Impact of a Nutritional Intervention Based on Amaranth Flour Consumption to Recovery Undernourished Children
Wendy Margarita López-Alonso1
, Jaime Reyes-Hernández2* 1Department of Public Health, Faculty of Nursing and Nutrition, Universidad Autónoma de San Luis Potosí, S.L.P. México.
2Department of Food Science, Faculty of Nursing and Nutrition, Universidad Autónoma de San Luis Potosí, S.L.P. México.
Corresponding Author Email: reyes.jaimeh@uaslp.mx
DOI : http://dx.doi.org/10.12944/CRNFSJ.9.1.22
Download this article as:
![]()
Amaranth flour (AF) can be used as an alternative for nutritional recovery, however, there is not enough evidence on the efficacy of these types of programs. The objective of this study was to assess the effect of an Integral Nutritional Recovery Program (INRP) with AF as complementary feeding on anthropometry in children with grade 1 malnutrition. A quantitative before-after study with intervention and follow up was developed. Dyads of caregiver and grade one malnourished children were evaluated (Control group n=37 and experimental group n=46). A supplement based on amaranth flour were given to Control group (CG) and Experimental Group (EG), only EG received the intervention IPNR. Variables evaluated were weight/height (W/H), muscle mass (MM), fat mass (FM), arm circumference (AC), head circumference (HC), triceps skinfold (TRSF), subscapular skinfold (SSF), body mass index (BMI), subscapular/triceps index (SS/TR), and centripetal index (CI). Data were analyzed using ANOVA, orthogonal arrangements, and paired-T test, 95% CI, significance p≤0.05. Initial anthropometric evaluation showed that the conformation of the CG and EG was homogeneous (p ≥ 0.05). After three months of follow up height and HC showed no differences (p ≥ 0.05). In contrast, W/H, AC, SSF, TRSF, BMI, and FM increased in different magnitudes in function of time for both groups. Paired analysis indicated higher increases in EG than CG. Subscapular/triceps index decreased, and MM showed a tendency to increase (p ≤ 0.1). No significant differences were observed between males and females, height and HC (p ≥ 0.05). Integral Nutritional Recovery Program was effective in improving nutritional status of experimental group and continuing for three months. A follow up is recommended after six months to verify nutritional recovery.
KEYWORDS:Amaranth Flour; Intervention; Malnutrition; Nutritional Recovery Program
Introduction
According with WHO nutritional deficiencies is among the first 10 causes of mortality in children under nine years of age.1-3 In Latin America and the Caribbean, malnutrition of children under five years of age is part of the double burden of malnutrition.1-3 Economic Commission for Latin America and the Caribbean reports that since the 1990s to the decade of 2010, Mexico reduced chronic malnutrition by over 60%.1,2 However, it is also true that in the last three years there has been a rebound in the Hunger index, undernourishment is close to 7% in the Region.3 Data of 2017 indicate that in San Luis Potosí State, mild malnutrition is cause of morbidity in children from one to four years of age with a rate of 1261 per 100,000 inhabitants.4 Thus, it is clear that it continues being a serious public health problem.1,4
Malnutrition commonly associated to food deficiencies causes retarded growth in children and affects psychosocial development and school performance with catastrophic consequences in the occupational trajectory and economic income, produces greater poverty.1,3,5 These conditions are inherited to next generations; poverty favors the vicious circle because it increases disease and risk of death. In addition to the risk of chronic communicable and non-communicable diseases in adulthood, which is why the WHO insists on investing in childhood health.5
To reduce the number of children with malnutrition, federal and state public health institutions in Mexico have implemented food support programs for over 40 years. These types of programs providing breakfasts, supplements to prepare porridge, multivitamins, milk and, recently at state level, this has included the program consisting in the distribution of amaranth flour began as a pilot plan in the state of San Luis Potosí and was the first in its class. Although the nutritional quality of amaranth has been well documented,6 there is still little evidence on the use of amaranth flour in nutritional recovery programs of children with malnutrition.7 Generating scientific evidence on the efficacy of these types of programs based on local foods can help to establish new alternatives for nutritional recovery, given that it has been demonstrated that they help to increase anthropometric variables,7 and because of their economic viability.8 However, by themselves, programs supplying food supplements are not sufficient because malnutrition is a multi-factor problem that involves behavioral aspects, habits, and customs of the principal players, in response we design, an Integrating Nutritional Recovery Program (INRP) focused in three axis: a) delivering local food, b) modifying knowledge, basic health skills and behaviors of the principal players, like primary caregivers (PC), children, and health providers (HP). INRP focused in the PC, because in the perspective of the Mexican population, nutritional prevention aspects should have programs with multiple levels of influence and it is desirable to construct nutritionally a healthy environment in the home, especially from early age because childhood is the ideal moment to intervene in habits.5,9,10 Another fundamental axis is the training of HP, who must have knowledge to allow them to provide adequate accompaniment to the families, given that they are responsible for evaluating, educating, and monitoring the child’s nutritional recovery. If the three pillars were integrated into current programs in the fight against malnutrition, the effectiveness of these programs could be improved. This study sought to evaluate the effect of an INRP with amaranth flour as complementary feeding on anthropometry in children with grade 1 malnutrition.
Methods
Design
A quantitative before-after study with intervention and follow up was performed. For to assess the anthropometric effect of an Integral Nutritional Recovery Program (INRP) two groups were set up; an experimental group (EG) and a control group (CG). An intervention (IPNR) based on controlled consumption of amaranth flour in an experimental group (EG) was applied. Meanwhile, the control group (CG) was given a supplement based on amaranth flour without intervention. This study was carried out from November 2010 to February 2011.
Sample
The initial recruitment of malnourished grade 1 children was acquired of the Ministry of Health of the State of San Luis Potosí. Target population (n= 240) was identified in the nutritional control census that met the inclusion criteria: PC and children between two and four years of age from masculine and feminine genders with grade 1 malnutrition, receiving amaranth as a food supplement. After the briefing about the study and its ethical implications, 123 PC accepted to participate and signed the informed consent. Forty-eight children were not located so they were excluded; additionally, 40 children were lost to follow up. The final sample of the EG had 46 children, while CG had 37 children. Both EG and CG were classified as grade 1 malnutrition, according to weight for height (W/H) appointed to the INRP, which had nutritional control after three months.
Study Variables
The independent variable consisted of the educational intervention of three main ideas: a) supply of an amaranth flour supplement, controlling consumption during the follow up to the EG. The CG also received the amaranth flour according to the usual procedure in health centers. To obtain accuracy in the doses that would be supplied in children, packages with 15 g amaranth flour (recommended daily dose) were made, weighed on a calibrated scale for exact weight, giving the EG the 20 bags that they should consume during the period before the next measurement. b) PC or maternal training. The contents of the orientation to the PC include nutrition, correct diet, and amaranth flour preparation. c) Accompaniment of PC by HP (community personnel of the SSA-SLP, and community health promoters) trained based on the 2007 State Nutrition Program and its strategies of supplementation with amaranth flour, as well as communication processes and filling in the corresponding records and anthropometry through a workshop, as observed in Table 1.11 Dependent variables assessed were: weight/ Height (W/H), muscle mass (MM), fat mass (FM), arm circumference (AC), head circumference (HC), triceps skinfold (TRSF), subscapular skinfold (SSF), body mass index (BMI), subscapular/triceps index (SS/TR), and centripetal index (CI).
Instruments
Mechanical scale 700 with a Seca 220 Stadiometer (SECA Gmbh & Co., Hamburg, Germany), Skinfold Compass: Body Caliper What are you made of? (The Caliper Co. Inc-2533, Carson City, USA, Exclusive Patented AccSpringTM), Consumption Control register, Record of Consumption follow up, and W/H WHO tables.
Table 1: Training Aimed at Health Providers and Primary Caregivers of Children from 2 to 4 Years of Age with Grade I Malnutrition.
| Sessions | 1 (2h) | 2 (2h) | Didactic Strategy |
| Caregivers | -Nutritional needs of children from 2 to 4 years of age.-Characteristics and consequences of malnutrition-Nutritional requirements and correct diet.* | -Benefits of the amaranth flour supplement.-Preparation of amaranth flour and its introduction in the diet of children.-Fill out the form to register the daily consumption of amaranth flour by children. | -Evaluation of previous knowledge.-Slides.-Group discussion.-Demonstration and feedback from the health provider to prepare amaranth flour.-Agree-Disagree with brief statements about nutritional recovery and reflect on the cost-benefit balance of healthy nutritional behavior with the introduction of amaranth flour.-Closure and evaluation of new knowledge. |
| Health providers | Characteristics and consequences of malnutrition and nutritional needs of children from 2 to 4 years of age.-Correct nutrition. *-Benefits of the amaranth flour supplement.-Preparation of amaranth flour and its introduction in the diet of children. | -Interpersonal communication, motivation and persuasion.-Ethical bases of therapeutic intervention.-Systematic organization of health actions.-Filling out the record format of health providers to monitor the consumption of amaranth flour by children (frequency, dose, schedule, preparation form, and incidents). | -Evaluation of previous knowledge.-Slides.-Group discussion.-Feedback from the main researcher for the preparation of amaranth flour.-Feedback from the main researcher to fill in the amaranth flour consumption monitoring form. |
*Good feeding plate, Mexican Official Standard (Plato del Bien Comer, Norma Oficial Mexicana NOM-043-SSA2-2005, Servicios básicos de salud. Promoción y educación para la salud en materia alimentaria. Criterios para brindar orientación). https://www.salud.gob.mx/Unidades/cdi/nom/compi/043ssa205.pdf
Procedures for Data Collection
The PC and their children from the EG and CG attended the anthropometric measurements of the children and the diagnosis of the baseline nutritional status and follow up in the health centers. The nutritional diagnosis was made based on the Geneva tables, accepted by WHO, according to the Mexican Official Standard (NOM-031-SSA2-1999) to care for the health of children.12 The W/H index was used due to its sensitivity and specificity for nutritional diagnosis in children under five years of age.13 The educational and assessment program was implemented with the EG in the health centers and through home visits. Dependent variables were evaluated every 20 days until completing five measurements by the third month post-intervention. The personnel were assigned the children to whom the home visits should be made to verify consumption of amaranth flour and to carry out the registration; in addition, the promoters randomly monitored the children’s homes to verify consumption.
Statistical Analysis
The data were captured and processed by using STATISTIC V 7.1 (StatSoft Inc., Tulsa, OK). Analysis of data from the first or baseline stage consisted in evaluating the homogeneity of the groups. The second stage evaluated changes in anthropometric measurements every 20 days during the three-month follow up. The last stage conducted a paired analysis of the baseline measurements versus the final ones. Descriptive statistics, like frequencies, percentages, measures of central tendency and dispersion, mean differences in scores before and after the training with ANOVA (evaluation of gender and group), orthogonal arrangements, Student’s t test, and paired sample T test for independent and related samples were used (95% CI, p ≤ 0.05).
Ethical Aspects
The present study was supported by the general approval of the State Bioethics and Health Research Committee of the Ministry of Health (SSA) to the Project: Nutrition in Vulnerable Population: Preschool, number 24.10. The study was based on guidelines established by the Helsinki Declaration of the World Medical Association, in the General Health Legislation of Mexico, fifth title, sole chapter, article 100, referring to research on human beings, sections III and IV, Health Legislation of the State of San Luis Potosí, article 84, sections III and IV. Given that the study sample was made up of children treated in health centers, it was anticipated that the caregiver, after the explanation of the study and the right to participate or not in the research and to withdraw their consent at any time, without exposing themselves to retaliation, sign or place their fingerprint in an informed consent format to endorse the approval for the child’s participation.
Results
For this research, the CG was given a supplement based on amaranth flour for consumption by children with malnutrition, while the EG received an IPNR. The results showed an EG made up of 46 minors, 29 of female sex and 17 of male sex, with mean age of 3 years and 4 months. The CG was comprised of 37 children; 20 were of female sex and 17 of male sex, with a mean age of 3 years and 1 month. The gender analysis showed no significant differences between males and females after six evaluations (p ≥ 0.05).
Initial Homogeneity of the Experimental and Control Groups
Conformation of the groups was homogeneous, the results of the initial anthropometric evaluation (Ev1) of the control group (CG1) and (EG1) showed no significant differences in weight, height, MM, SSF, SS/TR index, CI, HC and AC (p ≥ 0.05) (Table 2). Only three variables were significant: TRSF, BMI, and FM (p ≤ 0.05).
Follow up of the Evaluation of the Nutritional State
After three months of follow up, height and HC showed no differences among evaluations or between both groups evaluated (p ≥ 0.05). In contrast, parameters, like weight, AC, SSF, TRSF, BMI, MM, and FM showed an increase in different magnitudes in function of time for both groups. The SS/TR index had a descending behavior. Regarding the weight variable, the average values showed increments in function of time in both groups, but higher in EG, compared with CG (figure 1 A). The paired analysis indicated significance in the EG compared with the CG (figure 1 A´). The EG went from 11.9 ± 2.3 kg in the first evaluation to 13.0 ± 2.4 kg in the final (p ≤ 0.05). In contrast, the CG showed no significant increments (p ≥ 0.05).
 |
Table 2: Nutritional Assessment of Undernourished Mild Children through Anthropometrics Parameter in a Control Group without Intervention and an Experimental Group with Intervention. |
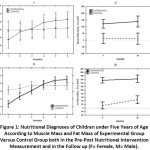 |
Figure 1: Nutritional Diagnoses of Children under Five Years of Age According to Muscle Mass and Fat Mass of Experimental Group Versus Control Group both in the Pre-Post Nutritional Intervention Measurement and in the Follow up (F= Female, M= Male). |
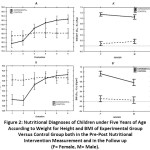 |
Figure 2: Nutritional Diagnoses of Children under Five Years of Age According to Weight for Height and BMI of Experimental Group Versus Control Group both in the Pre-Post Nutritional Intervention Measurement and in the Follow up (F= Female, M= Male). |
Muscle Mass, Fat Mass, and Body Mass Index
For the MM case, it was observed that although the EG showed a growing behavior during the six evaluations, none was significant (p ³ 0.05); however, the trend suggests that an additional evaluation could end up being significant (the comparison between EV1 and EV6 for the EG had p = 0.082). In the CG, the MM behavior over time remained constant from EV1 to EV6, without statistical significance in any evaluation. The EG showed ascending behavior of FM during the six evaluations, with significance only in the difference between EV1 and EV6 (p £ 0.05). Not so for the CG where no significance existed in any evaluation. The paired analysis indicated increased FM and a significant difference between the EG and CG, with this increase being higher for the EG. In turn, the BMI of the EG increased in function of time, while the values of the CG remained constant. Although in the final measurement no differences were observed between the EG and CG, the paired analysis revealed a clear increase in the CG (figure 2). The increment of BMI values of the EG were significance between measurements EV3 ¹ EV4 and EV1 ¹ EV6 (p ≤ 0.05). For the CG, no significant differences were noted. Finally, the gender analysis was not a determinant factor in the results; there was no statistical significance for the BMI, MM, and FM variables since the start of the research (figure 1; A´,B´ and figure 2; C´, D´).
Triceps Skinfold, Subscapular Skinfold, and Arm Circumference
A behavior similar to weight was observed in the TRSF. No differences were noted between the EG and CG in the final evaluation (EV6), however, the paired analysis showed that the EG had a significant increase after three months; no so for the CG (Table 2). For SSF, the comparison between the sixth and first measurement was significant for both groups, with this difference being higher in the EG (p ≤ 0.05). Increased SSF in the EG had significant differences in measurements EV3 ¹ EV4 and EV4 ¹ EV5 (p ≤ 0.05) (Table 2). For the CG, the differences were in evaluations EV3 ¹ EV4 and EV1 ¹ EV6 (p ≤ 0.05). The other evaluations had no significant differences among them and between groups. The paired analysis for the AC only showed differences between the evaluations EV1 and EV6 for the EG. For the CG, no differences were observed in any of the six evaluations conducted (p ≥ 0.05).
Subscapular/Triceps Index and Centripetal Index
In both groups, the SS/TR index showed descending behavior throughout the six measurements. Differences were only observed between evaluations EV1 and EV6 in the CG and the EG (p ≤ 0.05). The comparison between the EG and CG through the paired analysis showed differences, the SS/TR index values were higher for the CG (p £ 0.05). Moreover, the centripetal index – in spite of showing an ascending behavior – showed no statistical significance in any evaluation or between the groups (p ³ 0.05).
Discussion
Anthropometric Evaluation
IPNR was the principal factor influencing on the recovery differences observed, but height and HC were not sensitive to IPNR after three months, low height is associated with chronic malnutrition and its recovery requires long periods when it can be recovered,14,15 and the importance of HC is its correlation with brain size, both, height and HC depend of variables like the type of malnutrition, hormonal, catch up growth and genetic variables.15,16-19 However, some of these parameters could have nutritional progress if the programs were extended enough time to see significant changes (e.g., one year). With acute malnutrition, some anthropometric variables may be more sensitive to nutritional changes in short time periods. This study, and for both groups, observed changes in TRSF, SSF, SS/TR, which estimated the body fat percentage; AC, variable commonly used to estimate malnutrition in the community, BMI, and FM; 20,21 a higher number of variables with statistical significance was observed in the EG compared with the CG (p £ 0.05), similarly to another intervention with amaranth flour.7 The aforementioned suggests that controlled intake of amaranth flour, with care protocols and follow up can be efficient and favor faster nutritional recovery of malnourished children.
Of the variables observed, with statistical significance, W/H and W/A are of greatest use to diagnose the nutritional state of the children, but BMI, which is the most frequently used epidemiologically, not is the most accurate estimate of adiposity,20,22 an increase in these variables does not necessarily mean nutritional improvement in the children, given that increased weight does not necessarily translate into increased lean mass but an increase in body fat. Increased FM and MM must take place in adequate proportion for it to be healthy to the children.23 This is why an adequate selection and interpretation of nutritional variables is of vital importance. In this study, the EG gained weight, FM, and MM, this last – although not significant (p ≥ 0.086) – suggests that with one or two additional evaluations its significance would have been positive due to the trend observed. Instead, for the CG the muscle content remained constant, as well as the fat content, during all the evaluations. The increased FM observed in EG was not considered a malnutrition problem, given that besides the MM increase, parameters, like SS/TR index and CI, suggest better distribution of fat on the trunk and limbs in the EG compared with the CG. A value > 1 on the SS/TR index indicates that fat is mostly distributed on the body trunk, while a value ≤ 1 indicates that the fat is distributed in the body’s peripheral zones. Something similar occurs with the CI where the values of the EG indicate lower fat distribution on the trunk.17, 20, 23 Thereby, the IPNR improved the anthropometric parameters of the children and it was reflected in increased weight, MM, and FM and diminished SS/TR index and CI. This implies, in the long term, lower risk of chronic diseases, like diabetes, obesity, or of suffering metabolic syndrome.5
Nutritional recovery intervention program. As already mentioned, the CG only received the supplement as done normally and follow up was conducted every 20 days as with the EG. The IPNR proposed for the EG revolved around three fundamental axes; the PC, the HP, and the delivery and the child’s consumption of a food supplement based on amaranth flour. Given the age of the child with malnutrition (2-4 years), the PC is the principal person responsible for the child’s feeding, thus, the program was focused strongly on training the PC, defined into three stages; awareness of the childhood malnutrition problem, correct feeding, and constant motivation of the PC. The results suggest that the intervention permitted greater participation from the PC in the child’s feeding processes. Generation of awareness on caring for the child, which although already existing, upon integrating information based on clinical evidence, elimination of myths and wrong information, favored more active, self-sufficient, and satisfactory participation by the PC. Additionally, the generation of short-term objectives and goals permitted sustainable improvement throughout the program, generating self-motivation in PC that was transmitted to the children. HP are fundamental for the program’s success, given that besides the knowledge they provide during the training of the PC, they are responsible for evaluating the child’s nutritional state, monitoring, and maintaining the PC motivated through home visits, strategy that has shown its usefulness.24 Commitment by the HP is the base for the IPNR to be more effective. Within the context in which families have a child with malnutrition, the PC visualizes the HP as a figure of authority by coming from a governmental health institution. This generates a change in behavior in the PC when they are given food support, similar to what happens when they go to a medical consultation where commitment with the doctor is generated and adherence to treatment, however, is reduced when the interaction between the HP and the PC is superfluous, which may be associated with lack of training of the HP, lack of interest, excess number of patients, among other factors. The HP need more strategies to improve the nutritional education.25 The foregoing causes the PC to abandon treatment or apparent compliance with the program. At the same time, when the PC is not conscious of the risks and consequences of malnutrition in children, interest is lost more rapidly in the recovery process.26 Therein the importance of constant training that involves improved skills and competencies of the HP. This has directly repercussions in the nutrition recovery process of children. In this sense, the CG showed a general blockage in the nutritional recovery of the children, consequently they had a minimum recovery progress. The aforementioned was a reflection of poor interest by the PC, low frequency of consumption and/or bad management of the food supplement. The supplement provided often ended up being used for consumption by other members of the family, and, in other cases, the children consumed the supplement but not with the correct frequency, similarly to results reported in other kinds of supplementation, in this cases the chances of recovery diminish to 50%.26, 27 The behavior of the CG was associated with low co-responsibility by the PC in the child’s nutritional recovery, transferring most of the responsibility to the government’s health system (Ministry of Health; SSA-SLP).27 The limitations of this study were related to reduced follow-up, it is recommended to follow up at least six months to verify changes in the parameters as MM and in the adherence to the treatment.1,28
Conclusions and Clinical Implications
The poor knowledge of the problem of malnutrition, low PC co-responsibility, deficient accompaniment, and a nutritional/caloric deficit due to low frequency of supplement consumption generated stagnated nutritional recovery of the children. In turn, the PC in the group applying IPNR seem to have acquired greater awareness of the problem of malnutrition and its consequences, given that consumption and frequency were as indicated. When the HP are better prepared, they improve empowerment of the PC in caring for their children’s health.26 In addition, an attitude was developed of co-responsibility with governmental health institutions (Ministry of Health; SSA-SLP). These small differences in attitude and behavior generated important changes in the anthropometric parameters, especially in EG.
Acknowledgments
Consejo Potosino de Ciencia y Tecnología (COPOCYT), Ministry of Education and Ministry of Education of San Luis Potosí.
Funding Sources
The investigation was supported by grants FOMIX-2013 Consejo Potosino de Ciencia y Tecnología (COPOCYT), FMSLP-2013-C02-208475 and “Promote Educational Innovation and Social Responsibility of the Faculty of Nursing and Nutrition, P / PROFEXCE 2020-24MSU0011E-10” for the publication of research results.
Conflict of Interest
The authors declare no conflict of interest.
References
- Fernández A, Martínez R, Carrasco I, Palma A. Impacto social y económico de la doble carga de la malnutrición. Modelo de análisis y estudio piloto en Chile, Ecuador y México. 2017. Naciones Unidas/CEPAL/Programa Mundial de Alimentos (WFP). www.cepal.org.
- Shamah Levy T, Vielma-Orozco E, Heredia-Hernández O, Romero-Martínez M, Mojica-Cuevas J, Cuevas-Nassu L, Santaella-Castell JA, Rivera-Dommarco J. National Health and Nutrition Survey 2018-19. National Results. Cuernavaca, México: Instituto Nacional de Salud Pública. 2020. https://ensanut.insp.mx/encuestas/ensanut2018/doctos/informes/ensanut_2018_informe_final.pdf
- FAO, FIDA, OMS, PMA y UNICEF. 2019. El estado de la seguridad alimentaria y la nutrición en el mundo 2019. Protegerse frente a la desaceleración y el debilitamiento de la economía. Roma, FAO. ISBN 978925131600-9. http://www.fao.org/publications/es
- Diagnóstico sectorial de salud en San Luis Potosí 2018. www.slpsalud.gob.mx/transparenciaadmon/transparencia/2019/ene/DiagnosticoSalud/DIAGNOSTICO-SALUD.pdf
- Lancet Commisions. A future for the world´s children? A WHO-UNICEF-Lancet Commisions. Lancet. 2020;395:605-658. https://doi.org/10.1016/S0140-6736(19)32540-1
CrossRef - Algara-Suárez P, Gallegos-Martínez J, Reyes-Hernández J. Amaranth: Effects on nutrition and health. Revista Académica de Investigación Tlatemoani. Grupo Eumed-Universidad de Málaga, España, Universidad Autónoma de San Luis Potosí, México. Abril 2013; 9:1-21. www.eumed.net/rev/tlatemoani/12/rhgm.pdf.
- Vértiz-Cardona A, Gallegos-Martínez J, Reyes-Hernández J. An intervention based on self-efficacy and parenting competence to help recovery childhood malnutrition. Journal of Nursing Education and Practice, 2019; 9(11):107-113. https://doi.org/10.5430/jnep.v9n11p107.
CrossRef - Azimi F, Esmaillzadeh A, Alipoor E, Moslemi M, Yaseri M, Hosseinzadeh-Attar MJ. Effect of a newly developed ready-to-use supplementary food on growth indicators in children with mild to moderate malnutrition. Public Health. 2020; 185: 290-297.
CrossRef - Stang J, Bonilla Z. Factors affecting nutrition and physical activity behaviors of Hispanic families with young children: implications for obesity policies and programs. J Nutr Educ Behav. 2018; 50(10):959-967. https://doi.org/10.1016/j.jneb.2017.08.005.
CrossRef - Ontai LL, Sutter C, Sitnick S, Shilts MK, Townsend M. Parent food-related behaviors and family-based dietary and activity environment: associations with BMI z-scores in low-income preschoolers. Childhood Obesity. 2020;16(S1):S55-S63. https://doi.org/19.1089/chi.2019.0105.
CrossRef - Health Ministry (Secretaría de Salud de San Luis Potosí). State Nutrition Program. 2007.
- Galván M, Amigo H. Programas destinados a disminuir la desnutrición crónica. Una revisión en América Latina. Archivos Latinoamericanos de Nutrición. 2007; 57(4): 316 – 326. http://www.bvsde.paho.org/texcom/nutricion/programas.pdf.
- Barquera S, Rivera-Dommarco J, Gasca-García A. Políticas y programas de alimentación en México. Salud Pública Méx 2001; 43: 464 – 477.
CrossRef - Stobaugh HC, Rogers BL, Rosenberg IH, Webb P, Maleta KM, Manary MJ, Trehan I. Children with poor linear growth are at risk for repeated relapse to wasting after recovery from moderate acute malnutrition. J Nutr 2018;148:974–979. https://doi.org/10.1093/jn/nxy033.
CrossRef - Nabwera HM, Bernstein RM, Agbla SC, Moore SE, Darboe MK, Colley M, Jallow AT, Bradbury R, Karafin J, Fulford AJ, Prentice AM. Predicting undernutrition at age 2 years with early attained weight and length compared with weight and length velocity. Journal of Tropical Pediatrics, 2018, 64, 364–372. https://10.1093/tropej/fmx075.
CrossRef - Ivanovic DM, Leiva BP, Pérez HT, Almagia AF, Toro TD, Urrutia MSC, Inzunza NB, Bosch EO. Nutritional status, brain development and scholastic achievement of Chilean high-school graduates from high and low intellectual quotient and socio-economic status. British Journal of Nutrition. 2002; 87: 81–92. https://10.1079/BJN2001485.
CrossRef - Vega FL, Iñárritu PM, Robles MB. Rate of growth in children recovering from malnutrition. Rev Mex Ped 2006; 72(6): 268 – 271.
- Gotthelf SJ, Jubany LL. Evolución del perímetro cefálico en niños desnutridos de najo nivel socieconómico durante el tratamiento de recuperación nutricional. Argent. Pediatr. 2002; 100 (3): 204-209. https://www.sap.org.ar/docs/archivos/2002/arch02-3/204.pdf.
- Weisstaub SG, Araya QM. Catch up growth. An unresolved challenge. Rev. Med. Chile. 2003; 131 (2):213-219. http://dx.doi.org/10.4067/S0034-98872003000200013.
CrossRef - Kuhle S, Ashley-Martin, Maguire, Hamilton DC. Percentile curves for skinfold thickness for Canadian children and youth. Peer J. 2016; 4 (e2247): 1-22. https://10.7717/peerj.2247.
CrossRef - Mramba L, Ngari M, Mwangome M, Muchai L, Bauni E, Walker S, Gibb DM, Fegan G, Berkley JA. A growth reference for mid upper arm circumference for age among school age children and adolescents, and validation for mortality: growth curve construction and longitudinal cohort study. BMJ. 2017;358 (j3423): 1-8. http://dx.doi.org/10.1136/bmj.j3423.
CrossRef - Subscapular and triceps skinfolds reference values of Hispanic American children and adolescents and their comparison with the reference of Centers for Disease Control and Prevention (CDC. Nutr Hosp. 2015;32(6):2862-2873. https://dx.doi.org/10.3305/nh.2015.32.6.9775.
- Aristizabal JC, Barona J, Hoyos M, Ruiz M, Marín C. Association between anthropometric indices and cardiometabolic risk factors in pre-school children. 2015; 15 (170): 1-8. https://dx.doi.org/10.1186/s12887-015-0500-y.
CrossRef - le Roux IM, le Roux K, Comulada WS, Greco EM, Desmond KA, Mbewu N, Rotheram-Borus MJ. Home visits by neighborhood Mentor Mothers provide timely recovery from childhood malnutrition in South Africa: results from a randomized controlled trial. Nutrition Journal 2010, 9 (56):1-10. http://www.nutritionj.com/content/9/1/56.
CrossRef - MacMillan-Uribe AL, Woelky KR, Olson B. Exploring family-medicine provider´s persepctives on group care visits for maternal and infant nutrition education. 2019; 51(4):409-418. https://doi.org/10.1016/j.jneb.2019.01.009.
CrossRef - Teshome G, Bosha T, Gebremedhin S. Time-to-recovery from severe acute malnutrition in children 6–59 months of age enrolled in the outpatient treatment program in Shebedino, Southern Ethiopia: a prospective cohort study. 2019; 19 (33):1-10. https://doi.org/10.1186/s12887-019-1407-9.
CrossRef - Reyes-Hernández J, Gallegos-Martínez J. La desnutrición infantil: población rural del Programa Oportunidades. ISSN : 1989-9300 Revista Académica de Investigación Tlatemoani. Grupo Eumed-Universidad de Málaga, España, Universidad Autónoma de San Luis Potosí, México, 2012; 9: 1-23.
- Jiménez CR, Moreno NB, Leyton RM, et al. Motivation and stages of change for physical exercise in adolescents. Rev Lat Psicol. 2015; 47: 196-204. https://doi.org/10.1016/j.rlp.2014.11.001.
CrossRef
Accepted on: 20 Feb 2021
Second Review by: Padam Dahal India
Final Approval by: Neha Sanwalka





Web of Science Coverage
Emerging Sources Citation Index (ESCI)
2024 Journal Impact Factor: 1.1
Scopus Journal Metrics
CiteScore 2025: 2.6
CiteScore Details
Sustainable Nutrition: Food Systems, Nutrient Retention, and Public Health Impact
![]()
This journal is a member of, and subscribes to the principles of, the Committee on Publication Ethics (COPE)








