Introduction
Undernutrition continues to afflict 180 million children worldwide and is responsible for in excess of 3.5 million maternal and child deaths each year. Until recently malnutrition was a neglected issue. However, it has recently begun to rise up the political agenda [http://www.ids.ac.uk.August12/2013]. Maternal and child undernutrition account for 11% of the global burden of disease [Black et al., 2008]. Globally, about one in four children of under 5 years old are stunted (26 per cent in 2011). An estimated 80 per cent of the world’s 165 million stunted children live in just 14 countries. Ethiopia is among 14 countries with the largest burden and highest prevalence of stunting [UNICEF, 2013]. In Ethiopia between 2000 and 2011 the prevalence of both underweight and stunting has declined to 32 and 23 percent respectively. The country needs to accelerate efforts to reach the Health Sector Development Plan’s target of reducing the prevalence of stunting to 30 percent by 2015 [FMoH, 2008; GOE, 2013].
In order to prevent malnutrition in children, family and community should be the first line of protection. Community-Based Nutrition (CBN) aims to build up the capacity and the ownership of communities and families to make informed decisions on child care practices [FMOH, 2008; FMOH, 2011]. CBN is an important component of the National Nutrition Program (NNP), designed to build upon the Health Extension Program (HEP) packages to improve nutritional status of under-five children and pregnant and lactating women. CBN was implemented in different phases in Ethiopia [FMOH, 2013]. Although there has been a marked improvement in the level of malnutrition in the country, child malnutrition is still prevalent according to the Ethiopia Demographic and Health survey (EDHS) of 2011. The prevalence of stunting was 44% among children 6 – 59 months, underweight was 29% and 10% children were wasted [DHS, 2011].
CBN supports improved quality and coverage of a number of preventive and promotive activities of CBN at the community level, including: monthly growth monitoring and promotion for under-two children; monthly community dialogues to engage community members in assessing and improving nutrition; quarterly screening of under-five children and pregnant and lactating women for malnutrition (with linkages to targeted supplementary food where available); improving referral practices; and six-monthly campaigns of Vitamin A supplementation and deworming for children 6-59 months [FMoH, 2008; 2011].
As part of this programme shift, CBN training modules have been shortened and incorporated into the Integrated Refresher Training (IRT). IRT is a new model which is developed by Federal Ministry of Health for delivering in-service training to health extension workers (HEWs) that could be able to implement the health extension packages including the former CBN training module. The community based nutrition components of the IRT include: maternal nutrition (MN), breastfeeding, complementary feeding (CF), and growth monitoring and promotion (GMP) and community health days (CHD) [FMOH, 2011]. The nutrition components of IRT not been evaluated so far; so this study will help to improve the component by identifying the gaps and opportunities. Therefore, the current study aimed to assess quality of CBN components of integrated refresher training and stakeholder perceptions on the quality training and change in health extension workers (HEWs) knowledge in Amhara Region.
Materials and Methods
Study areas
The study was conducted in randomly selected four woredas of Amhara region. Amhara region is located 9°-14° N and 36°-40°E in Ethiopia’s Northwest. The state shares common borders with the state of Tigray in the north, Afar in the east, Oromiya in the south, Benishangu-gumuz the south west and the Republic of Sudan in the west. The State of Amhara covers an estimated area of 170,752 square kilometres. According to the 2007 census, the region’s population was 17,214,056 of which 50.2% were males and 49.8% females. About 85% of the people are engaged in agriculture. The State is one of the major Teff (staple food) producing areas in the country. Barley, wheat, oil seeds, sorghum, maize, wheat, oats, beans and peas are major crops produced in large quantities [CSA, 2008].
Methods
Institutional based cross-sectional study design was employed. Data was collected from June to July, 2012. Both qualitative and quantitative data were collected. Observations were conducted during IRT training sessions and field practices. Pre and post training test were administered to participants to evaluate their knowledge change after training. In-depth interviews (IDIs) were conducted with selected trainees and master trainers (MTs) from each of the training session. A total of 139 HEWs and 22 master trainers (MT) were involved in the study. The quantitative data exported from Epi-Info were analyzed using SPSS version 17.0. Paired sample t-test was used to see knowledge gainedafter training. HEWs perceptions of training and observations of training by the research team were summarized as a measure of quality of training. Qualitative data from IDIs was reported in the pre-established themes on the quality of training, barriers and facilitating factors to delivering the training as planned.
Instrument, measurements and variables collected
In-depth interviews were conducted by researchers who were received training on the instruments and assistant by a note taker and digital tape recorder. Moreover observations were also conducted during training sessions. Pre-test and post test questions, composed of all CBN components were prepared. Indicators were: observation in training session, structured tests, perception of both MTs and trainees.
Results and Discussion
Observations and participants’ perceptions on breast feeding training session.
Breast milk is the only food or drink that a newborn child needs in the first 6 months
of his/her life. Exclusivity is a measure of the amount of breastfeeding without supplementation (e.g., infant formula or other breast milk replacements), and 6 months of age is a key marker since complementary foods (i.e., solids) usually begin around 6 months postpartum [WHO, 2011; BCC, 2006]. A shorter duration of exclusive breastfeeding does not protect infant growth so well as exclusive breastfeeding for six months does [WHO and UNICEF, 1998]. Moreover, the early introduction of complementary foods shortens the duration of breastfeeding, interferes with the uptake of important nutrients found in breastmilk and reduces the efficiency of lactation in preventing new pregnancies [Zeitlin and Ahmed, 1998; Oski and Landaw, 1980; Bell et al., 1987].
Around half of MTs said that training was delivered based on the manual as designed; they explained it in a good way and the facilitator guided to do so. On the other hand, the remaining half of them said that there was shortage of time to strictly follow each and everything listed in the manual which made some of them rush, others skip some exercises and the rest push the session in order to finish the breast feeding part. Some (5) MT of them explained as they were not using breast models and dolls. Moreover, they explained that more time should be given for the topics like breast attachment, positioning and expressing breast milk by mentioning that it is a new practice for rural community.
Master trainers from Ebinat woreda responded:
“The use of audiovisuals for the session makes the training very practical. There was breastfeedingvideo. We thought it is better if the training is supported by audio-visual. Actually that thing is not included in the training materials. However I have an idea that it is better if it is included in the content.”
In contrary to this most of the trainees said that the training they received on breast feeding is enough. They have mentioned different reasons; they stated that they have got enough skill to apply it practically in the community, some said it is the right way to address the available gaps in the community, others said it is easily understandable and they trained well. Some said the training on breast feeding (BF) is not enough. They reasoned out that shortage of materials like breast model and doll have made the training difficult to understand the training on attachment and positioning. They also said it was more of theoretical or absence of practical session/demonstration which is the other shortcoming of the training.
Health Extension worker from Meket woreda said:
“Expressing breast milk was not enough as it was very uncommon in our community. Even it is not clear for me. Since it is related with bottle feeding, it needs additional and improved training. So more time must be given for this section and we ourselves are lactating and we can practice it. I tried it last night but I can’t because I didn’t practice it here.”
This was also observed in IRT sessions where MTs used 20 additional minute on average than allocated time for breast feeding session. As observed in the four sessions, use of more time than allocated in the above specified topic could be due to insufficiency of the allocated time to do all exercises in separate groups and discussing it with the larger group. In addition, on average 65 % of BF session was fully delivered with two way communications. The reason why the rest part of the session was not fully delivered might be of MTs rush to finish the sessions on time and MTs thought that participants already know the messages.
Even though more than 60% of the trainees said the training on BF was adequate to give services to the community and significant knowledge gained (p<0.05) on breast feeding was seen by participants after the training, it was observed that they failed to give all the appropriate advice related to breast feeding during the field practice. This could be due to shortage of time given for the field practice which made them not to follow all the procedures and the MTs were not supervising and giving feedback for them. The classroom practical session was not properly done as per the guideline which could be the other reason.
Observations and participants perceptions on complementary feeding trainingsession.
Complementary feeding (CF) is the process of giving other foods and liquids in addition to breastmilk. Complementary foods can be especially prepared for the infant or can be the same foods available for family members, modified in order to meet the eating skills and needs of the infant [IASC,2009; Monte and Giugliani, 2004].The impact of feeding practices on nutritional status, growth, development, and health outcomes of infants and young children are well documented. The critical window for improving child nutrition is from pregnancy through the first 2 years of life, a period when the transition is made to CF [IASC, 2009].
Most (15) MTs said that they delivered the training based on the manual and they reasoned out that it was scheduled and prepared in a way that HEWs could understand. However, some (5) MTs mentioned that there was time shortage which obliged them to give some topics as a reading assignment and rush on some topics that they thought HEWs have a good understanding.
Master trainers from Gidan woreda responded:
“It is not possible to say delivered as it was designed; this was mainly because of shortage of time. If we think to deliver it as to the manual we would not be able to cover the portions. That’s why some times we gave more time to new topics by reducing some time from the topics which we consider trainees would have a better understanding.”
Other MTs also explained that there was difficulty in strictly following the manual. Their reason was shortage of participant manual and family health cards (FHCs) as a result they were using the old FHC to fill the gap.
In addition, some (5) MTs mentioned the importance of having a poster that contains the procedures of complementary food preparation. Complementary food session didn’t contain adequate information on iodized salt utilization and they suggested that information regarding the importance of iodized salt utilization should be included in this session since the utilization especially in their community was poor.
Master trainers from Regional health office stated as:
“When we demonstrate the food preparation, we had material problem. For e.g. the materials for food preparation are not included in the training package. We prepared the cooking materials and food stuffs available in the area by our own initiation. I think it will help to give the training easily if these things are included in the package.”
MTs were rushing and skipping some exercises to finish the session and use of extra time was observed in sessions; on average additional 13 minutes to the allocated were used. This was noted while observing the sessions, where 59% of the CF sessions were delivered all messages under the sub-topics with two way communication. This shows that in order to finish sessions on time MTs were not delivering all the messages as designed. Although most trainees mentioned that the training they received on CF was adequate and significant knowledge change was seen (p<0.001), gaps in delivering appropriate message about CF for the caregiver were observed during the field practice. This could be due to the fact that enough time was not allocated for the field practical session on which only half day was allocated for growth monitoring, inter personal communication with caregiver, conducting community conversation and demonstration of complementary food preparation [FMOH, 2011]. The other reason might be that less facilitators’ involvement in following up the trainees during field practice.
Observations and Participants perceptions on growth monitoring and promotion training session
Community-based growth and monitoring programs is one of the short-route responses to reduce the prevalence of malnutrition. In order to detect cases of malnutrition and associated illnesses, monthly measurements of children’s weight growth are recorded and compared to previous records and plotted on a chart against an international reference population. The linear growth retardation acquired early on infancy can’t be easily reversed after the second year of life [Monte and Giugliani, 2004; UNICEF, 2004].
Though most (14) MTs complain time shortage for delivering GMP session as designed, in all the observations it was finished on average 15 minutes earlier. This could be due to all woredas didn’t practice proper weighing. Preparation of weighing basket was also not done in all sessions except one woreda. Furthermore, interpreting weight gain and nutritional status determination were skipped in two woredas and it was observed that per session, on average 55 % of GMP messages were delivered as designed (all messages with two way communications). This shows that skipping exercises might be the reason for the sessions on GMP to be finished early.
More than half interviewees said the training was not enough due to different reasons. They said that additional training is needed as they didn’t get adequate knowledge. Shortage of time was the main problem raised. They were not able to do the practical weighing and plotting exercise due to time shortage. They also said that, they need more training on interpretation of the result after plotting.
Health Extension worker from Gidan woreda responded that:
“For example in the area where I am working there is no separate growth chart for the two sexes; but what I observed here was in blue and red colors. So, it needs additional explanation why we needed to put them separately.”
Although there was significant knowledge gained statistically (p<0.05), the trainees answered only half of the questions correctly on post test. This could be as a result of skipping practical exercises and not delivering all messages as designed. And again, in the field practices most failed to appropriately weigh a child and determine its nutritional status, though most trainees replied that the training they received on GMP was adequate. Since in some places trainees didn’t even get the chance to practice weighing a child as the MTs were doing it themselves, this might have effect on delivering the service to community.
Some HEWs were confused with new information in the manual especially on children who are eligible for growth monitoring and didn’t want to stick to the new.
Master trainers from Regional health office responded:
“Even though we gave the training based on the manual, there was conflicts among participants and facilitators concerning to the age of children eligible to GMP (2 or 3 years).The manual clearly shows that the age of child for GMP should be under 2 years but most of the HEWs resist this and have a tendency to follow the previous trend i.e. under 3 years. They thought their immediate boss should order them to practice them based on the new manual.”
Almost all MTs complain on the time allocated to this session; they said that the session contains important and practical topics which HEWs expected to do independently in the community but the time allocated for the topics were not adequate to deliver the training by ensuring each participant understands everything. Understanding the invisible malnutrition, properly weighing a child, plotting a child’s weight on the growth chart, interpreting growth trend and discussing the issue with the mother were frequently mentioned topics which need more time in order to have better understanding. Some MTs supported this suggestion and said that practical exercises were skipped due to shortage of time and as a result most of the participants were unable to perform the growth monitoring and community conversation activities during field practice.
Furthermore some MTs recommended that the GMP exercise presented as table in the manual, and the interpretation of growth trend in graph 3 should be revised as it created confusion and they also stressed that the material of weighing basket should be again modified as it was not comfortable for the children during weighing. Shortage of training materials like family health card and participant manual were mentioned and suggested to be solved in the future before conducting training.
Observations and Participants perceptions on maternal nutrition training session
Maternal and child undernutrition account for 11% of the global burden of disease.
Maternal nutrition refers to the nutritional needs of women during the antenatal and postnatal period (i.e., when they are pregnant and breastfeeding) and also may refer to the time period before conception (i.e., adolescence).Maternal undernutrition affects the health of both mothers and children and, as a result, has broad impacts on economic and social development. Undernourished pregnant women have higher reproductive risks, including death during or following childbirth [Black et al., 2008; MGUR, 2012]. Study shown that maternal and child undernutrition (maternal height, birth weight, intrauterine growth restriction, and weight, height and body mass index (BMI) at 2 years according to the new WHO growth standards) were related to adult outcomes (height, schooling, income or assets, offspring birth weight, BMI, glucose concentrations, blood pressure) [Victoria et al, 2008].
The perception of MTs on maternal nutrition was more or less similar; they all explained that they delivered the training according to the manual and pointed out that it would be better if put separately just like other components of the nutrition. Their complaint was not only on how the section was organized but also the detail and clarity of the contents included in it. According to their opinion, lacteal feeds and food taboos were not presented in detail and might not be sufficient for the trainees to teach the community. They explained that the manual mentions only the type of foods which are accepted and not accepted culturally but it didn’t put clearly why some of them are accepted and others are prohibited. This deficiency made them to think two different things: the first was, to perceive as the manual didn’t consider the reality that health and growth of a child fully relies on the condition of a mother and the other was, to think ways of addressing these gaps. In this regard, they reported that they made a thorough discussion using their own experiences and some examples: “We explained what types of foods were prohibited, why prohibited and in what way they could change the communities’ attitude.” (MT).
Nearly half of the MTs explained that even if they gave the training according to the manual they had faced some challenges due to shortage of time and unavailability of some materials. As they explained, neither the theoretical nor the practical session had been allocated sufficient time, and because of this, they were forced to deliver only basic points, simply by telling trainees to cover the rest by themselves:
Master trainers from Ebnat woreda said:
“We convey only key massages and left others as a reading assignment.”
Due to these reasons, they were not confident to say that trainees would bring the desired behaviour at the community level.
Majority of the trainers reported that they had no adequate knowledge on Outpatient Therapeutic Feeding Program (OTP) services. They told that they were confused with what the manual says and the reality on the ground. In the manual there are eligibility criteria’s for pregnant and lactating woman to get OTP services, but, because of budget constraint and lack of knowledge it is uncommon to give this service. MTs also indicated that none of the HEWs knew how the service should be given.
On the contrary, few MTs told that the manual has sufficient time and detailed contents; to them, it has a lot of exercises, and training was delivered in a participatory and explanatory way.
Observations and participants perceptions on community Health Day training session.
In this section trainers were asked to tell whether they gave training according to the manual or not and to explore possible reasons which made them not to provide according to the manual. Almost all MTs told that they take the training according to the manual even if shortage of time was the main problem to them. Most of those MT told that this shortage was mainly during practical sessions.
Another master trainers from East Estie woreda responded:
“To dig out everything and solve the problems, there wasn’t enough time. There were argumentative ideas raised. So this needs more time. Caring for malnourished children by itself needs more than an hour. The time given for practical part was very short and even not enough to explain the points.”
When asked about the delivery of messages with respect to the sequences put in the manual, trainers cited a range of reasons why they skip and not keep the sequence in some portions. Most of them asserted that they were themselves trained in this way and the assumption that trainees already knew and practiced it.
Master trainers from Meket woreda said:
“We were just applying what we have been trained in training of trainers. That’s why we go to the particular community getting full information about the pertaining problems in that area. In today’s session, for instance: first we gathered information about the number of children weighed and their nutritional status from the last month registry of the health post. Having this information, we just began the session with counselling.”
Few of the interviewees also raised the need for hiring of additional HEWs because some of those who already received the training are leaving to other places.
“There should be additional HEWs because nowadays HEWs are migrating to other places.”(MT from Regional health office).
The others were in doubt of the health extension workers ability to carry out this work independently in their work places.
“What we understood from this section is most HEWs are unable to carry out independently in their work places. They need support from someone else whenever there is community health days.” (MT from Meket woreda).
Majority of the trainers described that the training was highly affected by shortage of materials. As a result, they were not able to show some procedures.
“That is because we don’t have the materials. We have asked but only albendazole, vit A and MUAC tape was found. We have asked tally sheet and registration book, it is but there isn’t any.” (MT from Estie woreda).
Training adequacy for non-CBN Areas
Most interviewees indicated that the training was not enough for those who had no previous CBN exposure. According to the trainers, this was clearly observed when they were receiving training of trainers (TOT) with those who had already trained CBN.
Change in Knowledge of trainees.
This study was aimed to assess change in knowledge of participants. They were given pre-test before the training and post test after the training. The trainees were given four days training by master trainers on CBN components (breastfeeding, complementary feeding, growth monitoring and promotion, maternal nutrition and community health day at woredas level). Paired t-test was used to see the knowledge change and was found to be statistically significant. The mean pre-test score for breastfeeding was 5.19 and post test score 5.31, which indicated an increase of 0.12 over pre-test score (Table 1). The result of this study also showed there were 0.96 increment observed in CF i.e., the mean pre-test score for CF was 4.01 and it was 4.97 for post-test. The result of GMP showed that there was 0.69 increments after intervention. In this study there is significant change in knowledge of training given in breastfeeding and community health day (p<0.05). There is a highly significant change in knowledge in the complementary feeding and growth monitoring and promotion components (P<0.001); however, there is no statistically significant change in knowledge observed in training that was given on maternal nutrition (P>0.05) (table 1).
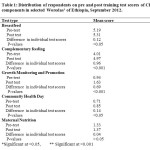 |
Table 1: Distribution of respondents on pre and post training test scores of CBN components in selected Woredas’ of Ethiopia, September 2012. Click here to View table |
Health Extension workers perceptions on the quality of training.
HEWs were interviewed to assess their perception on quality of training. More than half of the study subjects responded that training was given in the components of CBN was the right amount. Whereas about quarter of trainees perceived that they need more training on CF, BF, GMP, MN and CHD to understand the subjects (table2).
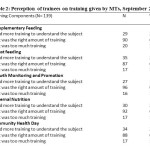 |
Table 2: Perception of trainees on training given by MTs, September 2012. Click here to View table |
Field practices
Field practices were done in all four woredas where nutrition part of IRT sessions observed. In all field practice sessions; details on what must be done, when and how, was informed for participants before going to the field. Facilitators and co-facilitators were selected in all sessions except in one woreda. The communities were informed about the field practice prior to the date of practice but they were not divided in to two gottes (peasant association) in all sessions. On the other hand, use of community growth charts were observed only in the practical session conducted at one woreda. In addition inadequacy of FHCs and unavailability of checklist to follow the community conversation were noticed in all the four practical sessions.
One participant was expected to weigh a child and do the inter-personal communication with the care taker; however a group of 3 to 4 participants were weighing one child and doing the inter-personal communication except in one woreda where weighing a child was done by the master trainers. The reason mentioned was only few children were available at the time of field practice and surprisingly only 3 children were weighed in the field practice held at one (Estea) woreda.
Among 21 children, who were observed during growth monitoring at the field practice of all sessions, all procedures of weighing were followed only for 7 of them. In addition all the appropriate advices were delivered for none of the care takers. Correct age and nutritional status determination was done only for 14 and 11 respectively (table 3). Of the four field practice sessions observed, community conversation (CC) was conducted on the 3 woredas but not in one woreda as only 3 care takers were available at the time of field practice. However all community conversations in the three practical sessions were not conducted properly.
 |
Table 3: Activity done by participants at the field practice of all sessions, September 2012 Click here to View table |
Conclusion and Recommendations
In conclusion; the training that were given in four selected woredas were not quality wise and as designed. The IRT of nutrition component lack reporting and monitoring format.The nutrition component of IRT training manual should be revised based on the finding. The time allocated for all CBN component were not adequate, in all nutrition components the allocated time for training should rearranged. Reporting format and monitoring evaluation should be added in revised training manual. There should be training for the health extension workers with more number of days by considering new CBN woredas.
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
MT conceived the idea and designed the study, coordinated data collection, transcribed qualitative data, performed analysis, interpretation of data and drafted the manuscript. TA coordinated data collection, interpreted data analysis and critical review and commented on the manuscript. AS conceived the idea, obtained funding, helped in the data collection instrument development, assisted in data collection and manuscript writing, and critically commented on the draft manuscript.TH, DK and AK commented on the draft manuscript. All authors gave final approval of the version to be published.
Acknowledgements
We are highly grateful to Ethiopian Health and Nutrition Research Institute, for the timely review, comments, and clearance of the study. This study was financially supported by World Bank through Federal Ministry of Health, we would like acknowledge the support from the World Bank. We would like to extend our appreciation to Federal Ministry of Health, Regional, Zonaland Woreda Health Offices for providing the necessary information and facilitating conditions while carrying out this study. We are also very grateful to extend our appreciation to the study participants who share their priceless time.
References
- http://www.ids.ac.uk/idsresearch/nutrition#sthash.sA3HxCl6.VKOdDRvK.dpuf. August12/2013.
- Black, R.E.; Allen, L.H.; Bhutta, Z.A. et al. Maternal and Child Undernutrition Study Group (2008). ‘Maternal and Child Undernutrition: Global and Regional Exposures and Health Consequences’, Lancet 371.9608: 243–60.
CrossRef - United Nations Children’s Fund (UNICEF). April 2013. Improving child nutrition. The achievable imperative for global progress.April 2013.
- Independent Review Team. Ethiopia Health Sector Development Program (HSDP-III) (2005/06-2010/11) Mid-term review. FMOH. Vol. I Component Report. 2008: Addis Ababa.
- Government of the Federal Democratic Republic of Ethiopia. National NutritionProgramme,June 2013 – June 2015.
- Federal Ministry of Health July, 2008. Programme implementation manual of national nutrition programme, July 2008–June 2013
- Federal Democratic Republic of Ethiopia Ministry of Health2011. Integrated Refresher Training for Health Extension Workers, Module II (CMNCH) – Facilitator Guide.2011.
- Central Statistics Agency [Ethiopia] and ICF International. 2012. Ethiopian Demographic and Health Survey, 2011.Addis Ababa, Ethiopia and Calverton, Maryland, USA: Central Statistics Agency and ICF International.
- Federal Democratic Republic of Ethiopia Population census commission. 2008. Summary and statistical report of population and housing census.2008.
- World HealthOrganization: Exclusive breastfeeding. Geneva, Switzerland: WHO; 2011. http://www.who.int/nutrition/topics/exclusive_breastfeeding/ en/index.html.
- Breastfeeding Committee of Canada (BCC): Breastfeeding definitions and data collection periods. Ottawa, Canada: The Breastfeeding Committee for Canada; 2006. http://breastfeedingcanada.ca/documents/.
- WHO/UNICEF. Complementary feeding of young children in developing countries: a review of current scientific knowledge. Geneva: World Health Organization, WHO/NUT/98.1,1998
- Zeitlin MT, Ahmed NU. Nutritional correlates of frequency and length of breastfeeding in rural Bangladesh. Early Hum Develop. 1995;41:97-100.
CrossRef - Oski FA, Landaw AS. Inhibition of iron absorption from human milk by baby food. Am J Dis Child. 1980;134:459-60.
CrossRef - Bell JG, Keen CL, Lonnerdal B. Effect of infant cereals in zinc and copper absorption during weaning. Am J Clin Dis Child. 1987; 131:1128-32.
CrossRef - Inter –Agency standing committee (IASC). Complementary Feeding of Infants and Young Children in Emergencies.2009.
- Monte CM, Giugliani ER. Recommendations for the complementary feeding of the breastfed child. J Pediatr (Rio J). 2004;80(5 Suppl):S131-S141.
CrossRef - UNICEF, “Low Birthweight: Country, Regional and Global Estimates”, Unicef and WHO, 2004.
- The Manoff Group and University Research Co., LLC (MGUR). Guidance for formative research on maternal nutrition. February 2012.
- Victoria et al (2008). Maternal and Child Undernutrition 2. Maternal and child undernutrition: consequences for adult health and human capital. Published OnlineJanuary 17, 2008DOI:10.1016/S0140-6736(07)61692-4.
CrossRef

This work is licensed under a Creative Commons Attribution 4.0 International License.








