Introduction
According to UNICEF, there are about 1.2 billion adolescents populations around the world, among them 88% are living in developing nations.1 As adolescents have a low prevalence of infection compared with under five children, and of chronic disease compared with ageing people, they have generally been given little health and nutrition attention, except for reproductive health concerns.2
According to WHO, in many developing countries, research and investment in health has been mainly devoted to infectious diseases, despite the growing need to address chronic diseases with more effort and resources.2 Deaths from infectious diseases, maternal and perinatal conditions and nutritional deficiencies combined are projected to decline by 3% over the next 10 years, while at the same time deaths due to chronic diseases are projected to increase by 17%. As a result, it is estimated that of the projected 64 million deaths worldwide in 2015, 41 million (64%) will result from chronic diseases unless urgent action is taken.3 Obesity is a well-recognized risk factor for various chronic health problems such as cardiovascular diseases, hypertension, stroke, type 2 diabetes mellitus, osteoarthritis and certain cancers. These conditions not only lead to reduced quality of life given their protracted nature, they also lead to premature death.4
Once associated only with high-income countries, overweight and obesity are now also prevalent in low and middle-income countries.5 It is currently estimated that as much as 20-50% of urban populations in Africa are classified as either overweight or obese and that by 2025, three quarters of the obese population worldwide will be in non-industrialized countries.6 WHO had declared overweight as one of the top ten health risks in the world and one of the top five in developed nations.7 Although an increased prevalence of overweight and obesity was initially detected among adults, a significant increasing trend in the prevalence of overweight and obesity among adolescents has been documented over the last few decades worldwide becoming an emerging public health issue for adolescents in developing countries.8 For example, estimates for the global prevalence of overweight and obesity among children and adolescents were made in 2004 and it was concluded that 10% of school-age children (age range: 5-17) were overweight, of which about a quarter (2-3% of school-age children) were obese. In actual numbers, the estimate suggested some 150-160 million school-age children worldwide were overweight, of which some 35-40 million were obese.9
There are only a small number of surveys examining the prevalence of overweight and obesity among adolescents in developing countries. With poverty and under development exacerbating the threat of infectious diseases, including HIV-AIDS, most public health nutrition programs have focused on under-nutrition and food security. From the information available, the prevalence of adolescent obesity appears to be rising in developing countries.8
Available evidences showed that one of the effective ways to prevent obesity in the adult life is prevention and management of adolescent overweight and obesity. A fundamental step in the prevention and control of obesity is the identification of risk factors contributing to the rapid increase of obesity. Therefore, the present study aims to provide baseline and reference data on the prevalence and the associated factors of overweight and obesity among urban communities of school adolescent in Hawassa city, which is one of the economically, industrially and culturally fast growing cities in the Ethiopia.
Methods
Study Setting and Sample
Institution based cross sectional study was conducted among high school adolescents in Hawassa city. Hawassa, a capital city of SNNPR and Sidama Zone, is 273 km South of Addis Ababa. The city administration has a total area of 157.2 sq. kms divided in to eight sub cities and 32 kebeles. In the city administration, there are 164 schools, of which 39 are governmental while the rest 125 are nongovernmental schools. Data was collected from February to March 2012. The sample size was determined using the formula of sample size determination for single population proportion taking the proportion of adolescents overweight to be 25 % from the study in Addis Abeba.10 Based on statistical formula, the total sample size calculated for this study was 599. Design effect and default was considered in the sample size calculation. A stratified sampling technique was used to select samples. All high schools in Hawassa city were classified in to three categories based on their ownership into governmental, private and missionary. Since students from private and missionary schools share similar feature based on their family ability to pay school fee, for the present study the two categories were merged to provide two stratas. Twenty high schools from the two strata’s (15 nongovernmental and 5 governmental) were found having 16,724 students (male-8917 and female-7807) in age range of 10 – 19 years. From the total high school in the city administration, Tula high school was excluded from the study because the inhabitants have life style likes that of the rural peoples and they reside out of Hawassa city. Eight high schools (2 governmental and 6 nongovernmental) were selected by using PPS. From the 154 sections in the selected schools, 64 were selected based on PPS. After having the number of students to be selected in each section through PPS, a systematic sampling technique was employed to identify the students from the selected sections through the following procedure. A sampling interval was calculated by dividing the total students in each class by the sample size to be drawn from that class. As a starting point, a random number was generated between one and the sampling interval. The generated number indicated the first student to be included in the sampling process. Then the sampling interval was added on to the first number to identify the consecutive students from the list.
Data Collection
Trained diploma nurses were employed to collect data using pre-tested structured questionnaires which were administered to the selected adolescents from each of the selected class and the subjects were requested to record their responses in the presence of data collector’s and investigator, who provided necessary clarification to the queries, if any, in live classroom sessions. Information on the household possession of articles (car, motor bicycle, pedal bicycle, TV, computer etc) were also collected as a proxy variables for calculation of socioeconomic index. Most parts of the questionnaires were adapted from WHO steps instrument for chronic disease risk surveillance.11
Self-administered qualitative Food Frequency Questionnaire was used to collect information on the frequency of consumption of various foods for the past one-month from all the study subjects. This method was designed to obtain qualitative descriptive data on usual intake of food and class of food over a long period. Food frequency questionnaires are useful for ranking of individuals for specific food items so that characteristics of those with high and low intakes can be compared.12
Anthropometric measurements like weight, height, and TSFT were performed by using calibrated equipment and standardized techniques. The researcher performed all anthropometric measurements to eliminate inter-examiner error. Weight was recorded using SECA electronic weight scale and height was measured by using the Stadiometer. TSFT was measured using slim-guide skin fold calipers.12 Two reading of height, weight and TSFT were taken and their mean were considered as final. TSFT & BMI that is the ratio of weight in kilogram to height in meter square were used to assess overweight and obesity in the study subjects. The new WHO reference data using WHO Anthro-Plus computer program was utilized for the estimation of overweight and obesity in the study subjects. The values between 85th to 97th percentile for specific age and sex were considered overweight and values above 97th percentile for age and sex were considered as obesity.13 For TSFT thickness, the values between 85th to 95th percentile for specific age and sex were considered overweight and values above 95th percentile for age and sex were considered as obesity.14
The Global Physical Activity Questionnaire developed by WHO for physical activity surveillance was used to collect information on physical activity participation in three settings (or domains) including activity at work, travel to and from places and recreational activities and sedentary behavior. The activity level of the study participants were evaluated according to the standard WHO total physical activity calculation guide.11
Statistical Analysis
Data were analyzed using SPSS version 16 and WHO Anthro-Plus programs. Descriptive statistics using frequencies, proportions and table were used to present the study results. Chi-square test was used for unadjusted analysis nominal factors associated with adolescent overweight and obesity. Multivariable analysis were performed following bivariate analysis to adjust for the effect of confounders using multiple logistic regression, both crude and adjusted odds ratio with 95% confidence interval were reported. All continuous data were checked for normality using the Kolmogorov-Smirnov test and statistical significance was considered at significance level of 5%. Agreement between BMI and TSFT was determined by Kappa (k) coefficient, which provides the chance-adjusted agreement in identifying the same individuals as overweight or obese. The Shrout, classification was used to interpret the k values as follows: 0–0.1, virtually none; 0.11–0.4, slight; 0.41–0.6, fair; 0.61–0.8, moderate; and 0.81–1, substantial.15
Prior to starting the work, the Ethical Review Committee of the Hawassa University approved the study proposal. The nature of the study was fully explained to the the school administration, participants and parents of the participants and prior written consent for the study was taken from them. Data obtained from each study participant was kept confidential and all who participated in the study were acknowledged.
Result
A total of 554 participants from the two groups of schools, government 366 (61.1%) and non-government 188 (33.9%) were involved in this with a response rate of 93%. Sex were evenly divided among the study participants, 280 (50.5%) were males and 274 (49.5%) were females. The median BMI of the study participants were 19.852 kg/m2 ranging from 14.27-37.66 kg/m2 while the median value of TSFT were 11.5 mm ranging from 3.5-41 mm. Majority of the study participants, 405 (73.10%), were under the age range of 16-18 years. 262 (47.3%) of the study participants were Protestants, whereas 233 (42.1%) were Orthodox by their religion. Around one third of the study subjects 188 (33.9%) were Sidama by their ethnicity, followed by Amhara 94 (17.0%), and Oromo 70 (12.6%) (Table 1).
Regarding marital status, 552 (94.2%) of the study participants, were single and more than one third 216 (39.0%) of the study participants were from ninth grade level, while grade ten, eleven and twelve accounted 157 (28.3%), 96 (17.3%) and 85 (15.3%), respectively. The majority 329 (59.4%) of the study participants were living in the family size between five and seven followed by more than eight 141 (25.5%). Parental educational status revealed that more than half 302 (54.5%) of the fathers had attended more than secondary school education whereas 45 (8.1%) of the fathers had no formal education. On the other hand around one third 192 (34.7%) of the mothers had attended more than secondary school education, attending secondary school education, primary school education and no formal education each accounted 143 (25.8%), 137 (24.7%) and 82 (14.8%) respectively. Almost half 278 (50.2%) of the participants were from medium socio economic index category. The major occupation of the fathers and the mothers were government employee 224 (41.6%) and housewife 207 (38.3%) respectively.
Concerning the family ownership of vehicle, 208 (37.5%) of the participants family had pedal bicycle while 154 (27.8%) and 74 (13.4%) had motor bicycle and car respectively. The majority of the households 473 (85.4%) had television, while around half 279 (50.4%) had house phone, nearly one third 168 (30.3%) had computer and majority of the participants 407 (73.5%) had personal cell phone.
The physical activity pattern of participants was assessed using the GPAQ which were evaluated according to the standard WHO total physical activity calculation guide (Annex 11). Evenly divided proportion of adolescents were engaged in high 252 (45.5%) and moderate 231 (41.7%) activity while few 71 (12.8%) proportion of adolescents had low (sedentary) activity pattern. 403 (72.7%) of the participants used to watch TV or used computer for less than three hours daily and nearly one third of adolescents 151 (27.3%) watched TV or used computer for more than three hours daily. Very large proportion 431 (77.8%) of adolescents never consumed alcohol, while 366 (66.1%) eat three meal per day, 238 (43.0%) eat one or less snack per day, 279 (50.4 %) never skipped their breakfast and 267 (48.2%) eat two to four meal per week out of their home (Table 2).
Based on FFQ, nearly every participant 525 (94.7%) eat cereals based foods either more than once per day or once per day. Minority of participants used vegetables 159 (28.7%) and fruit 153 (27.6%) only three to six times per week. Majority 377 (68.1%) of the participants consumed fish twice per month or less while similar proportion 381 (68.8%) of the participants consumed sweet either more than once per day or once per day. Only few participants consumed meat 99 (17.8%), egg 86 (15.5%) and fast food 112 (20.2%) either more than once per day or once per day.
It was found out that the prevalence of overweight in the study participants was 12.9 % and the prevalence of obesity was 2.7% based on BMI for age classification while based on TSFT, the prevalence of overweight and obesity was 11.0% and 3.8% respectively. The combined prevalence of obesity and overweight was 15.6 % and 14.8 % based on BMI for age classification and TSFT classification respectively. Statistically significant agreement was observed between the two tools (k=0.841; p <0.001).
The prevalence of overweight and obesity for age group 10-14 was 12.5% and 0% respectively, whereas for age group 15-19 was 12.9% and 2.8% respectively. The sex specific prevalence of overweight was 5.7% for males and 20.2% for females, whereas obesity was 1.1% for males and 4.4 % for females. Additionally the prevalence of overweight and obesity in non-governmental school was 20.4 % and 6.5 % where as in governmental school its prevalence was around 9% and 0.8% respectively.
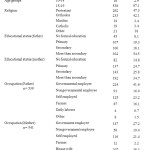 |
Table 1.Demographic and Socio-economic characteristics of adolescents in Hawassa, 2012. Click here to View table |
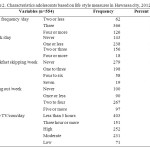 |
Table 2. Characteristics adolescents based on life style measures in Hawassa city, 2012 Click here to View table |
General chi square test for independence was use to investigate the association between the prevalence of overweight and obesity and nominal explanatory variables. Accordingly school ownership, sex of the participants, head of the house hold, time spent watching television or using computer and mother’s occupation were found to be significantly associate with being overweight (p<0.05). Chi square test for trend was used to measure of association between prevalence of overweight and obesity and ordinal measure explanatory variables and consumption of fruit, vegetables, meat, egg, sweet, fast food, TPA and socio economic index were found to be statistically associated with the dependent variable (p<0.05).
Multivariable analysis was done using the significant variables in the bivariate analysis. Forward stepwise likelihood ratio method of the multiple logistic regressions was used to select variables with significance level of 0.05. The most important covariates identified were: sex, consumption of fruit, meat, fast food, socio economic index, TPA and time spent using TV/computer were significantly associated with the dependent variable (Table 3).
The present study found that adolescent girls were 5.14 times more likely at risk of becoming overweight and obese than adolescent males (AOR=5.14 [95%CI: 2.41-10.99]). Adolescent students who eat fruit twice per month or less are 4.67 times more likely to be overweight than adolescents who eat fruit for more than two times per day (AOR= 4.67 [95%CI: 1.76-12.38]). The odds of being overweight were 91% lower in adolescents who eat meat twice per month or less compared with adolescents who eat meat once or more than once per day (AOR=0.09 [95%CI: 0.03-0.25]). Adolescents from higher socio economic index category were 7.19 time at higher risk for becoming overweight as compared to adolescents whose family socio economic index were in the lowest category (AOR=7.19 [95%CI: 2.6-19.89]).
Total physical activity was associated statistically with overweight and obesity in the study population. Adolescents in low (sedentary) activity category were 5.46 times more likely to be obese than that of active adolescents (AOR= 5.46 [95%CI: 2.25-13.21]). There was statistically significant association between times spent watching TV or using computer and overweight. Those adolescents who used to watched TV or used computer three or more hours per day were 3.04 times more likely to be overweight than those who watched TV or used computer for less than three hours per day (AOR =3.04 [95%CI: 1.52-6.11]).
Finally, the odds of being overweight were 88% lower in adolescents who eat fast food twice per month or less in the previous one month period compared with adolescents who eat fast food more than once per (AOR=0.12[95%CI: 0.04-0.34).
 |
Table 3. Odds ratios of overweight and obesity for demographic, socioeconomic, dietary and physical activity factors (logistic regression analysis) for adolescents in Hawassa city, 2012 Click here to View table |
Discussion
The study showed that the prevalence of overweight in the study participants was 12.9 % and the prevalence of obesity was 2.7% based on BMI for age classification while based on TSFT, the prevalence of overweight and obesity was 11.0% and 3.8% respectively. The combined prevalence of obesity and overweight was 15.6 % and 14.8 based on BMI for age classification and TSFT classification respectively. Statistically significant agreement was observed between the two tools (k= 0.841; p <0.001). The present study used BMI classification for further analysis of the problem of overweight and obesity, as this method has been increasingly accepted the most popular and accepted indirect measure of adiposity in adolescents for survey purposes. The present study demonstrated that quite numbers of adolescents were overweight and obese indicating that to some extent there was high prevalence of overweight and obesity in adolescents living in an urban community of Hawassa.
However, the prevalence of overweight and obesity in this finding was lower than that of developed countries such as USA,16 Canada ,17 Greece18 and Italy19 having the prevalence of overweight ranging from 22-36% and obesity 4.15- 9.45 respectively. The present finding was better comparable with the study from developing countries. The results indicated a significant sex difference of overweight (males 5.7% vs females 20.2%) and obesity (males 1.1% and females 4.4 %) with girls 5.14 times more likely to be overweight or obese compared with boys (AOR=5.14 [95%CI: 2.41-10.99]). Similar reports were observed from different studies. The First South African National Youth Risk Behavior Study of schoolchildren aged 13–19 years showed that 17% of the participants were overweight and 4% obese nationally, of which 7% of boys and 25% of girls were overweight.20
In Tunisia, the prevalence of overweight was 18.9% (male 17.2% vs. female 20.7%) and obesity 4.3%, i.e male 4.0% vs. female 4.6%.21 More than twelve percent of Egyptian adolescents (boys 7 % and girls 18 %) were overweight, and 6.2 % (boy 6 % and girls 8 %) were obese.22 Prevalence of overweight and obesity among primary school children age 5-19 in Addis Ababa was 7.6 % (boys 5.4% vs girls 9.4) and 0.9 % ( boys 1.1 % and girls 0.8 %) respectively.23 Contradicting result regarding sex specific distribution of overweight and obesity were observed from different countries including, Canada,17 Greece18 and Italy19 where the prevalence were more among boys than girls but in most developing countries prevalence is more in girls which is true for the present study also.
Many studies in LMICs revealed the higher prevalence of obesity among adolescent girls compared to boys; several factors may explain these sex differences. Biologically, energy needs differ for boys and girls and in relation to rate of growth. Further, timing of sexual maturation differs by sex.24 Behavioral factors are also important in explaining the sex differences: boys are generally more physically active compared to girls especially during adolescence.25 Concerns about body image, particularly among adolescent girls, may lead to problematic eating behaviors such as irregular meal patterns that may result in increased weight gain.26 Additionally, girls in developing countries like Ethiopia may stay at home for long time and their movement from place to place are much restricted due to cultural influence than boys which result in physical inactivity leading to overweight and obesity.23
A clear socio-economic gradient in the prevalence of overweight and obesity was observed in this study, where adolescents from higher socio economic index category were 7.19 time more likely to be overweight or obese as compared to adolescent whose family was from the lowest socio economic index category (AOR=7.19 [95%CI: 2.6-19.89]). This finding was consistent with the result from different developing countries including India where the prevalence of overweight and obesity was significantly higher (p <0.05) among the adolescents of high SES (15%) compared with those of low SES (3.3%).27 Similar results were reported from Vietnam28 and Mexico29 where increased risk of being overweight or obesity were found in the adolescents from wealthier family. This might be related to the diets, adolescents from higher socio-economic group are well known to adopt western life leading to greater consumption of high fat and high caloric diet which may substitute the healthy traditional diet; cereals, fruit, vegetables, etc , and more sedentary life style. Besides these, patterns of high energy expenditure among the poor and cultural values favoring a larger body size may also continue to contribute to the positive associations observed in lower-income countries,30 which is particularly true in Ethiopian context where childhood and adolescent obesity is still considered a sign of healthiness and high social class.
Many studies from developed countries brought contradicting reports, where food insecurity and poverty are clear risk factor for obesity. In these countries, adolescents in higher socioeconomic groups tend to have a healthier diet, characterized by greater consumption of fruit, vegetables, lower-fat milk and less consumption of fats.31 In Germany levels of obesity was higher in the lower socio-economic groups.32 Additionally report from America supported this finding.33 Possibly the misconception of the population of the developing countries about obesity, its risk and generally the poor knowledge regarding healthy diet contribute to this discrepancy.
In the present study TPA was statistically associated with overweight and obesity. Adolescents in low (sedentary) activity category were more likely to be overweight than that of active adolescents. Report from Pakistan indicated that lack of physical activity was found to be significantly associated with obesity in children and adolescents.34 Another result from India revealed that regular physical activity was an important factor in reducing the prevalence of overweight and obesity, in this study prevalence was significantly lower in adolescents who participated regularly in household chores (P < 0.001), played outdoor games and performed physical exercise.35 Studies from36 Canada 37 and Norway38 also supported the findings of the present study. Decreased energy expenditure in this group may explain the finding.
There is a positive significant association between times spent watching television or using computer and overweight. A similar finding was reported from Iran for school children aged 11–18 years.39 In Iraq, it was found that children and adolescents who watched TV more than 3 hours, were more prone to be obese than those who watched less than 3 hours/day.40 Additionally different studies from Canada 37 and Ireland,41 reported similar result. This could be related to the lack of physical activity in this group.
According to American Dietetic Association, fruits and vegetables have been promoted for the prevention of childhood and adolescent obesity because of their low energy density, high fiber content, and satiety value.42 The present finding indicated that fruit consumption was inversely associated with the adolescent overweight and obesity, adolescent students who eat fruit twice per month or less were 4.67 times more likely to be overweight than adolescents who eat fruit for more than two times per day (AOR= 4.67 [95%CI: 1.76-12.38]).
In bivariate analysis, consumption of vegetable also showed a significant association with overweight but after controlling for potential confounders in the multiple logistic regression models its association disappeared. Different scholars found diverse results concerning the effect of fruit and vegetable on body weight of adolescents. A study from Iran reported that a higher intake of fruits and vegetables in school students (6–18 years) had a significant negative association with increase in BMI.43 A study among university students in Kuwait revealed regular consumption of fruits and vegetables was protective factor for obesity.44 The present investigation on the effect of vegetable consumption was in line with the finding of different studies45,46,47 where they didn’t find the protective effect of vegetable consumption. Most of the observed evidence was stronger for fruits alone or for fruits and vegetables combined than for vegetables alone. The present study did not examined the combined association of fruit and vegetable on overweight and obesity. The lack of association in present study may be related to independent assessment of the effects of vegetable on the prevalence of overweight and obesity.
The odds of being overweight and obese were 91% lower in adolescents who eat meat twice per month or less compared with adolescents who eat meat once or more than once per day. Supporting finding from Switzerland48 and Addis Abeba23 showed a direct association between intake of meat products and overweight and obesity.
The rise in consumption of fast food, in developed and developing nations, might have particular relevance to the adolescent’s obesity epidemics. These foods typically contain potentially adverse dietary factors including saturated and trans fat, high glycemic index, high energy density, and, increasingly large portion size. Additionally, these foods tend to be low in fiber, micronutrients, and antioxidants.49 Similar with most studies the present finding showed significant positive association between fast food intake and the prevalence of overweight and obesity. A longitudinal study in a representative sample of US adolescents found that fast food consumption was associated with increased weight gain from adolescence to adulthood.50 Additionally report from Malaysia pointed out that high consumption of fast foods was the major cause for body weight problem.51
There is no specific definition of snacking, but many studies had considered snacking as eating between meals, especially eating between breakfast and lunch (morning snacking) and between lunch and supper (evening snacking).52 Some studies in the Western World indicated that as snacking increases, the total energy intake increases. However, there is little evidence that a higher frequency of eating per day is a potential cause of obesity. WHO reported that there is insufficient evidence that increased eating frequency leads to increased or decreased obesity,53 similarly no association between snacking, meal frequency and overweight was found in the present study.
The consumption of sweet as a key contributor to the epidemic of overweight and obesity in children and adolescents had been strongly debated. However, contradicting findings were reported concerning the effect of sweet consumption on the prevalence overweight and obesity. In the current study even if sweet consumption was significantly associated with overweight in bivarite analysis, it failed to demonstrate these significance in the multiple logistic regression model. Similar report from Germany found no consistent associations between weight status and sweet consumption.32 In addition large study which examined the associations between overweight and selected dietary and physical activity patterns in school aged youth age 10-16 years from 34 countries. As indicated in their report, a significant (P < 0.05) negative relationship between the intake of sweets and BMI classification were observe in 31 out of the 34 countries (91%), indicating higher sweets intake was associated with a lower odds of being overweight.54 However these big inconsistencies may possibly be related with, first overweight children may deliberately restrict their intake of sweets in order to control weight. Second overweight adolescents are more likely than normal weight adolescents to under-report unhealthy food intake.55 Finally, because in the present study the data was only collected on the frequency of food consumption, it is possible that the overweight youth ate greater portion sizes and thus consumed greater amounts of sweets even though they consumed sweets less often.
Obese adolescents are more likely to skip breakfast or to eat smaller breakfasts than leaner adolescents. The evidence seems to suggest that breakfast skipping may be a risk factor for increased adiposity, particularly among older children or adolescents. However, the strength of the evidence is limited. The present study found out no association regarding the effect of breakfast skipping and prevalence of overweight and obesity. Several studies supported this finding.56, 57 In contrast a positive association between breakfast skipping and a measure of adiposity indicating that breakfast skippers were more likely to have a weight higher than normal were reported.58,59,60 Present finding may be explained by the smallest value given to breakfast in Ethiopia, where most segment of the community eat smaller breakfasts as it is traditionally accepted as “yegororo mamuasha”, so that there might be minimal difference in between groups who consume breakfast or not.
Regarding the eating out behavior of adolescents, no significant association was found in the present study. Similarly, a nationally representative study found no association between food eaten away from home and reported BMI.56 However, other investigators have found a significant positive association between the frequencies of eating out behavior and increased in body weight.36 The consumption of regular household diets out of the home environment may possibly explain the present finding.
Conclusion
The present study revealed that more than one tenth of adolescents were overweight, making it a hidden problem of Hawassa city. More disturbing is the fact that compared with earlier studies in other parts of the country, there is an increasing trend for overweight and obesity among adolescents. The causes of overweight and obesity among adolescents aged 10-19 years in the study area may be many and complex but might stem basically from the life style of adolescents. Higher socioeconomic status, low levels of physical activity, watching television for more than three hours per day and frequent consumption of meat, fast foods, limited fruit consumption and being female were significantly associated with a higher prevalence of overweight and obesity in the study subjects. Based on the observed finding the authors recommend the following points in order to control the problem of overweight and obesity among adolescents in the study area. As a recommendation, adolescents and their families should receive health education on diet and physical activity. Additionally school based preventive program should be set and adolescent girls and private schools should be the first target for intervention.
Competing Interest
The authors declared no competing interests
Acknowledgments
The authors want to thank NORAD project coordinating office for funding the research study. Our gratitude also goes to those involved directly or indirectly in the accomplishment of this research.
References
- UNICEF: State of the World’s Children: Adolescence–An Age of Opportunity; 2011.
- WHO (World Health Organization): Preventing chronic diseases; A vital investment, Geneva; 2005.
- Victora CG., Adair L, Fall C, Hallal PC, Martorell R, Richter L, Sachdev HS: Maternal and child under nutrition: Consequences for adult health and human capital. Lancet 2008, 371 (9609): 340-357.
CrossRef - Asfaw A: The effects of obesity on doctor-diagnosed chronic diseases in Africa: empirical results from Senegal and South Africa. J. Public Health Policy 2006, 27 (3): 250-264.
CrossRef - Campbell T: Emerging disease burdens and the poor in cities of the developing world. J. Urban Health 2007, 84 (3): 54-64.
CrossRef - Kamadjeu RM, Edwards R, Atanga JS, Kiawi EC, Unwin N, Mbanya JC: Anthropometry measures and prevalence of obesity in the urban adult population of Cameroon: an update from the Cameroon Burden of Diabetes Baseline Survey. BMC Public Health 2006,6: 228.
CrossRef - WHO (World Health Organization): The World Health Report; Reducing Risks, Promoting Healthy Life, Geneva: 2002.
- Popkin BM: Global nutrition dynamics: the world is shifting rapidly toward a diet linked with non-communicable diseases. Am. J. Clin. Nutr 2006, 84:289-98.
- Wang Y, Lobstein T: Worldwide trend in childhood overweight and obesity. Int.J. pediatr.Obes 2006, 1(1): 11-25.
CrossRef - D. Kebede, T. Ketsela: Precursors of atherosclerotic and hypertensive diseases among adolescents in Addis Ababa, Ethiopia Bulletin of the World Health Organization 1993, 71 (6): 787-794.
- WHO (World health organisation): The WHO Stepwise approach to chronic disease risk factor surveillance (STEPS), Switzerland; 2007.
- Gibson R.S. 2005. Principles of nutritional assessment 2nd edition. Oxford university press; 319.
- WHO (World Health Organization): WHO AnthroPlus for personal computers. Manual: Software for assessing growth of the world’s children and adolescents. Geneva; 2009.
- Must A, Gerard ED, William HD: Referencing data for obesity: 85th and 95th percentiles of body mass index and triceps skin fold thickness. Am. J. Clin. Nutr 1991,53: 839-46.
CrossRef - Shrout PE: Measurement reliability and agreement in psychiatry. Statistical Methods in Medical Research 1998, 7: 301–317.
CrossRef - Flegal KM, Ogden CL, Wei R, Kuczmarski RL, Johnson CL: Prevalence of overweight in US children. Comparison of US growth charts from the Centers for Disease Control and Prevention with other reference values for body mass index. Am. J. Clin. Nutr 2001.73: 1086–1093.
- Tremblay MS, Katzmarzyk PT, Williams J.D: Temporal trends in overweight and obesity in Canada, 1981–96. Int. J. Obes 2002, 538–543.
CrossRef - Krassas GE, Tzotzas T, Tsametis C, Konstantinidis T: Prevalence and trends in overweight and obesity among children and adolescents in Thessaloniki, Greece. J. Pediatr. Endocrinol.Metabol 2001, 14: 1319–1326.
- Vignolo M, Pistorio A, Torrisi C, Parodi A, Grassi S, Aicardi G: Overweight and obesity in a group of Italian children and adolescents: prevalence estimates using different reference standards. Ital. J. Pediatr 2004, 30: 53-57.
- Medical Research Council. Umthente Uhlaba Usamila: The1st South African National Youth Risk Behaviour Survey. Pretoria:Department of Health, 2002. (http ://www.mrc.ac.za/healthpromotion/healthpromotion.htm ) (accessed on March, 2012).
- Aounallah-Skhiri H, Traissac P, Ati JEI, Eymard-Duvernay S, Landais E, Achour N, Delpeuch F, Romdhane HB Maire B. Nutrition transition among adolescents of a South-Mediterranean country: dietary patterns, association with socio-economic factors, overweight and blood pressure. A cross-sectional study in Tunisia. Nutrition Journal 2011, 10: 38.
CrossRef - Kelishadi R: Childhood Overweight, Obesity, and the Metabolic Syndrome in Developing Countries. Epidemiologic Reviews 2007, 29 (1): 62-76.
CrossRef - Zeleke A: Prevalence of childhood and adolescent overweight and obesity among elementary school students in Addis Ababa: Double burden of malnutrition in Ethiopia. Msc. Thesis, Addis Abeba University. Addis Abeba, 2007.
- Wisniewski AB, Chernausek SD: Gender in childhood obesity: family environment, hormones and genes. Gend. Med 2009, 6 (Suppl 1): 76-85.
CrossRef - Kruger R., Kruger H.S, Macintyre UE: The determinants of overweight and obesity among 10- to 15-year-old schoolchildren in the North West Province, South Africa – the THUSA BANA (Transition and Health during Ur20banisation of South Africans; BANA, children) study. Public Health Nutr 2006, 9 (3): 351-358.
CrossRef - Neumark-Sztainer D, Paxton SJ, Hannan PJ, Haines J, Story M: Does body satisfaction matter? Five-year longitudinal associations between body satisfaction and health behaviors in adolescent females and males. J. Adolesc. Health 2006, 39 (2): 244-251.
CrossRef - Laxmaiah A, Nagalla B, Vijayaraghavan K, Nair M: Factors Affecting Prevalence of overweight among 12-17-year-old urban adolescents in Hyderabad, India. Obesity 2007, 15: 6
CrossRef - Tang HK, Dibley MJ, Sibbritt D, Tran HMT: Gender and socio-economic differences in BMI of secondary high school students in Ho Chi Minh City. Asia Pac. J. Clin.Nutr 2007, 16 (1): 74-83.
- Salazar-Martinez E, Allen B, Fernandez-Ortega C, Torres-Mejia G, Galal O, Lazcano-Ponce E: Overweight and obesity status among adolescents from Mexico and Egypt. Archives of Medical Research 2006, 37 (4): 535-542.
CrossRef - Monteiro CA, Moura EC, Conde WL: Socioeconomic status and obesity in adult populations of developing countries. A review. Bull World Health Organ 2004, 82: 940–6.
- Power EM: Determinants of healthy eating among low-income Canadians. Can. J. Public Health 2005, 96 (suppl. 3): 37–8.
- Kleiser C, Rosario SA, Mensink GBM, Langenohl RP, Kurth BM: Potential determinants of obesity among children and adolescents in Germany: results from the cross-sectional KiGGS study. BMC Public Health 2009,9: 46.
CrossRef - Boumjte PI, Huang C.L, Lee, Lin JY, Hwan B: Dietary habits, demographics and the development of overweight and obesity among children in the United States. Food Policy 2005, 30 (2): 115-128.
CrossRef - Warraich HJ, Javed F, Faraz-ul-Haq M, Khawaja FB, Saleem S: Prevalence of Obesity in School-Going Children of Karachi. Obesity in Pakistani.Children 2009. 4 (3):4816.
- Kumari DJ, Krishna BSH: Prevalence and risk factors for adolescents (13–17 years) overweight and obesity. Current science 2011, 100: 3.
- Chacar HR, Salameh P: Public schools adolescents’ obesity and growth curves in Lebanon. Lebanese Medical Journal 2011, 59 (2):81.
- Janssen I, Katzmarzyk PT, Boyce WF, King MA, Pickett W: Overweight and obesity in Canadian adolescents and their associations with dietary habits and physical activity patterns. Journal of Adolescent Health 2004, 35 (5): 360-367.
CrossRef - Fasting MH., Nilsen TIL, Holmen TL, Vik T: Life style related to blood pressure and body weight in adolescence: Cross sectional data from the Young-HUNT study, Norway. BMC Public Health 2008, 8: 11.
CrossRef - Veghari G, Sedaghat M, Joshaghani H: The prevalence of obesity and its related risk factor in the north of Iran. Journal of Research in Health Sciences 2010, 10(2): 116–121.
- Lafta RK, Kadhim MJ: Childhood obesity in Iraq: prevalence and possible risk factors. Annals of Saudi Medicine, 2005. 25(5):389–393.
- Ochoa MC, Moreno-Aliaga MJ, Martínez-González MA, Martínez JA, Marti A, the GENOI Members: Predictor factors for childhood obesity in a Spanish case-control study. Nutrition 2007, 23 (5): 379-384.
CrossRef - American Dietetic Association: Individual, family, school and community-based interventions for pediatric overweight. J. Am. Diet Assoc 2006, 106:925–945.
CrossRef - Kelishadi R, Ardalan G, Gheiratmand R: Thinness,overweight and obesity in a national sample of Iranianchildren and adolescents: CASPIAN Study. Child: Care, Health and Development 2008, 34 (1): 44–54.
- El-Ghazali S, Ibrahim JM., Kanari BM, Ismail NA: The relationship between lifestyle and body mass index among university students in Kuwait. Egyptian Journal of Community Medicine 2010, 28: 69–76.
- Lin BH, Morrison RM. Higher fruit consumption linked with lower body mass index. Food Rev 2002, 25: 28–32.
- Boutelle K, Sztainer DN, Story M, Resnick M: Weight control behaviors among obese, overweight and nonover weight adolescents. J. Pediatr Psychol 2002, 27: 531–540
CrossRef - Rockett HR, Berkey CS, Field AE, Colditz GA: Cross-sectional measurement of nutrient intake among adolescents. Prev. Med 2001, 33: 27–37.
CrossRef - Aeberli I, Kaspar M, Zimmermann M.B: Dietary intake and physical activity of normal weight and overweight 6 to 14 year old Swiss children. Swiss Med.Wkly 2007,137:424–430.
- Hu FB, Vandam RM, Liu S. Diet and risk of type II diabetes: the role of types of fat and carbohydrate. Diabetologia 2001,44: 805–17.
CrossRef - Niemeier HM, Raynor HA, Lloyd-Richardson EE, Rogers ML, Wing RR: Fast food consumption and breakfast skipping: predictors of weight gain from adolescence to adulthood in a nationally representative sample. J. Adolesc. Health 2006, 39: 842-9.
CrossRef - Sakinah Ha, Seong-Ting Ca, Rosniza Rb, Jayah KPb: Socio-Demographic, Dietary and Physical Activity Determinants of Adolescents Overweight and Obesity in Kelantan. Health and the Environment Journal 2012, 3 (1): 44-53.
- Zaal B, Musaiger AO, D’Souza R: Dietary habits associated with obesity among adolescents in Dubai, United Arab Emirates. Nutricion Hospitalaria 2009, 24 (4): 437–444.
- WHO (World Health Organization): Diet, nutrition and prevention of chronic diseases. WHO Technical Report Series 916, Geneva; 2003.
- Janssen I, Katzmarzyk P, Boyce WF, Vereecken C, Mulvihill C, Roberts C, Currie C, Pickett W: Comparison of overweight and obesity prevalence in school-aged youth from 34 countries and their relationships with physical activity and dietary patterns, Obesity reviews 2005,6: 123–132.
CrossRef - Garaulet M, Martinez A, Victoria F, Perez-Llamas F, Ortega RM, Zamora S: Difference in dietary intake and activity level between normal-weight and overweight or obese adolescents. J Pediatr Gastroenterol Nutr 2000, 30: 253–258.
CrossRef - Lin BH, Huang CL, French SA: Factors associated with women’s and children’s body mass indices by income status. Int. J.Obes. Relat.Metab.Disord 2004, 28: 536–542.
CrossRef - Nicklas TA, Morales M, Linares A: Children’s meal patterns have changed over a 21-year period: the Bogalusa Heart Study. J Am Diet Assoc 2004, 104: 753–761.
CrossRef - Strien TV, Niekerk VR, Ouwens MA: Perceived parental food controlling practices are related to obesogenic or leptogenic child life style behaviors. Appetite 2009, 53 (1): 151-154.
CrossRef - O’Dea JA, Caputi P: Association between socioeconomic status, weight, age and gender and the body image and weight control practices of 6- to 19-year-old children and adolescents. Health Educ Res 2001, 16: 521–532.
CrossRef - Rampersaud GC, Pereira MA, Girard BL, Adams J, Metzl JD: Breakfast Habits, Nutritional Status, Body Weight, and Academic Performance in Children and Adolescents. Journal of the American Dietetic Association 2005, 105: 743-760.
CrossRef

This work is licensed under a Creative Commons Attribution 4.0 International License.






