Effects of Nutrition Education on Nutrition Knowledge and Iron Status in Primary School Pupils of Gatanga District, Muranga County, Kenya
Department of Foods Nutrition and Dietetics, Kenyatta University, P.O.Box 43844-01000, Nairobi, Kenya.
DOI : http://dx.doi.org/10.12944/CRNFSJ.1.2.02
Download this article as:
![]()
School-age children are both growing and learning, and anaemia can affect cognitive function, motor performance and educational achievements of this age group. Nutrition education has not been given the priority it deserves in primary schools due to the busy school curriculum. It is in this light this study was designed for one teaching calendar year. Subjects & methods: Pupils (n=601) covering the age 11-18 years were included. The main objective of this study was to evaluate the effects of three main Nutrition Education strategies on nutrition knowledge and iron status among primary schools children in Gatanga district. A baseline survey was conducted in 12 randomly selected schools for class six pupils and their households. Questionnaires and an interview schedule were used to collect data, with pre and post tests. The interventions schools were Mabanda, Kigio and Kirwara (experimental) and Gakurari (control school). Baseline data were analyzed by use of Statistical Package for Social Sciences (SPSS) and Nutri-Survey computer packages using both descriptive and inferential statistics. The data were coded to search for emerging themes. This led to the identification of variables and concepts of iron deficiency in the children, which was crucial to the design of the corrective measures model for the interventions. On average the mean mark, in nutrition knowledge at baseline was 30.05%. In the post-tests all experimental schools (n=154) significantly improved in nutrition knowledge, and the peer facilitated school performed best with (51.52+24.79) marks, Researcher facilitated school (48.39+22.23) and the agriculture staff (38.70+9.87). The pre-test post- test improvement in the control school (31.21+12.74) was however not significant (p>0.05). A total of 31.4 % pupils ( Sub sample n=89) were found to be anaemic after altitude adjustments at a calculated factor 0.5 for Gatanga altitude (2237m ASL). Pupils’ haemoglobin status were not significantly different (p>0.05) between the experimental and control schools at baseline, notable differences occurred in the experimental schools after the interventions. Relationship between nutrition knowledge and nutrient intake was positive and there was a statistically significant relationship between nutrition knowledge and hemoglobin levels at p<0.05 (R2=0.253, p=0.025). Anemia was found to be a significant problem and therefore the need for a comprehensive intervention strategy by all stakeholders to improve the iron status in this age group.
KEYWORDS:Peers;Agriculture staff;Intervention;Gatanga pupils
Introduction
Iron deficiency anemia (IDA) is a problem of serious public significance and it is estimated that 60 million school-age children suffer from iron deficiency disorders whilst some 120 million suffer from iron deficiency anemia (The FRESH Framework, 2013). In young children it may impair physical growth, cognitive development, and immunity; in school-aged children it may affect school performance. Overall, global estimates show 46% of school age going children are anaemic (UNICEF, 2008). It is the only nutrient deficiency which is also significantly prevalent in industrialized countries (WHO, 2013). Iron deficiency anemia is a frequent laboratory abnormality in children. As many as 20% children in the United States and 80% children in the developing countries risk being anemic at some point by the age of 18 years (Ramzan et al., 2009). Different studies from Turkey have shown prevalence of anemia among school children by hemoglobin (Hb) concentration to be between 16.3% and 61.1% (Kaya et al., 2006).
In developing countries, half of all young children suffer from anaemia, often as a result of iron-deficiency. A study done in Cote d’Ivoire by Kakunted (2008) revealed 50% prevalence of anaemia in school children and women. Iron deficiency anemia affected 30% of school children in Egypt and was by far the most common nutritional Different studies from Turkey have shown prevalence of anemia among school children by hemoglobin (Hb) concentration to be between 16.3% and 61.1% (Kaya et al., 2006).disorder in a study by Ismail (2004). A study done in the year 2009 in Zanzibar on iron status found that overall, 62.3% of children were anaemic (hemoglobin < 110 g/L), and 82.7% of anaemia was associated with iron deficiency (Stoltfus et al., 2001). The school years are therefore an opportune time to intervene, and interventions must be based on sound epidemiological understanding of the problem in this age group (Stoltzfus et al., 2001). According to data from localized surveys at least 33% of Kenyan children are anemic and that a large number of children are not able to enjoy their right to nutrition. Despite the importance of good nutrition and good health in childhood, there is a long-standing problem of guidelines and policies that address the issues of nutrition and health intervention and cost effective strategies for poverty reduction. Unacceptable levels of over-nutrition and under-nutrition in Kenya, including chronic under nutrition and micronutrient deficiencies, are responsible for high rates of illnesses and deaths nationally (KNBS, 2010). From the 1999 Kenya national micronutrient survey, iron deficiency was high with 43% of pre-school children and 42% of school going children suffering from iron deficiency. The prevalence of anaemia among pre-school children in Kenya stood at 73% while among school-aged children was 56% in a study by UNICEF (2009) and (MOPH&S, 2012). The regional distribution of anaemia among children in Central and Midwest Highlands of Kenya was 8.6-89.5% (UNICEF, 2009). Many children are anaemic due to food insecurity and poverty.
Schools provide a social context in which children learn and develop, thus making schools a desirable environment for nutrition education promotion (Gunde, 2004). Pupils spend a lot of time, over three quarters of the year in the school environment and therefore are in constant contact with the teachers and peers who are their main models. School children are at an exploratory learning stage, an opportunity that can be taken advantage of to instil positive behaviour, through classroom learning and hands on practical experiences. Habits and attitudes formed in early life are translated into the future adults’ lifestyles. It is therefore important that the school environment enable and reinforce healthful eating and health behaviours through behavioural –focused classroom instruction. It is, therefore, the school children who stand to gain the most through nutrition education strategies. The causes of IDA are not only known; but also solutions that are both inexpensive and effective are also available (WHO, 2007).
Iron deficiency anaemia is frequently exacerbated by infectious diseases like Malaria, HIV/AIDS and other sexually transmitted infections and hookworm infestation. Other infections such as tuberculosis are also important factors contributing to the high prevalence of anemia in some areas (MOE, 2007; WHO, 2013; WHO, 2007). Another cause is dietary intake based mainly on grains that contain anti- nutrients such as phytates that bind iron, and therefore not broken down in the gastrointestinal tract. The body absorbs only 5% of all the iron in plant food and the rest is excreted by the body (Andang’o et al., 2007). Children, who make up 50% of the total population, suffer varying but significant degrees of ill health, nutritional deficiencies and morbidity that unequivocally impede effective learning and realization of their full productive potential. The health consequences are devastating, invisibly eroding the development potential of individuals, societies and national economies. The main strategies for the prevention and control of micronutrient deficiencies are nutrient supplementation and food-based strategies of fortification and dietary diversification, deworming, malaria control, combined with nutrition education (Sifri et al., 2002). Nutrition education should target both the pupils and mothers/caregivers and should focus on good eating habits ( Kaya et al., 2006). In view of these facts this study aimed at determining the iron status of the pupils and designing a viable model for intervention to mitigate against the condition.
Materials and Methods
Study design: Experimental with pre and post-tests and preceded by a baseline survey. Ethical approval was given by Kenyatta University review ethical committee. Baseline study on follow up pupils’ to their households’ was undertaken for demographic and socio economics, food consumption and intakes whereby an interview schedule was used to collect data. Pre-tests questionnaires on nutrition knowledge were administered before embarking on the interventions. These included determination of the level of nutrition knowledge about the nutritive value of food, food sources, deficiency diseases, health and sanitation (hygiene and food safety), cooking methods and selection of iron rich foods. The assessment of iron, helminth and malaria status was done by a laboratory technician from Level 4, Kirwara Sub-District hospital of Gatanga on the first week of April 2012.The purpose of the study and the procedures for Hb, malaria and stool sample collection were explained to head teacher, senior teacher, the class teacher and the children in class six whose parents had signed the consent forms. Random sampling of boys and girls was undertaken to choose the sample required. Information about name, sex, age and sample numbers were recorded. The sample size for both boys and girls were similar since none of the girls said they had menarche. The gender specific sample size was determined based on discussions with the laboratory technician who suggested a greater sample size for females, than males if they had menarche since there is an established higher prevalence of anemia in menstruating females. Pubertal status was assessed by the status quo method: Female pupils were asked whether they had experienced menarche before the blood samples were taken and the males’ nocturnal emissions. None of them said they had menarche or emissions in both the pre-tests and post- tests.
Venous blood sample was drawn with a sterile disposable needle and syringe from the sampled pupils asceptically from antecubital veins of the arm and 2ml of blood was alliqotted into BD vacutainer tubes with K2E anti-coagulant (EDTA-sequestrene) after disinfections with methylated spirit swap and drying of skin. The tubes were then packed in a cooler box at 2-80C for about 6 hours and transported by a private vehicle to Level 4 Kirwara Sub-district hospital for analysis. The children were categorized as having iron deficiency anaemia when found with Hb <12g/dl for girls, and <13g/dl for boys of the specified ages based on WHO standards.
Intervention study
The intervention study was meant to address the gaps in the baseline findings to improve on the iron status of the school pupils. Five peer educators and the agriculture staff were trained by the researcher before embarking on teaching in the experimental schools on each topic in March/ April 2012 after the baseline study. This was meant to measure the effectiveness of each strategy in delivery of nutrition education messages. Flip charts for trainings in the intervention were developed by the researcher and validation done by the teachers. Deworming was done and hygienic practices were taught to pupils. Pupils are keen to learn from role models who can have a great influence in their eating habits. Nutrition education using the three strategies of the researcher, Agriculture extension officer and the peer educators was taught to intervention schools to among other things evaluate the effectiveness of each strategy. At each visit, facilitators determined whether each child from the baseline roster was present, absent, had left school, or had transferred to another school. Lesson plans showing the lesson organization and presentation were also made with guideline from the classroom curriculum chart and Class 5 and 6 Science books (FAO, 2005; Alex et al, 2010; Vasishta & Patel, 2002). More emphasis was laid on the importance of iron rich foods and how to produce and eat them. An end-term survey was undertaken to assess the impact of the intervention to follow-up pupils’ households. The dietary intake on 24hr dietary recall (taken twice and averaged), food frequency, dietary diversity score and technologies adopted were assessed at the household level for the follow-up pupils.
Results and discussion
1.Age of the primary school pupils’ in Gatanga district at baseline study
Age will help determine the nutrition education materials that are appropriate for teaching the pupils’ to enable them actively participate and retain knowledge and transfer it to others. Figure 4.1 shows distribution of Gatanga primary school pupils’ by age in years.
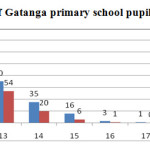 |
Figure 1: Distribution of Gatanga primary school pupils’ by age in years Click here to View figure |
Figure 1: Distribution of Gatanga primary school pupils’ by age in years
The age of the pupils in the 12 baseline schools in class six (6) ranged from 11 years to 18 years. Of these, 86.2% were 11-13 years, 12.7% were 14-15 years and 1.1 % was 16-18 years. The results reveal that at younger age (11 years) there were more girls than boys but after that there was a declination in enrollment for girls
2 Effects of the intervention
Nutrition knowledge was offered to all the experimental schools using the three strategies; Peers, agriculture extension worker and the researcher. It included classroom lessons on nutrition, cookery and kitchen gardening activities in the school. School gardens can help to improve the nutrition and education of the children and their families in both rural and urban areas. The gardens should include a variety of vegetables and small livestock like rabbits (FAO, 2005).
2.1. Performance in Nutrition knowledge before and after interventions
Learners were taught under the different strategies after the pre-test on various predetermined nutrition education topics. Table 1 shows the performance in nutrition knowledge before and after the interventions.
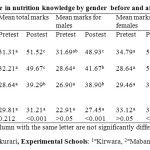 |
Table 1: Performance in nutrition knowledge by gender before and after the interventions Click here to View table |
Table 1: Performance in nutrition knowledge by gender before and after the interventions
The average mark in nutrition knowledge was 30.05% at pre-test and 46.8% in the intervention schools in the post-tests. In both pre & post-tests females did better than males. Post-tests showed a significant difference with the experimental schools performing significantly better than the control school at p<0.001. The performance of the control school also improved. The improvement may have been caused by the sensitization during the first testing and pupils may have tended to remember their responses during the second testing as cautioned by Mugenda and Mugenda (2003). The pre-test post-test improvement in the control school was however not significant (p> 0.05) as compared to the performance of the experimental schools.
3.Seven day food frequency & intake of selected iron rich foods before and after interventions
Various selected food groups were analyzed to compare their consumption pre and post intervention Table 2 shows pupils’ food frequency pre and post intervention.
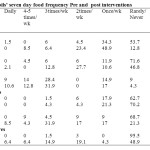 |
Table 2: Pupils’ seven day food frequency Pre and post interventions Click here to View table |
Table 2: Pupils’ seven day food frequency Pre and post interventions
There was improved consumption of some iron rich foods that included green leafy vegetables like amaranth and cowpea leaves by pupils and their households, though it was not statistically significant at p>0.05.
4. Mean nutrient intake from 24hr dietary recall by gender after intervention
Intakes may differ by gender due to various reasons. For example girls usually assist with cookery and hence may have higher intakes than the boys. Table 3 shows the pupils mean intake by gender post intervention.
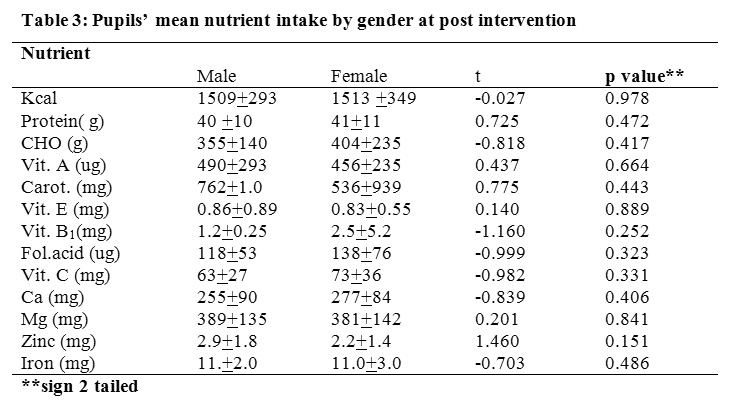 |
Table 3: Pupils’ mean nutrient intake by gender at post intervention Click here to View table |
Table 3: Pupils’ mean nutrient intake by gender at post intervention
Consumption of various nutrients was not statistically significant between both genders at P>0.05. The study period was favoured by a cool weather which influenced vegetable production with little watering hence higher consumption of various nutrients.
5. Mean haemoglobin levels before and after intervention
After the intervention the haemoglobin levels were compared pre and post intervention to establish if there was any change. Table 4 shows changes in mean haemoglobin levels of pupils’ pre and post intervention.
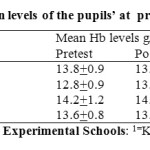 |
Table 4: Mean haemoglobin levels of the pupils’ at pre and post intervention Click here to View table |
Table 4: Mean haemoglobin levels of the pupils’ at pre and post intervention
Pupils haemoglobin status were not significantly different (p>0.05) between the experimental and control schools at baseline, notable differences occurred in the experimental schools after the interventions. In Kirwara where the peers were facilitating the mean Hb levels were 12.8g/dl before interventions and after the interventions the mean levels improved to 13.41g/dl. For Mabanda where the researcher was the facilitator the mean levels improved from 14.26 g/dl to 14.50g/dl, and Kigio where the Agriculture officer was the facilitator the levels improved from 13.50g/dl to 13.83g/dl. For the control school the Hb levels decreased from 13.70g/dl to 13.33g/dl. There was a negative statistically significant difference at p<0.001. There was a positive statistically significant difference in the haemoglobin levels in the peer facilitated school at p<0.05. Notable improvement occurred in the other two schools but was not significantly different at p>0.05.
6. Relationship between Nutrition knowledge of some selected topics and haemoglobin levels before and after interventions
The acquisition of nutrition knowledge may lead to improved nutritional status in this increased haemoglobin levels. Table 5 shows the relationship of nutrition knowledge and some selected topics and haemoglobin levels at pre and post-tests.
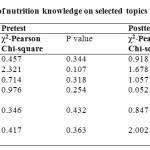 |
Table 5: Relationship of nutrition knowledge on selected topics and haemoglobin levels Click here to View table |
Table 5: Relationship of nutrition knowledge on selected topics and haemoglobin levels.
The results shows the selected nutrition knowledge topics were not significantly associated at p>0.05, but the associations were stronger at post-tests for all topics except the consumption of spinach.
7. The relationship among variables: Nutrition education, consumption of iron rich foods and the iron status of pupils’ across the three nutrition education strategies
Nutrition interventions are known to help in management of all kinds of malnutrition amongst the populations. Table 6 shows correlation between nutrition knowledge and selected variables after interventions.
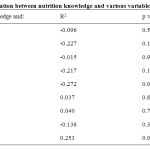 |
Table 6: Correlation between nutrition knowledge and various variables Click here to View table |
Table 6: Correlation between nutrition knowledge and various variables
Bivariate correlations (R2) explained the relationship between nutrition knowledge and selected nutrients at post-test. The relationships were statistically significant for some variables. Nutrition knowledge and various nutrient intakes as explained by Table 6 were not statistically significant. Nutrition knowledge and vitamin C intake improved at (R2= -0.272, p=0.068) and Hb (R2= -0.253, P=0.025).
Discussions
The pre-and post-intervention tests showed that pupils lacked nutrition knowledge (an average of 30.05% at pretest) and identified the need to increase effort on nutrition education in Gatanga District. Interventions on nutrition education to improve knowledge and practice that support healthy eating to address iron deficiency are required in any given population (Kakunted, 2008). After the intervention the average mean mark in nutrition knowledge in experimental schools improved to an average of 46.8% and the control school 31.21%. Post-tests showed a significant difference with the experimental schools performing significantly better than the control school at p<0.001. Pupils’ became more confident in answering nutrition questions after the intervention. There were significant positive correlations between nutrition knowledge and hemoglobin levels as explained in Table 6. The pupils in the experimental school improved their nutrition knowledge, iron rich food intake which could have positively influenced their hemoglobin levels. Deworming may also have influenced the hemoglobin levels in experimental schools as compared to the control school. Hemoglobin levels were lower before the interventions but significantly improved in the experimental schools. The peer facilitated school had the best improvement in haemoglobin levels, followed by the agriculture facilitated and the then researcher facilitated school. Peers may have had more influence to their colleagues who may have developed more confidence in their teaching hence better performance in many aspects of the interventions. After the interventions those children who were anaemic decreased in the experimental but increased in the control schools. This implies that the interventions were effective and pupils’ haemoglobin levels were improving. Relationship between nutrition knowledge and micronutrient rich food intake showed increased nutrient intake and iron status. There was an increased iron rich food intake and hence increased hemoglobin. The findings of the intervention study leads to the conclusion that the food based approach using the three nutrition education teaching strategies (Peer facilitated, Researcher and agricultural extension worker facilitated) could have some influence and hence an effective strategy to combat iron deficieny and promote good health and well-being of the pupils. Emphasis should be laid on the importance of nutrition education among the school pupils to address malnutrition. They should be given comprehensive knowledge for them to understand the importance of a balanced diet and the causes of deficiency diseases especially the importance of micronutrients like iron in the body. Topics should be included in the syllabuses that focus on promoting the use of iron rich foods to both the pupils and the caregivers.
Acknowledgements
My gratitude goes to the Youth Action for Rural development (YARD) Agricultural field staff, District Commissioner, District Education Officer, District Agriculture Officer, Medical Officer of Health, Public Health officer and his field officers, Laboratory technicians, the Pharmacists in Gatanga district for making it possible and enjoyable to carry out the study in the district. Special thanks go to the head teachers, senior teachers, class six teachers in all the study schools for support and validating the teaching materials that were used to teach the school pupils. Not to forget are the study pupils and their parents for their patience; interest and cooperation in making this study a success. The Government of Kenya through the Ministry of Agriculture for their support.
References
- The FRESH Framework. Access to Health and Nutrition Services. Focusing Resources on Effective School Health (FRESH) – Health related school policies, safe water and sanitation, and skills based health education. Retrieved on 23rd July 2013 (Admin) (2013).
- United Nations Childrens Education Fund. (2008). The Kenya National Technical Guidelines for Micronutrient Deficiency Control.Micro-nutrient Initiative. Ministry of Public Health and Sanitation, Kenya Pg 49-64.
- World Health Organisation. (2013). Micronutrient Deficiencies. World Health Organization Website 2013. Retrieved on 25th March 2013.
- Ramzan, M; Ali, I. & Salam, A. Iron Deficiency Anemia in School Children of Dera Ismail Khan, Pakistan. Pakistan Journal of Nutrition 8 (3): 259-263, 2009 .ISSN 1680-5194 (2009).
- Kaya, M; Pehlivan, E; Aydogdu, I; Genc, M; Gunes, G; Kaya, E. & Kuku, I. Iron Deficiency Anaemia Among students of Two primary Schools at different socio-economic conditions In Malatya, Turkey. Public Health specialist, Local office of the Ministry of Health, Mother and Child health center, Malatya, Inonu Universitesi Tip Fakultesi Lojmanlari, 22 Blok, No;7 Malatya-Turkey. Pg 236-242 (2006).
- Kakunted, P. Nutrition Education Material to Address iron deficiency Anaemia in Kenya. A Master’s of science Thesis, Faculty of the Department of Nutrition, Food Science, and Packaging, San Jose State University. UMI Number: 1459707. ProQuest LLC,789E. Eisenhower Parkway, P.O Box 1346 Ann Arbor, MI 48106-1346 (2008).
- Ismail, I. Awareness of Teachers of the Relationship between Students’ Performance and Nutrition Status: Egypt’s Experience. National Institute of Nutrition, Egypt (2004).
- Stoltzfus, R. J; Chwaya, H. M; Tielsch, J. M; Schulze, K. J; Albonico, M. & Savioli. L. (2001). Epidemiology of iron deficiency anemia in Zanzibari school children: the importance of hookworms. Center for Human Nutrition, Department of International Health, Johns Hopkins School of Public Health, Baltimore, MD 21205, USA.
- KNBS. (2010). Kenya demographic and health survey 2008/09. Kenya Bureau of statistics, Nairobi, Kenya. Calverton, Maryland: KNBS and ICF Macro. Pg1-106.
- Ministry of Health and sanitation / United Nations Childrens Education Fund. (1999). Anaemia and the Status of Iron, Vitamin A and Zinc in Kenya. The 1999 National Micronutrient Survey Report Pg 3-15.
- United Nations Childrens Education Fund. (2009). Nutrition situation update and Rationale for Financing Nutrition within the Health sector in Kenya. www.UNICEF.
- Ministry of Public Health and sanitation. (2012). Scaling Up Nutrition Symposium 5th -6th November 2012 Reports.
- Gunde, R. School children in Developing world: Health, Nutrition and school performance. UCLA International institute,11248 Bunche hall,Box 951487, Los Angeles, CA90095-1487, email:info-intl@internationalucla.edu (2004).
- World Health Organisation. (2007). Micronutrient Deficiencies. World Health Organization Website 2007.
- Ministry of Educatio(MOE). (2007). School Feeding Programme Handbook. Ministry of Education and World Food Programme. Kenya institute of Education.
- Andang’o, P.E.A; Osendarp, S.J.M; Ayah, R; West, C. E; Mwaniki, D.L; De Wolf, C.A; Kraaijenhagen, R; Kok, F.J & Verhoef, H.. Efficacy of iron-fortified whole maize flour on iron status of school children in Kenya: a randomized controlled trial, scientific journal. The Lancet of Sub-department of Human Nutrition Wageningen University(2007).
- Sifri, Z; Darnton-Hill, I.; Baker, S.K; Bendech, M; Aguayo,V.M. A concise overview of Micronutrient Deficiencies in Africa and future directions. African journal of food & Nutritional Sciences(AJFNS) online version ISSN 1681 – 608 ( 2002)Volume 2 No. 2 (2002).
- Food and Agriculture Organization. (2005). Classroom Curriculum Chart. Learning Objectives For Nutrition Education in Primary Schools in Developing Countries. Promoting Lifelong Health.Pg 1.
- Food and Agriculture Organization. (2005). Nutrition Education in Primary Schools.” A planning guide for curriculum Development Vol 1 and 11. FAO viale delle terme di caracalla, 00100 Rome Italy. Pg 1-8
- Food and Agriculture Organization. (2005). Setting up and Running a school garden. A manual for teachers, parents and communities. Promoting Lifelong healthy eating habits.FAO viale delle terme di caracalla,00100 Rome Italy. Pg 1-19.
- Alex, B; Njenga, J & Embeywa, H. (2010). Science in Action, Pupils Book 5. Oxford New Syllabus, University Press, East Africa Ltd, Nairobi Kenya. Pg 56-63.
- Vasishta S. K; Patel N. M. (2002). Learning Science for standard 5, Latest Revised Syllabus. Malimu Publications. Printed by: English Press Limited P.O. Box 30127,00100, Nairobi.Pg 59-119.
- Food and Agriculture Organization. (2013). Nutrition Education in Primary Schools in Argentina. UN: Ministry of Education, Science and Technology (MECyT); Secretary of Agriculture, Livestock, Fisheries and Foods, (SAGPyA) of the Ministry of Economy and Production. FAO web site retrieved 25thMarch 2013.
- Mugenda, O. & Mugenda, A. (2003). Research Methods. Quantitative and Qualitative Approaches .Nairobi. Acts press, 5 41-68





Web of Science Coverage
Emerging Sources Citation Index (ESCI)
2024 Journal Impact Factor: 1.1
Scopus Journal Metrics
CiteScore 2025: 2.6
CiteScore Details
Sustainable Nutrition: Food Systems, Nutrient Retention, and Public Health Impact
![]()
This journal is a member of, and subscribes to the principles of, the Committee on Publication Ethics (COPE)








