Infant and Young Child Feeding (IYCF) Practices, Household Food Security and Nutritional Status of Under-Five Children in Cox’s Bazar, Bangladesh.
 , , , ,
, , , , 1North South University, Dhaka,Bangladesh
2Institute of Nutrition and Food Science, University of Dhaka, Bangladesh
3FHI 360, Dhaka, Bangladesh.
Corresponding Author Email: rifatahmed011@gmail.com
DOI : http://dx.doi.org/10.12944/CRNFSJ.6.3.21
Download this article as:
![]()
This study was conducted among people in the two southern most sub-districts or Upazilas (Teknaf and Ukhiya) of Bangladesh. This area is known nationally and internationally for a number of reasons including the presence of Rohingya refugees, the longest sea beach in the world, the location of a crucial international border between Bangladesh and Myanmar, and its Rakhaine ethnic population. This study focuses on the host community people of these two Upazilas from a nutritional lens. Objectives To assess the socio-economic status, infant and young child feeding (IYCF) practices, household food security levels, hygiene, sanitation and healthcare seeking behavior, and also the nutritional status of children under-five among the population of Teknaf and Ukhiya Upazilas of Cox's Bazar, Bangladesh. The study employed a cross sectional approach. A total of 300 households with at least one 6-59 month old child were randomly selected by two stage cluster sampling in 2014. Data was collected through direct interviews with the participants using a structured questionnaire. Analysis of the data was carried out using the Statistical Package for Social Sciences (version16.0 SPSS Inc, Chicago, IL, USA) and Emergency Nutrition Assessment (ENA) software. Food security was measured by Household Food Insecurity Access Score (HFIAS). The study found that 43.6% of the children were breastfed within 1 hour of birth, 41.9% ofthe children were exclusively breastfed up to six months, and the average duration of exclusive breastfeeding was 5.2 months. Age appropriate meal frequency was found
inaccurate for 60.3% of the children aged 9-11 month. The rates of severe stunting, wasting, and underweight among the children were 16.0%, 3.0% and 14.6% respectively. Among the households, 46.9% were severely food insecure. It was found that household food insecurity was significantly associated with household income (p=0.000), maternal education (p=0.000),and stunting (p= 0.005) and wasting (p=0.044) for children under-five. Overall IYCF practices, nutritional status of under-five children and household food security among the studied population were not at a satisfactory level and the status was lower than reference data for the same region.
Cox's Bazar; Food Security; Infant and Young Child Feeding (IYCF); Nutritional Status
Introduction
Teknaf and Ukhiya are the two southern most Upazil as (sub-districts) under Cox’s Bazar district of Bangladesh. For a number of reasons, these areas have national and international attention. The world longest uninterrupted sea beach is there, this area contains a large number of forcibly displaced Rohingya refugees from Myanmar; there is Rakhain ethnic population group who have unique language, lifestyle,. culture and norms, and a portion of the border between Bangladesh and Myanmar is also situated there1 In addition, this area is one of the most natural disaster prone areas in Bangladesh.2 Due to the presence of Rohingya refugees in different registered camps and make shift settlements, a number of humanitarian organizations work in this area. However, it is important to know about the status of the host community people in terms of nutrition and food related indicators for which this study was mainly planned. In recent years, although Bangladesh has kept the economic progress upward, the development is not homogenous among all the different population groups. It ranks 146th out of 187 countries in the 2010 Human Development Index (HDI) and 70th out of 122 countries in the 2011 Global Hunger Index (GHI).3,4 In 2009, almost half (48.6%) of the children aged 6-59 months were stunted or chronically malnourished; while 37.4% were underweight (acute and/or chronic malnutrition).5 In addition, more children aged 6-23 months were more malnourished than the children in the 24-59 months age group. This was mainly related to poor Infant and Young Child Feeding (IYCF) practices.5 Although the rate of stunting among under-5 children has been reduced over the years to 36%, the process is not as fast as the economic growth of the country.6 Cox’s Bazar district suffers from some of the lowest social and economic indicators in the country, although there is socio-economic vulnerability everywhere in Bangladesh. Moreover, the district’s geographical location makes its inhabitants particularly vulnerable to natural disasters.7
According to Household Food Security and Nutrition Assessment (HFSNA) in 2009, nationally 25% households were found food insecure whereas 72.3% of households were found food insecure by Food Security and Nutrition Surveillance Project (FSNSP-2011) in the eastern hill region of Bangladesh under which the study area belongs.5,8 The studied Upazilas demonstrate some of the most alarming development indicators, with over 60% being poor in Teknaf Upazila according to the latest World Food program (WFP) poverty Map.9 Malnutrition is both a typical cause and a blemishing consequence of poverty.10 Malnutrition or under-nutrition is the physiological outcome of hunger and/or illness and manifests itself in numerous macronutrient and micronutrient deficiencies.11 It has both short-term and long-term consequences. The short-term consequences are morbidity, disability and mortality; where in the long term it affects a broad range of issues including educational prospects, productive employment, and economic capacity.12-13 Therefore, malnutrition may also be one of the principle mechanisms behind the transmission of poverty and inequality from one generation to the next.12 According to the conceptual framework of malnutrition, the underlying causes of malnutrition are inadequate access to food or food insecurity, impaired psycho-social environment and care practices and poor water and sanitation, public health and hygiene. These underlying causes are commonly influenced by poverty.14,15
Food security covers social availability of foods, access to purchasing capability and proper utilization and despite some limitations, household food insecurity access scale (HFIAS) is one of the tools to measure it at household level.16 As per HFIAS, the household food insecurity has two broad components, such as, the access component and the utilization component. First, the access component is characterized by anxiety and uncertainty about household food supply, insufficient quality of food, and insufficient food intake by household members. Second, the utilization component is mostly influenced by nutrition knowledge and beliefs, but also by access to healthcare, water, and sanitation services and practices related to the management of childhood illness and hygiene.17-19 As an underlying cause, household food insecurity can shape the nutrient intake and nutritional status at household level.20 Household food security and nutrition programs should place stronger focus on improving complementary feeding and exclusive breastfeeding practices in the vulnerable areas, ensuring greater enrollment of women at community health centers, providing more intensive training to community outreach workers.21 The improved referral systems and better management of severely malnourished children at the community health care centers is also needed for strengthening the nutrition programs as seen in the areas where this study was conducted.22
Study Objectives
The objectives of this study was to assess the socioeconomic status, IYCF practices, nutritional status of under-five children and the status of household food security of the people living around Rohingya refugee camps in Teknaf and UkhiyaUpazilas of Cox’s Bazar.
Methodology
The study design was cross-sectional. The study area was Teknaf and Ukhiya Upazilas of Cox’s Bazar district and the target population was the local host community. Households with at least one 6-59 month old child were included in the study. Households were selected randomly through (30×10) two-stage-cluster sampling to ensure 300 households with at least one 6-59 month old child be included in the study to give the representative sample size as calculated by the following sampling procedure.
![]()
Where, p=prevalence of wasting (15.9%) among the under-five children in Chittagong division, q=1-p, z=standard deviation (1.96 at 95% confidence interval), d=degree of freedom (5%), DE=design effect (1.46).
In the first stage, before going to the field, 30 villages (clusters) were selected from these two Upazilas with probability proportionate to the size (PPS) of the population in each village. In the second stage, from every cluster 10 households were selected randomly and data were collected. Once the data were collected from the targeted number of households in a particular cluster, the cluster was considered fulfilled. Data collection was conducted during February 2014 to April 2014. Before interviewing, the objectives of the study were made clear to the respondents before requesting their consent. For the socioeconomic indicators, both father and mother of the caregivers were considered, if possible, and IYCF information was received by in-depth interviewing only the mothers. For anthropometric measurements, Mid Upper Arm Circumference (MUAC) was measured using MUAC tape (S0145620 MUAC, Child 11.5 Red/PAC-50), weighing scale (Salter Type Baby Weighing Scale and Digital Bath Scale) was used to measure the body weights and, height-length measuring board (RC-HMB01) was used as appropriate. The weight, height and MUAC were measured to the nearest values of ±100g, ±0.1cm and ±1.0mm respectively after standardizing the measurements regularly before the data collection. Questionnaires were also used to collect the data required for this study. Edema was checked bilaterally by the standard prescribed protocol.23 Event calendar was used to get support for accurate age determination. Food security was measured using the HFIAS by Food and Nutrition Technical Assistance (FANTA). The results obtained for the Heights and Weights were used for assessing the nutritional status of the children by calculating Z-scores using the Emergency Nutrition Assessment (ENA) software. The standard cut-off values were used to categorize stunting: height for age Z-score (HAZ); underweight: weight for age Z-score (WAZ); wasting: weight for height Z-score (WHZ). The Statistical Package for Social Sciences (version 16.0 SPSS Inc, Chicago, IL, USA) software was used for calculating the other variables and test statistics. To observe the associations among the variables, Pearson Chi-square test (at α level 0.05) was carried out.
Findings
All the 300 randomly selected households gave consent to participate in the study. This gave a consent rate of 100%. As per the objectives of the study and the analysis of the data, findings can be
presented as following.
Socio-Economic Status
The mean (±standard deviation) age of the caregivers/mothers was 24.3 ± 4.0 years. The number of under-five children per mother per household ranged from 1 to 3. Average family size was 6 to 8 members per family. Literacy rate among the fathers (62.7%) was higher than that of the mothers (44.7%) and 8.0% of the mothers was involved in income generating activities. Average monthly family income was BDT 7,856.67 (USD 93.00) of which 66.2% was spent on food.
Only 8.0% mothers participated in regular income generating activities. There were common, casual livelihoods like brick field labor, wharf, and construction worker which were engaged by both male (36.3%) and female (4%). The study area was near to the sea thus a large proportion of the fathers were involved in fishing (17.3%) although a larger proportion was involved in driving (20.4%). The area is prone to flash flood and there is salinity in the surface water. For this reason, may be the cause why less people were involved in agriculture (6.3%). A total of 13.3% of the fathers and 3.3% of the mothers were involved in business mainly related to salt production, dry fish preparation, small and medium entrepreneurship and 6.4% of the fathers and 0.7% of the mothers were involved in other services. The largest proportion of the mothers (92.0%) labored in unpaid household activities.
Hygiene, Sanitation and Healthcare
Each of the 300 family that participated in this study had access to tube-well for drinking water; 98% of all the families had their own toilet facility, but only 24.3% of all the families had sanitary toilet facility. Most of the toilets were either trench (44%) or hanging (31.7%) type. Regarding morbidity, the disease episodes among the children in the last two month period was mainly diarrhea (42.1%), common fever and cold (47.0%) and pneumonia (2%). A total of 91.0% of the mothers were able to show the vaccination card for their children. Coverage of vitamin A supplementation and de-worming was 99.7% and 98.4% respectively. Only 0.7% of all the children attended regular growth monitoring and promotion (GMP) sessions.
Infant and Young Child Feeding (IYCF) Practice
Analysis of the data obtained on the IYCF practices for 236 children age 6-23 months indicated that each of them was breastfed by the mother. Rate of early initiation of breastfeeding and exclusive breastfeeding were 43.6% and 41.9% respectively. A total of 56.4% of the 236 children were provided pre-lacteal foods (water/honey) prior to breast milk. On average, the duration of exclusive breastfeeding was 5.2 (±0.78) months and the average age of initiating proper complementary foods was 5.9 (±0.68) months.
Appropriateness of age specific complementary food frequency among 6-23 month old children can be represented as shown in Table 1, where the light green and light orange cells indicate the correct and wrong practices respectively. For 6-8 month old children, the frequency of the complementary foods was appropriate for 96.8% cases, but for the 9-11 month and 12-23 month old children the appropriateness was only 39.7% and 57.4% respectively.
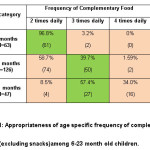 |
Table 1: Appropriateness of Age Specific Frequency of Complementary Foods (excluding snacks) Among 6-23 Month Old Children. |
Household Food Insecurity
Regarding the status of household food insecurity, as represented by Figure-1, shows that 19.0% of households were food secure as per the HFIAS but the status of moderate and severe food insecurity was 34.1% and 46.9% respectively among the households that participated in this study.
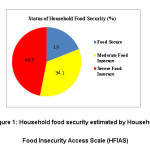 |
Figure 1: Household food security estimated by Household Food Insecurity Access Scale (HFIAS) |
Status of Malnutrition
Status of malnutrition among the 6-59 month old children from the studied households shows(Table-2) that the status of severe and moderate wasting among the children was 3.0% and 17.0% respectively. The rate of severe and moderate stunting was 16.0% and 28.7% respectively and for the underweight, the rate was 14.6% and 29.7% respectively. No statistically significant (P>0.05) difference was found between boys and girls in terms of their status of stunting, wasting, and underweight.
Table 2: Nutritional Status of the Under-5 Children.
| Wasting (WHZ<-2SD or MUAC<12.5cm) |
Boys(N=158) | Girls(N=142) | Total(N=300) | P-value* |
| Wasting (WHZ<-2SD or MUAC<12.5cm) Severe wasting | 5.1% (8) | 0.7% (1) | 3.0% (9) | |
| Moderate wasting | 18.9% (30) | 14.8% (21) | 17.0% (51) | |
| Not wasted | 75.9% (120) | 84.5% (120) | 80.0% (240) | |
| Stunting (HAZ<-2SD) Severes tunting | 14.6% (23) | 17.6% (25) | 16.0% (48) | |
| Moderate stunting | 25.9% (41) | 31.7% (45) | 28.7% (86) | >0.05 |
| Not stunted | 59.5% (94) | 50.7% (72) | 55.3% (166) | |
| Underweight (WAZ<-2SD) Severe underweight | 15.2% (24) | 14.1% (20) | 14.6% (44) | |
| Moderate underweight | 27.8% (44) | 31.7% (45) | 29.7% (89) | >0.05 |
| Not underweight | 56.9% (90) | 54.2% (77) | 55.7% (167) |
Data are presented as % (n), n=number of sample
Differences were considered to be statistically significant at P-value <0.05
*P-value was calculated by Pearson Chi-square (χ 2 ) test (2 tailed, α=0.05)
Measures of Associations
Associations among the variables (as presented in Table-3) indicate that household food insecurity was significantly associated with the household income (p=0.000), maternal education (p=0.000), stunting (p=0.005) and wasting (p=0.044) of the under five children.
Table 3: Associations Among the Variables.
| Variables(N=300) | Stunting (%) | P-value* | Wasting (%) | P-value* | Underweight (%) | P-value* | Food insecurity (%) | P-value* |
| Household incomeQ1(lowest percentile) | 17.7 | 0.483 | 9.3 | 0.849 | 18.7 | 0.765 | 38.0 | 0.000 |
| Q2 (mid percentile) | 17.0 | 6.7 | 15.0 | 28.3 | ||||
| Q3(highest percentile) | 10.7 | 4.3 | 11.0 | 12.0 | ||||
| Maternal education Illiterate | 27.7 | 0.047 | 9.3 | 0.146 | 24.7 | 0.999 | 50.0 | 0.000 |
| Primary | 15.7 | 10.7 | 18.7 | 27.0 | ||||
| Educated (≥SSC**) | 2.0 | 0.3 | 1.3 | 0.0 | ||||
| Food insecurityNo insecurity | 5.0 | 0.005 | 4.3 | 0.044 | 6.7 | 0.271 | – | – |
| Moderate | 18.0 | 6.3 | 16.3 | |||||
| Severe | 19.7 | 8.7 | 19.3 |
Differences were considered to be statistically significant at P-value <0.05Data are presented as % (n), n=number of sample
*P-value was calculated by Pearson Chi-square (χ 2 ) test (2 tailed, α=0.05)
**Secondary School Certificate (SSC)
Discussion
There are no published data on the statistics about the people of Teknaf and Ukhiya Upazila of Cox’s Bazar district in terms of their socioeconomic status, IYCF practices, food security and nutritional status of under five children. This area is under the Chittagong division of Bangladesh which is in the eastern hill region. For this reason, to compare the findings, available survey data was used that represent the status of overall Chittagong division as well as the eastern hill survey region (FSNSP) of Bangladesh.20,24 The socio-economic data obtained from the areas in the present study varies from the other parts of this region as well as from other coastal areas of Bangladesh. These two Upazilas, Teknaf and Ukhiya, are unique from other parts of Bangladesh because of the presence of Rohingya refugees in this area who currently number more than the number of native host community people. They are Rakhine tribal peoples who also have own language, lifestyle, food habits and social norms. These items have impacts on the socio-economic variables of this area. The Rohingya refugees are reliant on external aids that are met by the humanitarian and government organizations that have in turn also made the local people engage in related activities.25 An exact study is yet to be done but many local people seem to earn their livelihood through working with the organizations for the refugee people. The refugees must have an impact on the availability of local food sources, although no exact finding has been established as of yet on the impact on the household food availability of the host community people. In the present study, the average household size (7.0 people) among the studied population was higher than the average household size of the overall Chittagong division (5.0 people) as well as for the families living in the eastern hill areas of Bangladesh.20 When compared to the results on occupations of the parents in this study, the reference data shows that in eastern hill areas of Bangladesh, the parents occupations were mainly unskilled labor (21%), business (21%) and agriculture (26%). Although fishing was not clearly specified in the reference data, it lies under skilled labor (9%). A total of 8% of the mothers in the present study were involved in income generating activities, which is less than the 18% of mothers in Chittagong division as well as the 17% in coastal belt areas for the same indicator. One possible cause for the difference may be because there is a large household size and mothers have more babies for which they are mainly involved in household activities and nurturing their children. There might also be some social practices, in terms of restriction, regarding the outdoor involvement of women for income generation. The literacy rate among the fathers and the mothers in the present study was lower than the overall literacy rate in Chittagong division (79%) and eastern hill areas of Bangladesh (68.0%).20 Although these two Upazilas are critically important for many reasons, due to the refugee context, ethnicity of a small section of the population, and tourist attraction, the low literacy rate might be linked to the geographical isolation of the area. The area features income-generating activities like fishing, salt production and driving which draw this younger population group to be involved in income generation activities in lieu of education.
Hygiene and sanitation related data shows all families had access to tube well for getting drinking water and this coverage is better than the status of Chittagong division (95%) as well as coastal belt areas (84%). According to multiple indicator cluster survey (MICS 2012-13), in Cox’s Bazar 99.8% households have improved drinking water.24 Unlike the results obtained in our present study, the coastal belt region coverage of sanitary toilet among the households was 43% and according to multiple indicator cluster survey (MICS 2012-13) and this coverage in Cox’s Bazar district was 51.5%. Vitamin A supplementation coverage shows 99.7% children were supplemented through the national campaign; this coverage was more than the 82% vitamin A supplementation coverage in Chittagong division as well as the 83% coverage in the eastern hill region of Bangladesh.20 Coverage of de-worming among 24-59 month children in our present study was higher than the 62% reported in the Chittagong division. The high coverage of vitamin A supplementation and de-worming might be due to the many non-governmental organizations working with the health sector in the study area. Reference data shows prevalence rate of fever and diarrhea among the children of eastern hill areas of Bangladesh was 42% and 8% respectively.20
It was defined that a very low percentage of children who attended growth monitoring and promotion (GMP), may be due to inappropriate or lack of sensitization and guidelines from the health authority as well as limited education of the parents. Qualitative evidence revealed that the parents did not know that there is the system to check the growth and development of their children. They were mainly aware of the illness of their children and most of them thought the monitoring of growth is not required and not important. From service delivery point, service providers from the public and private sectors also work with nutrition but GMP is not focused strongly. Moreover, one or two sessions of GMP is often agreed by the mothers, may be for the purpose of malnutrition screening, but it was not conducted seriously for long term on a monthly basis.
Infant and young child feeding is very important for growth, cognition and well-being of the children. Findings show that the rate of children who were breastfed at an early initiation of breastfeeding (within 1 hour) was only 43.6% which is similar to the status of overall Cox’s Bazar district (41.4%) but less than the overall status of eastern hill areas (54%).20, 24 On the other hand, provision of pre-lacteal foods, any food prior to breastfeeding to newborn babies, was found to be at a very high rate (56.4%). As per delivery history from the mothers, low rate of early initiation of breastfeeding might be due to low coverage of institutional delivery, delay in breast milk secretion and social misconceptions in favor of pre-lacteal feeding. Most of the cases the pre-lacteal foods were honey, raw water, and bottle milk feeding. In our study both the status of exclusive breastfeeding was far less than the overall status of Cox’s Bazar district (64.6%) and provision of pre-lacteal food had a vital influence on it. Considering exclusive breastfeeding and complementary feeding, there is a gap between the average duration of exclusive breastfeeding (5.2 months) and average timing of initiation of proper complementary feeding (5.9 months). During this time mothers just provide snacks and different types of soft/semi-solid foods (hotchpotch, cereal powder, banana and porridge) to the children regardless of maintaining any frequency or dietary diversity. Age appropriate meal frequency, except for snacks, shows 93.2% of 9-11 month children were provided 2 meals per day instead of 3 meals recommended by national IYCF guidelines.26 The age specific meal frequency for children is often confused for the 9-11 month children group. The rate of age specific minimum meal frequency among 6-23 month children in Chittagong division was 80% and for coastal belt regions it was 84%. In this study only 6-8 month children were given complementary foods at the satisfactory level compared to other age groups.
Nutritional anthropometric data shows the rate of severe (<-3SD) wasting, stunting and underweight, as calculated by Z-score, among under-5 children were 3%, 16% and 14.6% respectively. According to the multiple indicator cluster survey (MICS 2012-13), the status of severe wasting, stunting and underweight among under-5 children in Cox’s Bazar was 3%, 22.7% and 13% respectively. On the other hand, the rate of moderate (-3SD to <-2SD) wasting, stunting and underweight were 17%, 28.7% and 29.7% whereas, as per reference, for Cox’s Bazar district these prevalence were 10.1%, 49.5% and 40.5% respectively.24 It seems with the exception of moderate wasting, all the other indicators obtained in our present study were either similar or less than those in the reference data for Cox’s Bazar. The difference might be due to variation in data collection time or there might be a seasonal variation of malnutrition in the studied areas. Our results indicate that the pattern of malnutrition was more acute than chronic. There might be a number of factors behind this idea that requires more studies to be done in future for proper clarification of the issues.
Conclusion
The overall status of infant and young child feeding, household food security and the nutrition of under-five children was not optimum compared to the reference data. Further investigation should be carried out for better clarification and to target the appropriate interventions.
Acknowledgements
The study was technically supported by North South University (NSU), Bangladesh. Thanks must go to the respondents who were kind enough for agreeing the interview.
Conflict of Interest
Authors declare no conflict of interest.
Ethical Statement
The authors state that this is an original article and it had not been submitted to any other journal for publication. The data are original and the volume of data was not split to create more publications. There was no manipulation done by the researchers that would question the ethics of the study.
References
- Ullah A. A. Rohingya refugees to Bangladesh: Historical exclusion and contemporary marginalization. Journal of Immigrant and Refugee Studies. 2011;9(2):139-161.
CrossRef - International Federation of Red Cross and Red Crescent Societies. (2011). Information Bulletin Bangladesh: Cox’s Bazar Floods, Information bulletin no 1. 2011.
- International Food Policy Research Institute/Concern worldwide/Welt Hunger Hilfe. Global Hunger Index -The challenge of hunger: Taming Price Spikes and Excessive Food Price Volatility. October 2011, Bonn, Washington D.C., Dublin. 2011.
- United Nations Development Programme. (2011).Human Development Report 2011, Sustainability and Equity: A Better Future for All in Human development statistical annex. New York: UNDP. 2011;127-130.
CrossRef - World Food Programme/United Nations Children‘s Fund/Institute of Public Health Nutrition. Bangladesh Household Food Security and Nutrition Assessment Report 2009. Dhaka. 2009.
- National Institute of Population Research and Training (NIPORT), Mitra and Associates, and ICF International. Bangladesh Demographic and Health Survey 2014: Key Indicators. Dhaka, Bangladesh, and Rockville, Maryland, USA. 2015.
- Bangladesh Bureau of Statistics. Preliminary Report on Household Income and Expenditure Survey – 2010, Dhaka. 2011.
- Helen Keller International. The Food Security and Nutrition Surveillance Project, Round 4: February-May 2011, Preliminary Result, Bulletin No2. 2011.
- Bangladesh Bureau of Statistics/World Bank/World Food Programme. Updating Poverty Maps of Bangladesh, Key Findings. 2009.
- Hunt., Joseph., Quibria M. G. Investing in Child Nutrition in Asia, Asian Development Bank Nutrition and Development Series, 1 (Preface). 1999.
- Action Contre la Faim International. (2010).Taking action: Nutrition for Survival, Growth and Development, White Paper. 2010.
- The Sphere Project. ). Humanitarian Charter and Minimum Standard for Humanitarian Response. 2011;146.
- Action Contre la Faim International Network. Acute Malnutrition: A Preventable Pandemic. New York. 2009.
- Action Contre la Faim International, Technical Department of Food Security and Livelihood. Food Security and Livelihood Assessment: A Practical Guideline for Field Worker. 2010.
- Action Contre la Faim International Network. (2008).Positioning Paper: Research Policy ACFIN.
- Coates J., Swindale A., Bilinsky P. Household Food Insecurity Access Scale (HFIAS) for measurement of food access: indicator guide. Washington, DC: Food and Nutrition Technical Assistance Project, Academy for Educational Development. 2007;34.
- Wolfe W. S., Frongillo E. A. Building household food-security measurement tools from the ground up. Food and Nutrition Bulletin. 2001;22:5–12.
CrossRef - Coates J., Frongillo E. A., Rogers B. L., Webb P., Wilde P., Houser R. (2006).Commonalities in the experience of household food insecurity across cultures: what are measures missing? Nutr.,May. 2006;136:1438-1448.
- Coates., Jennifer., Anne Swindale., Paula Bilinsky. (2007).Household Food Insecurity Access Scale (HFIAS) for Measurement of Household Food Access: Indicator Guide (v.3).Washington, D.C.: Food and NutritionTechnical Assistance Project, Academy for Educational Development, August. 2007.
- Helen Keller International (HKI) and James P. Grant School of Public Health (JPGSPH). (2016) State of food security and nutrition in Bangladesh: 2014. Dhaka, BD: HKI and JPGSPH. State of food security and nutrition in Bangladesh: 2014. Dhaka. 2016.
- Bangladesh Rural Advancement Committee. Research Report “The Food Supplementation Process in BRAC Areas under the Nutrition Project NNP”. Dhaka. 2006.
- Faruque A. S. G. et al. “Nutrition: Basis for Healthy Children & Mothers in Bangladesh”, Journal of Health, Population and Nutrition. 2008;26(3).
CrossRef - Institute of Public Health Nutrition (IPHN). National guidelines for community based management of acute malnutrition in Bangladesh: September 2011. Dhaka. 2011.
- UNICEF Bangladesh, Multiple indicator cluster survey 2012-2013. 2014.
- Frontières-Holland, M. S. 10 years for the Rohingya refugees in Bangladesh: Past, present and future. MSF-Holland, March, 5. 2002.
- Hackett., Kristy M. et al (2015). “Knowledge, attitudes and perceptions on infant and young child nutrition and feeding among adolescent girls and young mothers in rural Bangladesh.” Maternal and child nutrition2. 2015;173-189.
CrossRef
Accepted on: 02-11-2018
Second Review by: Dr. Shipra Gupta (India)
Final Approval by: Prof. Victor J. Temple





Web of Science Coverage
Emerging Sources Citation Index (ESCI)
2024 Journal Impact Factor: 1.1
Scopus Journal Metrics
CiteScore 2025: 2.6
CiteScore Details
Sustainable Nutrition: Food Systems, Nutrient Retention, and Public Health Impact
![]()
This journal is a member of, and subscribes to the principles of, the Committee on Publication Ethics (COPE)








