Treatment of Metabolic Alkalosis with Rice Broth
Hayder Aledan1*
, Zahraa Jasim3 and Manal Abdul Razak4 1Department of Medicine, Division of Nephrology, Basra College of Medicine, University of Basra, Basra, Iraq.
2Department of Medicine, Division of Nephrology, Arab Board of Health Specialization, Baghdad, Iraq.
3Department of Medicine, Basra College of Medicine, University of Basra, Basra, Iraq.
4Department of Medicine, Baghdad College of Medicine, University of Baghdad, Baghdad, Iraq.
Corresponding Author Email: hayder.aledan@uobasrah.edu.iq
DOI : http://dx.doi.org/10.12944/CRNFSJ.9.2.22
Download this article as:
![]()
The available treatments of metabolic alkalosis should be given in the hospital and may be associated with serious adverse events. We aimed to use rice broth for treatment of metabolic alkalosis. Patients with metabolic alkalosis were received oral rice broth solution; serum electrolytes and acid-base parameters were measured before and after the treatment. The majority of patients were older and in the ICU. After treatment with rice broth solution, there was statistical significant decreased in blood PH and serum [HCO3-] from a mean of 7.45 ± 0.03 to 7.4 ± 0.009 and 34.5 ± 4.4 to 24.9 ± 1.1 mmol/l respectively and statistical significant increase in serum [Na+], serum [Cl-], serum [K+], serum [Ca+2], serum [PO4-2] and serum [Mg+2] from a mean of 132.5 ± 3.7 to 136.5 ± 1.9 mmol/l, 93.2 ± 5.4 to 101.9 ± 2.7 mmol/l, 3.1 ± 0.3 to 3.6 ± 0.2 mmol/l, 0.99 ± 0.1 to 1 ± 0.1mmol/l, 3.4 ± 0.5 to 3.6 ± 0.4 mg/dl and 1.88 ± 0.2 to 2.28 ± 0.17 mg/dl respectively. Rice broth is an effective oral treatment of metabolic alkalosis.
KEYWORDS:Diuretics; Metabolic Alkalosis; Nasogastric Suction; Rice Broth Solution; Vomiting; 0.9% Isotonic Saline
Introduction
Metabolic alkalosis is the most common acid-base disorder and may accounted for half of the cases 1. It is associated with high mortality, 45% with arterial PH of 7.55 and 80% with arterial PH greater than 7.65 2. Chloride and potassium depletions cause both initiation and maintenance of metabolic alkalosis. Gastrointestinal loss of chloride occurs in vomiting or prolonged nasogastric suction 3, VIPoma of the rectum 4, congenital chloride diarrhea 5. Renal loss of chloride occurs with use of thiazide and loop diuretics and in chronic respiratory acidosis 6. Skin loss of chloride occurs in cystic fibrosis 7. Chloride depletion leads to maintenance of metabolic alkalosis by causing volume contraction with increased reabsorption of fluid and bicarbonate in the proximal tubules 8. Potassium depletion causes metabolic alkalosis through several mechanisms. First, potassium ions are shifted out of the cells in exchange for sodium and hydrogen ions 9,10. Second, hypokalemia stimulates renal ammonia synthesis leading to increase in renal net-acid excretion 11,12. Third, hypokalemia causes intracellular acidosis which increases hydrogen ions secretion by the proximal tubules 13. Fourth, hypokalemia leads to increased activity of the apical H-ATPase and H-K ATPase pumps in the collecting duct with reabsorption of potassium in exchange for hydrogen 14. Finally, severe hypokalemia is associated with downregulation of chloride transporters with renal chloride loss 15. Metabolic alkalosis may be asymptomatic or presented with symptoms of volume depletion or hypokalemia or presented with severe symptoms such as agitation, seizure and cardiac arrythmias 16. Spot urine chloride is of diagnostic importance, urine chloride less than 20 mmol/L occurs in vomiting, nasogastric suction, surreptitious diuretics use, laxative abuse, VIPoma and congenital chloride diarrhea, urine chloride more than 20 mmol/L occurs in real or apparent mineralocorticoid excess 17. If there is hypovolemia and chloride depletion, 3-5 liters of 0.9% isotonic saline plus 20 mmol/L potassium chloride added to the administered fluid is the appropriate treatment. A prompt alkaline diuresis leading to correction of metabolic alkalosis 18,19. Intravenous hydrochloric acid may be indicated in severe metabolic alkalosis (PH > 7.55) with serious manifestations, however it should be given in the ICU through central veins 20,21. Ammonium chloride is an alternative but it is contraindicated in renal or hepatic failure 22. Acetazolamide may cause alkaline diuresis but on the expense of urinary sodium and potassium loss 23.
Our aim is to find a safe and effective oral solution for treatment of metabolic alkalosis that can be given at home.
Methods
This was a prospective cohort interventional study of patients with metabolic alkalosis consulted the outpatient’s clinic or admitted in the general medical floor or intensive care unit at Baghdad and Basra Teaching Hospital from the period of January 1, 2019 to January 1, 2020. The study was approved by Ethical Committee of Arab Board of Health Specialization and University of Basrah/College of Medicine. Unfortunately, no control group was included in the study. Consent from patients was taken about the study. Causes of metabolic alkalosis due to primary or apparent mineralocorticoid excess were excluded from this study. Diagnosis of metabolic alkalosis was made by findings of high blood PH and high serum bicarbonate [HCO3-] levels. Rice broth solution was produced by mixing one cup of Basmati rice (250 mL) with six cups of water (1500 ml) to yield an approximately a one-liter solution and salt was added in a concentration of 6.5 g. The mixtures were heated until boiled then the temperature reduce to low levels for 10 minutes and left to cool. In order to overcome the lab error, 10 samples were taken from this solution and sent to the lab for PH and electrolytes measurements, mean ± SD for each electrolytes and PH were taken. Patients were received 2-3 liters of rice broth solution per day depending on the severity of hypovolemia and alkalosis and laboratory workups were done next day. Patients’ demographics including age, sex, race, body mass index, smoking and alcoholic history were documented. History of chronic diseases such as hypertension, diabetes, coronary artery disease, heart failure, cerebrovascular disease and chronic obstructive pulmonary disease was reported. Causes of metabolic alkalosis and whether the patients were in the outpatient or private sector or in the medical ward or ICU were mentioned. Patients’ volume status was assessed by heart rate (HR in BPM) and blood pressure measurement (BP in mm Hg) measurement both in supine and sitting position looking for orthostatic changes. Laboratory investigations were done before and after treatment with oral rice broth solution which included arterial blood gases (ABG) and basic metabolic panels (BMP). Both monovalent ions such as sodium [Na+] in mmol/L, potassium [K+] in mmol/L, chloride [Cl-] in mmol/L, bicarbonate [HCO3-] in mmol/L and divalent ions such as calcium [Ca+2] in mg/dL and mmol/L, phosphorus [PO4-2] in mg/dL and magnesium [Mg+2] in mg/dL were measured. Because of the concern of pseudohyponatremia due to indirect ion specific electrode (ISE) potentiometry which is used by the hospital-based laboratories, plasma [Na+] measurements using direct ion specific electrode potentiometry using the ABG were used 24. Matched serum [HCO3-] from the BMP and plasma [HCO3-] from the ABG was considered acceptable for interpretations otherwise skewed results were repeated. Because of the effect of proteins on the total serum [Ca+2] levels, ionized plasma [Ca+2] from the ABG was the utilized measurement 25. Because of the difficulty in arterial puncture in the outpatient and private clinics, venous blood gas (VBG) was done and addition of 0.04 number to the PH to have an approximate estimation of the arterial PH. The machine used for biochemical analysis was ABBOTT laboratories diagnostics Architect c 4000 made in USA and for ABG was RADIOMETER ABL800 FLEX made in USA. The PH of the solutions were measured using PH meter.
Outcome
The outcome of the study is correction of electrolytes and metabolic alkalosis.
Statistical Analysis
Continuous normally distributed variables were analyzed using means ± SDs and continuous skewed variables were analyzed using medians and interquartile ranges. Non continuous variables were analyzed using numbers and percentages. Comparisons of laboratory parameters before and after treatment with rice broth were made using paired sample T-test. Laboratory characteristics (HCO3 and K ions levels ranges) were analyzed statistically according to causes of metabolic alkalosis using Pearson Chi-Square test. P value of < 0.05 was considered statistically significant. The statistics were done using SPSS version 25.
Results
Fifty-three patients with metabolic alkalosis were studied. Table 1 illustrated the baseline demographics and clinical characteristics of the study cohort. The median age was 64, 43.4 % were males, 100 % were white, 50% were obese, 41.5% were smokers, 68% were hypertensive, 53% were diabetic, 41% had CAD and two patients had COPD. Causes of metabolic alkalosis were as follows: NG suction in 32%, vomiting in 32% and diuretics use in 30%. Fifty-three percent were in the ICU, 26% in the outpatient clinic and 21% in the medical ward. Table 2 showed the PH, electrolytes and glucose concentrations of 1liter rice broth solution. The PH was 6, the concentrations of electrolytes were as follow: [Na+] 150 mmol/L, [Cl-] 150 mmol/L, [K+] 5.2 mmol/L, [HCO3-] 0.005 mmol/L, [Ca+2] 1.8 mmol/L, [PO4-2] 0.4 mmol/L, [Mg+2] 3.2 mmol/L and glucose 0.06 g/L. Table 3 describes the lab parameters before and after treatment with 2-3 liters of rice broth solution. After treatment, the PH decreased from mean of 7.45 ± 0.03 SD to 7.4 ± 0.009, serum [HCO3-] decreased from mean of 34.5 ± 4.4 SD to 24.9 ± 1.1 SD, serum [Na+] and [Cl-] were increased from mean of 132.5 ± 3.7 SD and 93.2 ± 5.4 SD to 136.5 ± 1.9 SD and 101.9 ± 2.7 SD respectively, serum [K+] was increased from mean of 3.1 ± 0.3 SD to 3.6 ± 0.2 SD, serum [Ca+2] was increased from mean of 0.99 ± 0.1 SD to 1 +- 0.1 SD, serum [PO4-2] was increased from mean of 3.4 ± 0.5 SD to 3.6 ± 0.4 SD and serum [Mg+2] was increased from mean of 1.88 ± 0.2 SD to 2.28 ± 0.17 SD. Table 4 showed the ranges of serum [HCO3-] and [K+] according to causes of metabolic alkalosis. Both sever hypokalemia and metabolic alkalosis were in the ICU with NG suction. Diuretic use and NG suction were more common cause of metabolic alkalosis in the males while vomiting was the most common cause in the females (Figure 1). Vomiting was the most common cause of metabolic alkalosis in the outpatient clinic, diuretic use in the medical ward and NG suction in the ICU (Figure 2). NG suction was more common cause of metabolic alkalosis in the elderly, while vomiting was most common the younger age group (Figure 3). Metabolic alkalosis was more sever in the ICU (Figure 4). Vomiting was more common in lower BMI group, NG suction was more common in higher BMI groups and diuretic use was in between (Figure 5).
Table 1: Baseline Demographics and Clinical Characteristics of the Study Cohort.
| Characteristics | Overall cohort (n = 53) | |
| Age (years) | 64 (53, 69) | |
| Gender | Male | 23 (43.4) |
| Female | 30 (56.6) | |
| Body mass index kg/m2 | 30 (28, 31) | |
| Smokers | 22 (41.5) | |
| Hypertension | 36 (68) | |
| Diabetes mellitus | 28 (53) | |
| Coronary artery disease | 22 (41) | |
| Chronic obstructive pulmonary disease | 2 (4) | |
| Outpatient | 14 (26) | |
| Medical ward | 11 (21) | |
| Intensive care unit | 28 (53) | |
| Vomiting | 18 (34) | |
| Nasogastric suction | 18 (34) | |
| Diuretics | 17 (32) | |
Values are expressed in median (interquartile ranges), n (%)
Table 2: Electrolytes Concentrations and PH of the Home-Made Rice Broth Solution [250 mL Rice (1 Cup) and 1500 mL Water with addition of 6.5 Grams Salt]. Mean +- SD, n = 10.
| [Na+] mmol/L | [Cl-] mmol/L | [K+] mmol/L | [HCO3-] mmol/L | [Ca+2] mmol/L | [PO4-2] mmol/L | [Mg+2] mmol/L | Glucose g/L | PH |
| 150 ± 1 | 150 ± 1 | 5.2 ± 0.2 | 0.005 ± 0.0 | 1.8 ± 0.1 | 0.4 ± 0.1 | 3.2 ± 0.1 | 0.06 ± 0.01 | 6 |
Values are expressed as mean ± SDs.
Table 3: Comparisons of the Laboratory Values Before and After Treatment with 2-3 Liters per Day of Rice Broth Solutions. n = 53.
| Lab values | Before treatment | After treatment | P-value |
| PH | 7.45 ± 0.03 | 7.4 ± 0.008 | <0.001 |
| PCO2 mm Hg | 45.4 ± 3 | 40.7 ± 1.5 | <0.001 |
| [HCO3-] mmol/L | 34.5 ± 4.4 | 24.8 ± 1.1 | <0.001 |
| [Na+] mmol/L | 132.5 ± 3.6 | 136.5 ±1.9 | <0.001 |
| [Cl-] mmol/L | 93.2 ± 5.4 | 101.9 ± 2.7 | <0.001 |
| [K+] mmol/L | 3.1 ± 0.3 | 3.6 ± 0.2 | <0.001 |
| [Ca+2] mmol/L | 0.99 ± 0.1 | 1 ± 0.1 | <0.001 |
| [PO4-2] mg/dL | 3.4 ± 0.5 | 3.6 ± 0.4 | <0.001 |
| [Mg+2] mg/dL | 1.88 ± 0.2 | 2.28 ± 0.2 | <0.001 |
Vales are expressed as mean ± SDs.
PH, potential of hydrogen; PCO2, partial pressure of carbon dioxide; HCO3, bicarbonate ions; Na, sodium ions; Cl, chloride ions; K, potassium ions; Ca; calcium ions; PO4, phosphorus ions; Mg, magnesium ions.
Correlations were made using paired sample T test.
Table 4: Laboratory Characteristics (HCO3 and K) According to Causes of Metabolic Alkalosis. N = 53.
| Lab Characteristic | Vomiting | NG suction | Diuretic | P value |
| HCO3 24-34 mmol/L | 15 (83.3) | 4 (22.2%) | 11 (64.7) | 0.001 |
| HCO3 > 34 mmol/L | 3 (16.7) | 14 (77.8) | 6 (35.3) | 0.001 |
| K 3-3.5 mmol/L | 16 (88.9) | 10 (55.6) | 13 (76.5) | 0.072 |
| K < 3 mmol/L | 2 (11.1) | 8 (44.4) | 4 (23.5) | 0.072 |
Values are expressed as n (%).
HCO3, bicarbonate ions; K, potassium ions; NG, nasogastric.
Correlation were made using Pearson Chi-Square test.
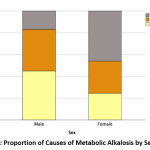 |
Figure 1: Proportion of Causes of Metabolic Alkalosis by Sex Status. |
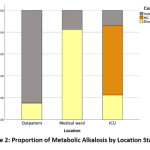 |
Figure 2: Proportion of Metabolic Alkalosis by Location Status. |
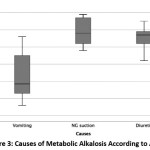 |
Figure 3: Causes of Metabolic Alkalosis According to Age. |
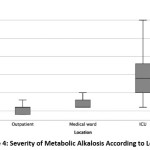 |
Figure 4: Severity of Metabolic Alkalosis According to Location. |
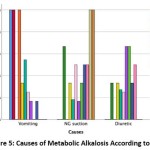 |
Figure 5: Causes of Metabolic Alkalosis According to BMI. |
Discussion
Unfortunately, no previous similar studies for comparisons. Treatment of metabolic alkalosis with volume contraction, hypochloremia and hypokalemia include intravenous administration of 3-5 liters of 0.9% isotonic saline which contains 154 mmol/L [Na+] and 154 mmol/L [Cl-] with addition of 20 mmol/L potassium chloride to the administered fluid. This form of therapy is given by intravenous route so it is need hospital admission and may cause volume overload in patients with heart failure or renal failure. In the present study, the majority of patients were older and had multiple chronic diseases which means they may have systolic or diastolic dysfunction and baseline renal dysfunction which make them vulnerable to complications of isotonic saline. Also, isotonic saline may be associated with an increase incidence of acute kidney injury 26. One liter of rice broth solution contains [Na+] and [Cl-] concentrations which are similar to 1 liter of 0.9% saline solution. It also contains [K+] in concentrations of 5.2 mmol/L and [Mg+2] in concentrations of 3.2 mmol/L which may help in cases of metabolic alkalosis with hypokalemia and hypomagnesemia such as in diuretics use. The rice broth solution is given by mouth and it is palatable with no any adverse effects observed compared to isotonic saline. Other options for treatment of metabolic alkalosis include hydrochloric acid, ammonium chloride and acetazolamide. Hydrochloric acid should be given in the ICU through carefully placed, free-flowing central venous catheter into the superior vena cava; It should be given in a glass container and the tubing should be changed every 12 hours 27. Ammonium chloride should also be given by intravenous route but, it metabolizes to urea, so it is contraindicated in patients with renal or liver failure. Acetazolamide is an oral form of therapy but, it can cause significant hypokalemia.
The study had some limitations. First, it is not randomized controlled trial to compare rice broth with isotonic saline and placebo. Second, more samples of rice broth are required to know the accurate concentrations of the electrolytes.
Conclusions
Rice broth solution is an effective and safe solution for treatment of metabolic alkalosis. It is an easy recipe to be done, it is palatable with no noted adverse effects.
Acknowledgments
We acknowledge the laboratory team who help us in doing the laboratory paramters of our study.
Conflict of Interest
There is no conflict of interest for all authors.
Funding Source
No funding for this work.
References
- Hodgkin JE, Soeprono FF, Chan DM. Incidence of metabolic alkalemia in hospitalized patients. Crit Care Med. 1980;8(12):725-8.
CrossRef - Anderson LE, Henrich WL. Alkalemia-associated morbidity and mortality in medical and surgical patients. South Med J. 1987;80(6):729-33.
CrossRef - Seldin DW, Rector FC. The generation and maintenance of metabolic alkalosis. Kidney International. 1972;1(5):306-21.
CrossRef - Babior BM. Villous adenoma of the colon. Study of a patient with severe fluid and electrolyte disturbances. Am J Med. 1966;41(4):615-21.
- Hoglund P, Haila S, Socha J, Tomaszewski L, Saarialho-Kere U, Karjalainen-Lindsberg ML, et al. Mutations of the Down-regulated in adenoma (DRA) gene cause congenital chloride diarrhoea. Nat Genet. 1996;14(3):316-9.
CrossRef - Ellison DH. The physiologic basis of diuretic synergism: its role in treating diuretic resistance. Ann Intern Med. 1991;114(10):886-94.
CrossRef - Pedroli G, Liechti-Gallati S, Mauri S, Birrer P, Kraemer R, Foletti-Jaggi C, et al. Chronic metabolic alkalosis: not uncommon in young children with severe cystic fibrosis. Am J Nephrol. 1995;15(3):245-50.
CrossRef - Kassirer JP, Schwartz WB. Correction of metabolic alkalosis in man without repair of potassium deficiency. A re-evaluation of the role of potassium. Am J Med. 1966;40(1):19-26.
- Jones JW, Sebastian A, Hulter HN, Schambelan M, Sutton JM, Biglieri EG. Systemic and renal acid-base effects of chronic dietary potassium depletion in humans. Kidney International. 1982;21(2):402-10.
CrossRef - Cannon PJ, Ames RP, Laragh JH. Relation between potassium balance and aldosterone secretion in normal subjects and in patients with hypertensive or renal tubular disease. The Journal of clinical investigation. 1966;45(6):865-79.
CrossRef - Nakamura S, Amlal H, Galla JH, Soleimani M. NH<sub>4</sub><sup>+</sup> secretion in inner medullary collecting duct in potassium deprivation: Role of colonic H<sup>+</sup>-K<sup>+</sup>-ATPase. Kidney International. 1999;56(6):2160-7.
CrossRef - Hernandez RE, Schambelan M, Cogan MG, Colman J, Morris RC, Jr., Sebastian A. Dietary NaCl determines severity of potassium depletion-induced metabolic alkalosis. Kidney Int. 1987;31(6):1356-67.
CrossRef - Sabatini S. The cellular basis of metabolic alkalosis. Kidney International. 1996;49(3):906-17.
CrossRef - Luke RG, Levitin H. Impaired renal conservation of chloride and the acid-base changes associated with potassium depletion in the rat. Clin Sci. 1967;32(3):511-26.
- Amlal H, Wang Z, Soleimani M. Potassium depletion downregulates chloride-absorbing transporters in rat kidney. The Journal of clinical investigation. 1998;101(5):1045-54.
CrossRef - Adrogue HJ, Madias NE. Management of life-threatening acid-base disorders. Second of two parts. N Engl J Med. 1998;338(2):107-11.
- Sherman RA, Eisinger RP. The use (and misuse) of urinary sodium and chloride measurements. Jama. 1982;247(22):3121-4.
CrossRef - Kassirer JP, Berkman PM, Lawrenz DR, Schwartz WB. The critical role of chloride in the correction of hypokalemic alkalosis in man. The American Journal of Medicine. 1965;38(2):172-89.
CrossRef - Rosen RA, Julian BA, Dubovsky EV, Galla JH, Luke RG. On the mechanism by which chloride corrects metabolic alkalosis in man. The American journal of medicine. 1988;84(3 Pt 1):449-58.
- Worthley LIG. Intravenous Hydrochloric Acid in Patients With Metabolic Alkalosis and Hypercapnia. Archives of Surgery. 1986;121(10):1195-8.
CrossRef - Finkle D, Dean RE. Buffered hydrochloric acid: a modern method of treating metabolic alkalosis. Am Surg. 1981;47(3):103-6.
- Warren SE, Swerdlin AR, Steinberg SM. Treatment of alkalosis with ammonium chloride: a case report. Clin Pharmacol Ther. 1979;25(5 Pt 1):624-7.
- Preisig PA, Toto RD, Alpern RJ. Carbonic Anhydrase Inhibitors. Kidney and Blood Pressure Research. 1987;10(3-4):136-59.
- Kim G-H. Pseudohyponatremia: does it matter in current clinical practice? Electrolyte Blood Press. 2006;4(2):77-82.
CrossRef - Hu Z-D, Huang Y-L, Wang M-Y, Hu G-J-L, Han Y-Q. Predictive accuracy of serum total calcium for both critically high and critically low ionized calcium in critical illness. J Clin Lab Anal. 2018;32(9):e22589-e.
- Palevsky PM. Intravenous Fluids. Finding the Right Balance. 2018;13(12):1912-4.
CrossRef - Beach FX, Jones ES. Metabolic alkalosis treated with intravenous hydrochloric acid. Postgrad Med J. 1971;47(549):516-20.
CrossRef
Accepted on: 23 July 2021
Second Review by: Dr. Kirti Bhati India
Final Approval by: Dr. Norazmir Md Nor





Web of Science Coverage
Emerging Sources Citation Index (ESCI)
2024 Journal Impact Factor: 1.1
Scopus Journal Metrics
CiteScore 2025: 2.6
CiteScore Details
Sustainable Nutrition: Food Systems, Nutrient Retention, and Public Health Impact
![]()
This journal is a member of, and subscribes to the principles of, the Committee on Publication Ethics (COPE)








