Assessment of Knowledge, Attitude and Practice of Adults in Jeddah About Food Interaction
 , , , , ,
, , , , , 1 Medical student, Faculty of Medicine, King AbdulAziz University, Jeddah, Saudi Arabia
2Food and Nutrition Research Unit
3Saudi Diabetes Research Group, King Fahd Medical Research Center, King Abdulaziz University, Jeddah, Saudi Arabia
4Dept. Clin Biochem. Faculty of Medicine, King AbdulAziz University, Jeddah, Saudi Arabia
5Department of Food and Nutrition- Home Economics, King Abdulaziz University, Jeddah, Saudi Arabia.
Corresponding Author Email: sbahijri@gmail.com
DOI : http://dx.doi.org/10.12944/CRNFSJ.4.3.02
Download this article as:
![]()
Cultural beliefs and practices, and improper use of medications of Saudis may be associated with poor nutritional status. The purpose of this study was assess knowledge, attitude and practice of Saudi adults regarding possible effects of selected food combinations, and effects of medications on nutritional status, in association with gender, age and educational level. A questionnaire was constructed to include demographic information, some food combinations culturally avoided, or scientifically known to adversely affect nutritional status, possible interactions of food with medications, sources of information, and personal experience of adverse effects following certain food combinations. Subjects were recruited from public areas to complete the questionnaire. An electronic version was distributed through social network. A total of 998 questionnaires were completed, with 60.9% females, 66.5% ≤25 years of age, and 75.6% having university degree. Women, and subjects with ≥ secondary school education had significantly higher knowledge score (P= 0.007, and 0.01 respectively). The majority of participants did not know food combinations that can adversely affect nutritional status, especially those having < secondary school certificate. Significantly higher proportion of subjects > 40 years of age believed in traditional taboos (P= 0.038). Attitude was affected by gender. Hearsay and media were major sources of information, with higher percentage of females intentionally seeking knowledge. Nutritional knowledge is poor among Saudis, with folklore, and media being main sources. This might contribute to the increased prevalence of nutrition related diseases. Nutrition education programmes should be introduced early in life through different channels.
KEYWORDS:Assessment questionnaire; Nutritional Knowledge; Food combinations; Food-food interactions; Drug-food interactions
Introduction
Micronutrients deficiencies are still quite common globally, even in developed and affluent countries.1,2 In particular, deficiencies in iron, iodine, vitamin A, folate and zinc can have devastating consequences. At least half of children worldwide ages 6 months to 5 years suffer from one or more micronutrient deficiency, and globally more than 2 billion people are affected.3 Saudi Arabia is no exception, with reports of various forms of anemia; including iron and folate deficiencies,4-6 zinc deficiency,7 vitamin A,8-10 and vitamin D11-13 deficiencies, and iodine deficiency14 found in literature. Unavailability of food, or eating an unbalanced diet that does not contain all nutrients necessary for good nutritional status are the immediate causes of nutritional deficiencies. In addition, social factors and cultural practices in most countries have a very great influence on what people eat, on how they prepare and combine various food types, on their feeding practices and on the foods they prefer, hence adequacy of their diet. Indeed, some traditional food practices and taboos in some societies may contribute to nutritional deficiencies among particular groups of the population. Food combining is one of the primary factors that can affect digestion, and absorption of various nutrients; thus; altering their bioavailability, and hence their assimilation.15 Therefore, commonly used; or avoided; food combinations in a community could be either deleterious or beneficial to nutritional status. Furthermore, population groups with higher nutrient. requirements, such as infants, adolescents, and pregnant and lactating women, may be more sensitive to nutrient- nutrient interactions.16 In addition, many commonly prescribed medications can interfere with the body’s ability to absorb and utilize nutrients.17 Nutritionists need to have a knowledge of the food habits, practices, and taboos of the communities in which they work so that they can help to reinforce the positive habits as well as strive to change any negative ones. Knowledge of drug/nutrient, and food- food interaction, including common food combinations used, or avoided in the community has not been previously studied in Saudi Arabia. Therefore, the aim of this study was to assess the knowledge of Saudi adults; randomly selected from Jeddah residents; about the possible effects of selected food combinations on nutritional status, as well as the effects of medications on nutrients bioavailability and metabolism. In addition, their source of information, and their attitude towards possible food or nutrient interactions, as well as the possible influence of gender, age and educational level were investigated.
Subjects and Methods
A short list of food combinations commonly believed to cause discomfort or disease; hence tabooed; as well as beliefs regarding the effect of physiological variables, and medications on expected effects, was collected from various local sources, including: folklore, social network and personal contacts. This was incorporated into a questionnaire constructed in clear Arabic, which also included the food – food interactions scientifically known to have negative effects on nutritional status (such as tea with iron containing foods, and phytate or oxalate rich foods with dairy products), sources of information (folklore and religious beliefs, hearsay, and unreliable sources, versus accredited sources), and questions on personal experience of adverse affects caused by certain food combinations or food- food interactions (symptoms, action taken, and effect on future dietary practices), in addition to demographic information on age, gender and educational attainment. The questionnaire was tested for clarity on 100 adult men and women aged 18- 75 years. The final version of the questionnaire; in addition to demographic information (3 questions), consisted of 23 multiple choice or true and false questions divided into:, knowledge (16 questions- Table 1), sources of knowledge, and previous experience with food- food interaction as well as ways of coping with it (7 questions) (Table 2). A score out of 16 was given to the knowledge section. The research was approved by “the Committee on the Ethics of Human Research” at King Abdulaziz University, Jeddah, Saudi Arabia. A cross sectional design was employed to recruit a convenience sample of apparently healthy men and women aged ≥ 18 years from the general adult population in public areas such as malls and waiting areas in hospitals during the period April 1, 2013 to March 31, 2014. Willing subjects were asked to complete the designed questionnaire. In addition an electronic version was distributed through social network.
Table 1: Questions testing knowledge of food/ food and drug / food interactions, and their answers
|
Questions |
Expected correct answer |
|
Yes |
|
No |
|
No |
|
No |
|
No |
|
Yes |
|
Yes |
|
No |
|
No |
|
Yes |
|
Yes |
|
No |
|
No |
|
No |
|
Yes |
|
Yes |
Table 2: Questions testing experience and attitude about food/ food and drug / food interactions, and indicating source of knowledge.
|
Questions |
Given Choices |
|
a)Yes b)No |
|
a)Yes b)No |
|
a) General feeling of discomfort and un-wellness, b)GI disturbances, c)Skin manifestations, d) others – More than one choice can be picked |
|
a)Resting and waiting, b) Self medication by taking laxatives or traditional herbal remedies, c) Seeing a doctor or going to hospital, d) other measures – More than one choice can be picked |
|
a)Yes b)No |
|
a)Religious teachings, b)School or college, c)The media, d)Friends and social contacts, e) Reading books, f) Browsing the internet, g)Family physician, h)Dietician, i) Health organizations, j) personal experience – More than one choice can be picked |
Statistical Analysis
The collected data were reviewed, coded, entered and analyzed using Statistical Package of Social Science (SPSS) software; version 20.0. Continuous variables were presented as mean values ± standard deviation, while qualitative variables were presented as absolute frequencies and relative frequencies (percentages). Contingency tables with calculation of chi-square test were used to evaluate association between categorical variables to assess the significance in the differences between proportions. On the other hand, the significance in the differences between means was assessed using independent Samples student t test for dichotomous nominal variables. All presented P-values were two-tailed and taken at a significance level of 0.05 and 95% Confidence Interval
Results
Valid returned forms were 998 questionnaires, with 608 or 60.9% of total filled by females. Demographic characteristics of participants are presented in table 3
Table 3: Demographic characteristics of participating males and females
|
|
Males N=390 |
Females N=608 |
Total N= 998 |
P Value |
|
|
Age categories
|
18-25 yrs |
244 (62.6%) |
420 (69.1%) |
664 (66.5%) |
0.007 |
|
26-40 yrs |
113 (29.0%) |
147 (24.2) |
260(26.1%) |
||
|
>40 yrs |
33 (8.5%) |
41 (6.7%) |
74 (7.4%) |
||
|
Educational attainments |
<Secondary school |
12 (3.1%) |
47 (7.7%) |
59 (5.9%) |
0.009 |
|
Secondary school |
76 (19.5%) |
108 (17.8%) |
184 (18.4%) |
||
|
≥Bachelor degree |
302 (77.4%) |
453 (74.5%) |
755 (75.6%) |
||
The majority of subjects (66.5%) were in the youngest age group, with less than 10% falling in the above 40 years category, but the distribution between age groups was significantly different between males and females, with a higher than expected percentage of females in the youngest age group, and lower percentage than expected in the other two age groups. In addition, most of the participants (75.6%) had at least a university degree. However, there was a significant gender difference in the distribution between different educational attainment categories, with a higher than expected percentage of females having less than secondary school certificate, and lower than expected percentage having secondary school
certificate, or university degree. Evaluation of Knowledge The mean score of participants in the knowledge section was 12.5, with a standard deviation of 1.83, and 559 (56% of total) having an above average score (>12.5). Women had a significantly higher mean score (13.4), compared to men (12.1) (P= 0.007). Educational attainment also had a significant effect on overall score (P= 0.01), with only 42.4% of participants with < secondary school qualifications had above an average score, compared to 56.9% for those with ≥ secondary school certificate . However, there was no significant effect due to age (P= 0.378), with 56.2% of participants ≤ 40 years of age obtaining above an average score, compared to 54.1% for the older group. Considering responses to individual knowledge questions, the outcome was different. The majority of responders (849 subjects – 85%of sample) acknowledged the existence of food- food interaction, and that it could be beneficial or deleterious to health, and/ or nutritional status (question 1- Table 1), with no significant difference between men and women (Figure 1a), nor between different age groups. However, educational level had a significant effect (P < 0.001) with 22 % of those having less than secondary school certificate being unaware of the fact, compared to a lower percentage of ≈15 % in the other two groups (Figure 1 b).
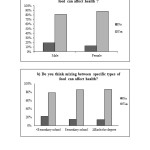 |
Figure 1: The percentage of participants acknowledging food/food interaction according to a) gender, b) educational attainment Click here to View figure |
Furthermore, misconceptions and lack of correct conceptions about unhealthy food combinations and various interactions were wide spread. Of note, the finding that 62.1% of the sample did not acknowledge the existence of drug-food or food- drug interactions, and interactions scientifically proven to affect nutritional status; such as tea and iron containing foods (Question 15- Table 1); were not known by 63% of the sample, with those having < secondary school certificate showing even a higher percentage of 85%. Similarly the effect of eating leafy vegetables and/or whole grains with dairy products (Question 6- Table 1) was unknown to 72% of the sample, with those having < secondary school certificate showing even a higher percentage of 91%. Age also had a significant effect on nutritional beliefs (P= 0.038), with almost half of those > 40 years of age (49.2%) believing in traditional taboos (Question 2-5, 8 &9- Table 1), compared to 38.9% of the younger age groups.
Evaluation of experience, attitude, and practice A total of 379 participant (44.6% of total sample) answered (yes), to question 1 in Table 2, thus indicated an experience of mixing between some specific types of food, with a significantly higher proportion of men compared to women (P= 0.041), but without a significant difference between age groups. However, only 154 of them (i.e. 40.6%) reported that they developed related ill health symptoms (Question 2- Table 2), with no significant difference between men and women , or between different age groups. Reported symptoms varied between choice a) general symptoms (15.6%), choice b) GI upset (71.5%), and choice c)skin manifestations (19.9%). However, only a very small percentage (9.1%) of those who had developed symptoms decided to stop mixing between these types of food, with a higher proportion of females compared to males (P= 0.047), but no difference between age groups, or due to educational attainment. Answers to methods used to alleviate symptoms (question 4- Table 2) also varied between choice a)Resting and waiting reported by 23.3% of those experiencing symptoms, choice b) Self medication by taking laxatives or traditional herbal remedies reported by 52.2% , and choice c) Seeing a doctor or going to hospital reported by 24.5%. Significant difference was noted between genders (P= 0.047), with a higher percentage of females resorting to choice b), and a higher percentage of men preferring choice a). In addition, a significantly higher percentage of participants ≤ 40 years preferred choice c) (P= 0.041). Regarding the source of their knowledge, only 1.1% of participants reported obtaining their knowledge from religious teachings (choice a- in question 6), while 55% of participants ( with a significantly higher proportion of > 40 years age group, P=0.038) reported obtaining their knowledge without making a conscious effort through social talks and meeting, or an actual personal experience (choices d- and j- in question 6), while 33% of subjects (mainly ≤ 40 years of both genders) reported making a personal unguided effort by browsing the internet (choice f- in question 6) , listening, watching or reading material available in the media(choice c- in question 6) (mainly females having > secondary school certificate), or by reading simple books (choice d- in question 6) (mainly those having > secondary school certificate). Only 12% of the participants made a conscious effort to obtain reliable information either from their own study programme (mainly females ≤ 40 years of age), or from professional sources by asking doctors, dieticians, or from information provided by health organization(choices b-, and g- to i- in question 6) (mainly females > 40 years of age).
Discussion
The interplay of many factors determine food- related behavior. These include: sociodemographic (income, education and occupation), physiological, as well as behavioral and life style factors, in addition to knowledge and attitudes related to diet and health [18, 19]. In spite of huge development and modernization in Saudi Arabia during the last four decades, nutritional deficiencies are still encountered and documented in literature.4-14 Food habits, and taboos may play a role, since food is not in shortage, and food choices have increased due to the improvement in economic status. Indeed, obesity among adults showed a progressive increase from 22% in 1990–199320 to 36% in 2005,21 and is projected to increase to 41% by 2022 in men, and to 78% in women particularly in the age groups 35–44, 45–54 and 55–64 years.22 These contrasting reports strongly suggest poor nutritional knowledge, and dietary practices; including avoiding or promoting certain food combination; among Saudis. In addition to health professionals, the contributions of professionals in many other spheres are needed to evaluate causes, and suggest possible solutions to these diet related conditions. No previous studies have been conducted in our region to study food habits, as well as beliefs and taboos regarding healthy nutritional practices. Our study is the first to assess knowledge, attitude, beliefs and practice in Saudi Arabia, hoping to provide some clues to existing diet related controversies. It is well established that components present in ingested meals may alter the mineral bioavailability in them, leading to better or poorer absorption.15 For example, beverages high in polyphenol content can be potent inhibitors of iron absorption especially non- heam iron,23 and better calcium uptake is found when taken together with oligofructose.24 In addition to its effect on micronutrient bioavailability, food combinations might affect the glycemic index of combination meals, hence their effect on weight as a whole, and waist circumference in particular,25,26 which in turn will have an effect on the risk of type 2 diabetes mellitus.27 Misconceptions and lack of knowledge is wide spread as seen in our results. The very common practice of drinking tea after meals might be one of the main contributors to the high prevalence of iron deficiency anemia in our community, with its associated poor work productivity and school performance. In addition, the fact that a high percentage ( 62%) of the sample did not know the truth about drug-food interaction, might partially explain the noted decreased efficacy of drug regimen prescribed by doctors resulting in poor control of chronic diseases such as diabetes, hypertension and dyslipidemia and reported in literature.28-31 Nutritional knowledge was affected by gender, and educational attainment, with females, and participants having ≥ secondary school certificate obtaining a higher mean score in knowledge section compared to males (P= 0.007), and participants with lower educational qualifications (P= 0.01) respectively. However, age affected certain parts of the knowledge section, with a higher percentage of participants ≥ 40 years of age believing in traditional taboos. This is expected, since younger people are less likely to cling to tradition. Gender differences were obvious in attitude and practice also, with a higher percentage of males admitting to mixing between foods thought to cause ill effects, and reporting that they did not stop this behavior after experiencing symptoms of ill health. On the other hand, age difference was obvious in the preference of younger age groups to consult health professional when faced with symptoms. In addition, both age and gender had an impact on source of knowledge for participants, with the older age group obtaining their knowledge unintentionally mainly through social gathering, compared to intentional seeking for information through the media, internet, or simple books by younger generation, especially females. It was also disappointing to find that only a small percentage of participants; mainly females; resorted to professional guidance. Our results can be explained by the fact that nutrition as a science is newly introduced to the Saudi public through the media mainly, with no formal nutrition education teaching being carried out in schools. At university level, it is only studied at specialized colleges for female students mainly, thus the higher awareness amongst female participants. Moreover, females tend to be more conscious about their appearances generally; especially when they work; needing to fit in with the latest image trends. Even though this is advantageous in a way, but without adequate knowledge and professional guidance, it could lead to poor health effects to themselves, and to their off springs as reported in literature.32 In conclusion, nutritional knowledge about food interactions is poor. Folklore is the main source. This might be a contributing factor to the increased prevalence of anemia and osteomalacia in our population. Therefore, professionally designed nutrition education programmes must be introduced early in life through school, and later through the media to modulate food habits in order to combat nutrition related diseases. The task maybe difficult, but not impossible. Indeed, in many countries the current staple foods are not the same as those eaten even a century ago, and rice was not indigenous to the gulf countries, yet it is now the major food staple in our region. Our study has its limitations, with method of collecting data being the main one. However, it provides information to a poorly researched area, and help to guide future nutrition education programmes.
References
- Micronutrient deficiencies: Iron deficiency anaemia [http://www.who.int/nutrition/topics/ida/en/]
- Micronutrient deficiencies: Vitamin A deficiency [http://www.who.int/nutrition/topics/vad/en/]
- UNICEF: Global Report. Investing in the future: A united call to action on vitamin and mineral deficiencies 2009.
- Al-Othaimeen AKO, Sadaa Al Orf, Abdulaziz: Prevalence of nutritional anaemia among primary school girls in Riyadh City, Saudi Arabia. International journal of food sciences and nutrition 1999, 50:237-243.
CrossRef - Al Hifzi I, Pejaver R, Qureshi I: Screening for iron deficiency anemia in a well baby clinic. Annals of Saudi medicine 1996, 16:622-624.
CrossRef - Al Hassan NN: The prevalence of iron deficiency anemia in a Saudi University female students. Journal of Microscopy and Ultrastructure 2015, 3:25-28.
CrossRef - Bahijri S: Serum zinc in infants and preschool children in the Jeddah area: effect of diet and diarrhea in relation to growth. Annals of Saudi medicine 2015, 21:324-329.
CrossRef - Al Senaidy AM: Brief report. Serum concentration of retinol, β-carotene, cholesterol, and triglycerides in Saudi school children. Journal of tropical pediatrics 2000, 46:163-167.
CrossRef - Al-Saleh I, Billedo G, El-Doush I, Mohamed GE-D, Yosef G: Selenium and vitamins status in Saudi children. Clinica chimica acta 2006, 368:99-109.
CrossRef - Alissa EA, Bahjri SM, Al-Ama N, Ahmed WH, Starkey B, Ferns GA: Dietary vitamin A may be a cardiovascular risk factor in a Saudi population. Asia Pacific journal of clinical nutrition 2005, 14:137.
- Bahijri SM: Serum 25-hydroxy cholecalciferol in infants and preschool children in the Western region of Saudi Arabia. Etiological factors. Saudi medical journal 2001, 22:973-979.
- Sedrani S, Al-Arabi K, Abanmy A, Elidrissy A: Vitamin D status of saudis III. Prevalence of inadequate plasma 25-hydroxyvitamin D concentrations. Saudi medical journal 1992, 13:214-219.
- Alsuwaida AO, Farag YM, Al Sayyari AA, Mousa DH, Alhejaili FF, Al-Harib AS, Housawi AA, Mittal BV, Singh AK: Prevalence of vitamin D deficiency in Saudi adults. Saudi medical journal 2013, 34:814-818.
- Abbag FI, Abu-Eshy SA, Mahfouz AA, Al-Fifi SA, El-Wadie H, Abdallah SM, Musa MG, Devansan CS, Patel A: Iodine-deficiency disorders in the Aseer region, south-western Saudi Arabia: 20 years after the national survey and universal salt iodization. Public health nutrition 2015, 18:2523-2529.
CrossRef - SandstroÈm B: Micronutrient interactions: effects on absorption and bioavailability. British Journal of Nutrition 2001, 85:S181-S185.
CrossRef - Power H, Heese H, Beatty D, Hughes J, Dempster W: Iron fortification of infant milk formula: the effect on iron status and immune function. Annals of tropical paediatrics 1990, 11:57-66.
CrossRef - Bobroff LB, Lentz A, Turner RE: Food/drug and drug/nutrient interactions: what you should know about your medications. University of Florida Cooperative Extension Service, Institute of Food and Agriculture Sciences, EDIS; 1999.
- Hulshof K, Wedel M, Löwik M, Kok F, Kistemaker C, Hermus RJ, Ten Hoor F, Ockhuizen T: Clustering of dietary variables and other lifestyle factors (Dutch Nutritional Surveillance System). Journal of Epidemiology and Community Health 1992, 46:417-424.
CrossRef - Martinez-Gonzalez M, Lopez-Azpiazu I, Kearney J, Kearney M, Gibney M, Martinez J: Definition of healthy eating in the Spanish adult population: a national sample in a pan-European survey. Public Health 1998, 112:95-101.
CrossRef - al-Nuaim AA, Bamgboye EA, al-Rubeaan KA, al-Mazrou Y: Overweight and obesity in Saudi Arabian adult population, role of socio-demographic variables. J Community Health 1997, 22:211-223.
CrossRef - World Health Organization. Noncommunicable Diseases and Mental Health Cluster. Surveillance Team.: STEPS instruments for NCD risk factors (core and expanded version 1.4) : the WHO STEPwise approach to Surveillance of noncommunicable diseases (STEPS). Geneva: World Health Organization; 2001.
- Al-Quwaidhi A, Pearce M, Critchley J, Sobngwi E, O’Flaherty M: Trends and future projections of the prevalence of adult obesity in Saudi Arabia, 1992-2022/Tendances et projections de la prévalence de l’obésité chez l’adulte en Arabie saoudite, 1992-2022. Eastern Mediterranean Health Journal 2014, 20:589.
- Hurrell RF, Reddy M, Cook JD: Inhibition of non-haem iron absorption in man by polyphenolic-containing beverages. British Journal of Nutrition 1999, 81:289-295.
- Ohta A, Ohtsuki M, Baba S, Adachi T, Sakata T, Sakaguchi E: Calcium and magnesium absorption from the colon and rectum are increased in rats fed fructo-oligosaccharides. J Nutrition 1995, 125:2417-2424.
- Du H, van Bakel M, Slimani N, Forouhi N, Wareham N, Halkjaer J, Tjønneland A, Jakobsen MU, Overvad K, Schulze M: Dietary glycaemic index, glycaemic load and subsequent changes of weight and waist circumference in European men and women. International journal of obesity 2009, 33:1280-1288.
CrossRef - Romaguera D, Ängquist L, Du H, Jakobsen MU, Forouhi NG, Halkjær J, Feskens EJ, Masala G, Steffen A, Palli D: Dietary determinants of changes in waist circumference adjusted for body mass index–a proxy measure of visceral adiposity. PLos one 2010, 5:e11588.
CrossRef - Sakurai M, Nakamura K, Miura K, Takamura T, Yoshita K, Morikawa Y, Ishizaki M, Kido T, Naruse Y, Suwazono Y: Dietary glycemic index and risk of type 2 diabetes mellitus in middle-aged Japanese men. Metabolism 2012, 61:47-55.
CrossRef - Khattab M, Khader YS, Al-Khawaldeh A, Ajlouni K: Factors associated with poor glycemic control among patients with type 2 diabetes. Journal of diabetes and its complications 2010, 24:84-89.
CrossRef - AlSaggaf W, Asiri M, Ajlan B, Afif AB, Khalil R, Salman AB, Alghamdi A, Bashawieh O, Alamoudi A, Aljahdali A: Reported Benefits of Insulin Therapy for Better Glycemic Control in Type 2 Diabetic Patients—Is This Applicable in Saudi Patients? Clinical Medicine Insights Endocrinology and Diabetes 2016, 9:13.
- Saeed AA, Al-Hamdan NA, Bahnassy AA, Abdalla AM, Abbas MA, Abuzaid LZ: Prevalence, awareness, treatment, and control of hypertension among Saudi adult population: a national survey. International journal of hypertension 2011, 2011:135-174.
- Alavudeen SS, Dhanapal C, Khan NA, Al Akhali KM, Paulliah SD: Prevalence and control of cardiovascular risk factors among type 2 diabetes mellitus patients in southern region of Saudi Arabia. Journal of Young Pharmacists 2013, 5:144-147.
CrossRef - Pugliese MT, Weyman-Daum M, Moses N, Lifshitz F: Parental health beliefs as a cause of nonorganic failure to thrive. Pediatrics 1987, 80:175-182.





Web of Science Coverage
Emerging Sources Citation Index (ESCI)
2024 Journal Impact Factor: 1.1
Scopus Journal Metrics
CiteScore 2025: 2.6
CiteScore Details
Sustainable Nutrition: Food Systems, Nutrient Retention, and Public Health Impact
![]()
This journal is a member of, and subscribes to the principles of, the Committee on Publication Ethics (COPE)








