Effect of vitamin C and vitamin E supplementation on endothelial function: a systematic review and meta-analysis of randomised controlled trials. British Journal of Nutrition. 2015; 113: 1182–1194. DOI:10.1017/S0007114515000227.
CrossRef - Ashor A., Siervo M., Lara J., Oggioni C., Mathers J. C. Antioxidant Vitamin Supplementation Reduces Arterial Stiffness in Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. The journal of Nutrition. 2014; 144(10): 1594-1602. DOI: 10.3945/jn.114.195826.
CrossRef - Ashor A. W., Shannon O. M., Werner A-D., Scialo F., Gilliard C. N., Cassel K. S., Seal C. J., Zheng D., Mathers J. C., Siervo M. Effects of inorganic nitrate and vitamin C co-supplementation on blood pressure and vascular function in younger and older healthy adults: A randomised double-blind crossover trial. Clin Nutr. 2020; 39(3):708-717. DOI: 10.1016/j.clnu.2019.03.006.
CrossRef - Ashor A. W., Siervo M., van der Velde F., Willis N. D., Mathers J. C. Systematic review and meta-analysis of randomised controlled trials testing the effects of vitamin C supplementation on blood lipids. Clin Nutr. 2016; 35(3):626-37. DOI: 10.1016/j.clnu.2015.05.021.
CrossRef - Ashor A. W., Werner A. D., Lara J., Willis N. D., Mathers J. C., Siervo M. Effects of vitamin C supplementation on glycaemic control: a systematic review and meta-analysis of randomized controlled trials. Eur J Clin Nutr. 2017; 71(12):1371-1380. DOI: 10.1038/ejcn.2017.24.
CrossRef - Ye Z., Song H. Antioxidant vitamins intake and the risk of coronary heart disease: a meta-analysis of cohort studies. European journal of cardiovascular prevention and rehabilitation. 2008; 15(1): 26–34. DOI: 10.1097/HJR.0b013e3282f11f95.
CrossRef - Levy M. A., McKinnon T., Goldfine H., Enomoto A., Schneider E., Cuomo J. Consumption of a multivitamin/multimineral supplement for 4 weeks improves nutritional status and markers of cardiovascular health. Journal of Functional Foods. 2019; 62:1-8. DOI: 10.1016/j.jff.2019.103511.
CrossRef - White D. J., Cox K. H., Peters R., Pipingas A., Scholey A. B. Effects of four-week supplementation with a multi-vitamin/mineral preparation on mood and blood biomarkers in young adults: A randomized, double-blind. placebo-controlled trial. Nutrients, 2015; 7(11): 9005–9017. DOI: 10.3390/nu7115451.
CrossRef - Mierzecki A., Kloda K., Bukowska H., Chelstowski K., Makarewicz-Wujec M., Kozlowska-Wojciechowska M. Association between low-dose folic acid supplementation and blood lipids concentrations in male and female subjects with atherosclerosis risk factors. Medical Science Monitor. 2013; 19: 733–739. DOI: 10.12659/MSM.889087.
CrossRef - Taneera J., Awadallah S., Mohammed A. K., Unnikannan H., Sulaiman N. Vitamin A levels are decreased but not influenced by glucose- or lipid-lowering medications in subjects with type 2 diabetes. Saudi Journal of Biological Sciences. 2021; 28(1): 572–577. DOI: 10.1016/j.sjbs.2020.10.044.
CrossRef - Sunga M., Rhieb S., Kim J. H., Lee S. W., Ha E. K., Jee H. M., Eun-Gyong Y., Chae K. Y., Han M. Y. Assessment of vitamin D, exercise, and lipid profile associated with excessive daytime sleepiness in school children. Sleep Medicine. 2021; 77: 51-57. DOI: 10.1016/j.sleep.2020.11.017.
CrossRef - Delosière M., Durand D., Bourguet C., Terlouw E. M. C. Lipid oxidation, pre-slaughter animal stress and meat packaging: Can dietary supplementation of vitamin E and plant extracts come to the rescue? Food Chemistry. 2020; 309: 125668-125672. DOI: 10.1016/j.foodchem.2019.125668.
CrossRef
Accepted on: 26 Oct 2021
Second Review by: Dr. Alireza Mohtashami Iran
Final Approval by: Prof. Shwu-Huey Sherry Yang





Web of Science Coverage
Emerging Sources Citation Index (ESCI)
2024 Journal Impact Factor: 1.1
Scopus Journal Metrics
CiteScore 2025: 2.6
CiteScore Details
Sustainable Nutrition: Food Systems, Nutrient Retention, and Public Health Impact
![]()
This journal is a member of, and subscribes to the principles of, the Committee on Publication Ethics (COPE)








