

Introduction
Micronutrients are vitamins and minerals, essential for a variety of biological functions in the body. Though, their daily dietary requirements are in very small amounts, deficiency in any one micronutrient can cause adverse effects on health such as susceptibility to infections and decreased work capacity. Childhood is marked with physical, mental and sexual development. Nourishing food is vital during this period to prevent malnutrition and attain the growth potential. Particular micronutrients such as iron, iodine, are essential for cognitive development of children while zinc, vitamin A, calcium and vitamin D are associated with linear growth and skeletal development.1.
Deficiencies of iron, zinc, iodine, calcium and folate in children below 5 years of age, are common contributors to poor growth, intellectual impairment, and increased risk of morbidity and mortality.2 Zinc deficiency can result in impaired immunity, stunting and poor-cognitive performance in older children (6–16 years). While anaemia in adolescence can cause reduced physical and mental capacity and diminished concentration in work and educational performance, and also poses a major threat to future safe motherhood in girls.3
Micronutrient deficiencies in children and adolescents can be caused by insufficient food intakes, lack of animal foods in diet, low bioavailability of minerals from plant-based diets and increased requirements.4 The adverse effects of micronutrient deficiencies are preventable by a) including variety of micronutrient-rich foods in daily diet and b) enhancing bioavailability of micronutrients through proper food preparation methods. Therefore, food-based interventions aimed towards increasing dietary modification and diversification are promoted as long-term sustainable strategy for prevention and control of micronutrient deficiencies. Greater dietary diversity has been associated with better growth and micronutrient status in children.5 Many studies have reported development of nutrient-rich recipes using local foods and choosing appropriate food preparation methods such as sprouting, malting, and fermentation, for improving bioavailable micronutrient intakes. Incorporating animal-source foods in the diet has shown to increase availability of vitamin A, iron, zinc and vitamins B2, B12.6 Food-to-food fortification of staple food with underutilized plant species (UUPS); e.g., maize with grain amaranth, soybean and moringa; sweet potato with cowpea, sorghum, casava with African yam bean etc. has shown to improve multiple micronutrient intakes; magnesium, phosphorous, zinc, potassium, iron and rise in fibre and protein levels in children.7 The present review evaluates:
- studies reporting the potential of dietary modification and diversification strategies at the community or household level
- the impact of such dietary interventions on mental and physical health during growing age.
Methods
Studies evaluating food-fortification strategies are diverse in design, outcome measures and age-groups. Therefore, a non-systematic review method was applied and web-based literature search was conducted in bibliographical databases for studies reporting:
- development of nutrient-rich foods or snacks
- assessing the impact of food-based intervention on growth, cognition and other health parameters in childhood.
Inclusion criteria were studies describing: i) formulation and evaluation of micronutrient-rich food products, ii) impacts of meals/snacks or lifestyle intervention at household/school/community level through randomized controlled trials (RCTs), iii) primary outcomes like micronutrient intakes, anthropometry, body composition, cognitive function, biomarkers of micronutrients, morbidity.
Exclusion criteria were studies reporting: i) effect of food fortification by micronutrient powders/sprinkles, ii) micronutrient supplements/tablets/syrups/soft-gels, biofortification, iii) in adult population, iv) in diseases.
Literature search: PubMed Central, Google Scholar, Wiley Online Library were searched for identifying studies. The search keywords included; dietary modification, diversification, micronutrient bioavailability, food-based intervention, randomised controlled trials, children, adolescents, micronutrient-rich foods, local food supplements, food fortification, mid-day meals, growth, bone mass, cognition and health. References from key articles, previous reviews, systematic reviews and meta- analyses were also included in the search.
Results
Study selection
Of the total 106 identified articles, 12 studies describing micronutrient-rich food products and 24 food-based intervention trials that met the inclusion/exclusion criteria were included in this review (Figure 1). Data were extracted from full-text articles of the selected studies.
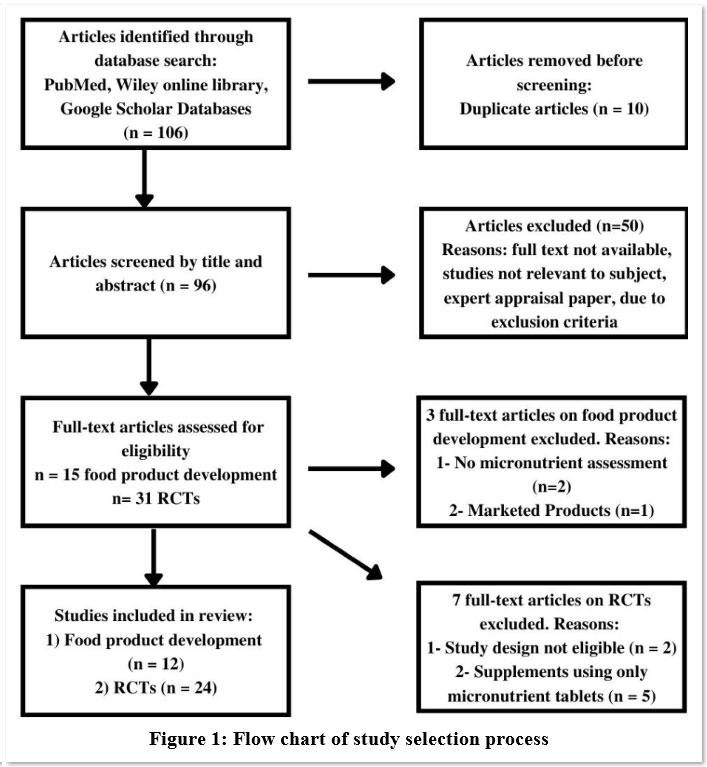 |
Figure 1: Flow chart of study selection process. |
Development of micronutrient-rich food products
Average dietary intakes of micronutrient-rich foods especially vegetables and fruits, are observed to be low in children and adolescents all over the world.8,9,10 To improve micronutrient intakes, twelve studies have reported formulation of new recipes as snacks/meals from leafy vegetables, fruits, pulses and millets (Table 1). Emphasis is given to use locally grown foods which are nutritious and are likely to be acceptable by the children.
Table 1: Characteristics of studies reporting development of nutrient-rich food products.
| Country ref | Participants | Food products | Methods | Findings |
| India 8 | Girls(10-16 yr) n=630 | 20 cereal-pulse-based recipes using chickpea, soybean, seeds, vegetables, with sprouting/fermentation. | 3-day 24-hour diet recall, nutrient intakes, in-vitro zinc dialyzability of new recipes vs common meals. | New recipes have high contents of zinc, calcium, iron, b-carotene, and vitamin C. |
| India 11 | – | Meals; cereal+GLV (29), cereal+pulses (12), cereal+other vegetables (16). | Analysed for 8 micronutrients, macronutrients, bioavailability of iron, zinc, copper | Increased bioavailable densities of iron, zinc, copper, 10-fold rise in b-carotene levels, two-fold rise in folate and riboflavin observed in GLV meals than other meals. |
| India 12 | – | 48 meals comprising of combinations made from 6 cereals, 4 GLV, 4 other vegetables, 4 pulses. | Nutrient contents, in-vitro iron dializability, 31 GLV-based vs 20 non-GLV meals compared. | One GLV-based meal provides > 0.75mg bioavailable iron. i.e. as per 1000 kcal. |
| India 13 | Type-1 diabetic children and adolescents(5-16 yr) (n=70) | 20 healthy snacks rich in calcium, iron, vitamin C, B1, B2, B3, zinc, β-carotene and low carbohydrates developed using spinach, red amaranth, kidney beans, soybean, chickpea, citrus fruits, seeds. | Sensory evaluation, nutrient content of recipes, anthropometry, 3-day diet recall, nutrient intakes. | Five-fold increase in zinc, calcium and iron contents and two-fold increase in vitamin contents (β carotene, vitamin C, vitamin B1, B2, and B3) in new recipes compared with routine snacks. |
| Ghana 14 | School-children (4-12 yr) (n=38) | Local dishes devised using dried M. oleifera leaves; 1) ofam (baked ripe plantain-roasted maize cake), 2) beans and gari (roasted cassava grits), 3) waakye (boiled red cowpea and rice); 4) groundnut soup, 5) porridge (composite white maize, groundnut, and white cowpea meal), 6) nkontomire (cocoyam leaves) sauce, jollof rice and 7) apapransa (boiled cowpea and maize flour). | Acceptability, contents of iron, zinc, copper, manganese, β-carotene. | M. oleifera leaf-fortified local dishes well-accepted by children. |
| India 15 | – | 3 types of khichdi (Rice + pulse thick porridge with vegetable) and paratha (flat bread stuffed with filling) formulated using GLV, pearl millet, maize, chickpea which are rich in iron, B vitamins, carotene. | Sensory evaluation by ten semi-trained members. | Overall acceptability for 2 products. |
| China 16 | 110 mothers with children 6 to 23 months. | Six nutritious recipes using local foods providing vitamin A, B1, B2, calcium, iron and zinc.; 1) rice porridge with tofu and rape, 2) rice with tomato and pork liver,3) noodles with egg, tomato, rape, 4) noodles with pork blood, carrots, 5) rice with lean pork, potato, 6) porridge with pumpkin, rape. | 24-hour dietary recall, acceptability, compliance,f easibility of 10 recommended recipes | Combination of three recipes for daily three meals satisfies most of the daily recommended nutrients for 6-23 months children. |
| India 19 | Girls(7–19 yr) (n=236) | Non-dairy-based calcium-rich products (n=14) compared with dairy-based calcium-rich products (n=12). | 3-day 24-hour dietary recall, sensory evaluation, macro and micronutrient contents of recipes | Non-dairy and dairy products are on par with respect to calcium contents. |
| India 20 | Children(2-16 yr)(n=220) | 25 recipes developed from millets, soybean, horse-gram, kidney beans, amaranth leaves, cauliflower leaves, seeds, dry coconut, using malting/germination, fermentation. | 24-hour dietary recall, calcium, energy and protein contents, calcium intakes, bioavailability | One serving of the recipes provides 42% of the calcium recommended dietary allowance (RDA) in children and 32% in adolescents. Increase of 20% in calcium bioavailability by food processing. |
| Africa 21 | – | Composite flour of sweet potato, avocado, pear, and Turkey berry with different proportions. | Proximate analysis, contents of iron, calcium, phosphorus, potassium, magnesium, sodium, copper, zinc, vitamin C | Composite flour with 40% sweet potato, 35% avocado pear and 25% Turkey berry was optimal in micronutrients. |
| Cambodia 22 | Households, mothers, and children under 5 yr of age (n=500) | Homestead food production, increasing household production and consumption of vitamin A–rich fruits and vegetable and small-animal production activities. | 1) Household intervention (n = 300)2) Control (n = 200), Consumption of micronutrient-rich foods, illness episodes. | Household production and consumption of micronutrient-rich foods increased, improved maternal and child intake. |
| Bangladesh 23 | Children (6-23 months)(n=150) | 35 recipes formulated like pumpkin soup, chicken soup, Chirar pulao (Rice + vegetable composite dish), small fish chops, vegetable khichuri (Rice + pulse + vegetable thick porridge), sweet potato halwa (sweet dish), bread, Rice+Chicken+GLV+oil, Rice+pulse+nuts+sweet potato+oil, Wheat+Fish+vegetable and White sauce etc. | Contents of 10 nutrients in 30 cooked recipes, acceptability of recipes | 28 recipes were most acceptable by both mothers and children. |
GLV: Green Leafy Vegetables, yr – years, RDA: Recommended Dietary Allowance
Habitual diet of adolescent girls was modified by adding sprouted pulses, vegetables to increase bioavailable micronutrient contents of zinc, calcium, iron, b-carotene, and vitamin C.8 These new recipes were found rich in bioavailable micronutrients. Meals comprising of whole cereals and green leafy vegetables (GLV) were found to improve intakes of zinc, riboflavin, copper, and b-carotene11 and also sufficient to satisfy daily iron requirement.12 Snacks without adding sugar/jaggery were made from GLV, beans, fruits and seeds for type-1 diabetic children There was a five-fold increase in calcium, zinc and iron contents as well as two-fold increase in β carotene, vitamin C, vitamin B1, B2, and B3 contents over their usual snacks. 13. Local dishes prepared from GLV, beans, millets and nuts were found to be rich in many micronutrients and acceptable by the young children.14, 15 Meals devised for 6-23 months old Chinese children using rice, tomato, tofu, egg or pork, can meet the recommended dietary allowance (RDA) of most nutrients.16
Low dietary calcium intakes (less than half the RDA) are mainly observed in low- and middle-income countries due to limited intake of dairy products.17,18 To devise recipes/food products rich in calcium contents with high bioavailability, 14 non-dairy food products were developed using millets, soybean, GLV, sesame and methods like malting, fermentation, and sprouting. These were found to be equivalent in calcium contents of 12 dairy-based products prepared using milk, cheese, paneer, cereal, seeds.19 Furthermore, calcium-rich recipes like multi-millet flatbread, sprout mix, soybean pulao (rice preparation with soybean), amaranth leaves-soy cutlet, were found to increase bioavailable calcium contents satisfying more than one-third of the RDA of children and adolescents.20
Local under-utilized food crops in Africa i.e., sweet potato, avocado pear, and turkey berry, were used in different proportions to develop nutrient-dense vegetable flours. The optimal composite flour was found to be the one made up of 40% sweet potato, 35% avocado pear, and 25% turkey berry. The functional properties of the composite flours were better than the control (sweet potato flour). Thus, food-to-food fortification of local flours is feasible and could be an easy and affordable means to improve rural nutrition.21
At household level, production and consumption of vitamin A–rich fruits and vegetable and small-animal production activities has a benefit of improving micronutrient status of both mothers and children.22 For Bangladeshi toddlers, thirty-five recipes were developed from local food items for complementary feeding practices and were found to be acceptable by children.23
All these studies indicate the strength of modest changes in selection of foods and proper cooking methods to fulfil daily micronutrient requirements. This approach is of great value in designing complementary feeding and school feeding programs for children as well as for families at household level.
Food-based interventions
Twenty-four randomised controlled trials (RCTs) are divided according to effects of dietary changes on children’s growth, body composition, biomarkers and cognitive function (Table 2).
 |
Table 2: Randomized Controlled Trials evaluating growth, body composition, biomarkers and cognitive function in response to dietary intervention. |
Growth parameters
As a nutritional supplement, ready-to-use foods (RUFS) were locally developed using rice-lentil or chickpea, to be similar in macro- and micronutrient composition to Plumpy’doz (soy-lipid-based nutrient supplement) for 6-18 months Bangladeshi children.24 Both RUFS contained sugar, soybean oil and whole-milk powder. Results indicated that RUFS with chickpea and rice-lentil supplementation were equally effective as Plumpy’doz in significant increases in length (of 0.06 cm/month) to 0.09 cm/month) and in weight (of 0.02 kg/month to 0.04 kg/month) relative to the control. Further RUFS significantly reduced linear growth deceleration. The prevalence of stunting at 18 months of age decreased by 4–6% over and above nutrition counselling alone (control group). This underlines the efficacy of local nutrient-rich foods in promoting growth. Promotion of such nutritious, culturally appropriate and acceptable products may be important in food-insecure settings in addition to other strategies for lessening the large burden of childhood stunting in South Asia.
Snacks using iron-rich foods, when cooked in iron pot have additional contents of contaminated iron. A beneficial effect of these snacks on iron status and growth was observed in preschool children, which also indicated that contaminated iron is bioavailable.25
A community-based intervention trial was conducted for 10 months in rural and urban malnourished children (6–59 months) from Iran. Complementary foods; i.e., poultry, meat, rice, yogurt, lentils, pinto beans and oil along with nutrition education showed improved growth status of the malnourished children.26 In Indonesian rural infants and children (5.8–28.7 months), giving local food-based recipes for complementary feeding also showed improved nutritional status. Further, it is expected to have a positive impact on the knowledge and maternal skills for weaning independently. 27
Mid-day school-meals in peri-urban region of Karnataka, India, were modified to include finger millet and pearl millet in place of rice along with pigeon pea for better nutritional outcomes. In a 3-months RCT, millet-based mid-day meals were fed to 136 schoolchildren, with 107 control children from other schools receiving usual fortified rice-based mid-day meal.28 The millet-based meals were providing balanced micro and macronutrients than the fortified rice-based meals. Furthermore, a significant improvement in stunting and body mass index (BMI) was observed in the intervention group but not in the control group suggesting the need for proper formulation of school meals.
Body composition
Bangladeshi children receiving Plumpy’doz and chickpea foods showed higher total fat free mass (FFM) and fat mass (FM) relative to the control group. While the group receiving WSB++ (marketed fortified food supplement containing wheat and soy flour, vegetable oil, vitamins, minerals, sugar and milk) showed no impact on FM and FFM. In line with the impact on linear growth, magnitude of increase in FFM was ∼2 times greater than the increase in FM. However, the benefits of the intervention did not persist 6 months after the intervention ended.29
Calcium supplementation through fortified or non-fortified millet-nuts sweet snack for one-year increased bone mass and promoted growth in Indian preschool children indicating the importance of adequate dietary calcium intakes for bone development.30
In a feeding intervention trial, for three school terms during 2 years, Kenyan school-children were given three isoenergetic supplements of meat, milk, and plain githeri, with control group receiving no supplement. The meat group showed the steepest rates of gain in mid upper arm circumference (MUAC) and mid-upper-arm muscle area (MAMA) over time, the milk group showed the next largest significant MUAC and MAMA gain compared with the plain githeri and control groups.31
In a 2-y placebo-controlled intervention trial, the effect of calcium-rich food supplements as against calcium and vitamin D tablet on bone parameters were assessed in girls (10-12 years, at Tanner stage I to II). By eligibility criteria, girls having dietary calcium intakes <900 mg/d were assigned to four groups. At the baseline, there were no significant group differences with respect to growth variables, daily nutrient intakes including calcium and hormonal concentrations. Increasing calcium intake from food is found to be more beneficial for bone mass accrual, specifically for cortical thickness of the tibia, than use of tablets containing a similar amount of calcium.32
To assess the effect of dairy supplement on bone mass accrual during puberty, an 18-month RCT was conducted in overweight and healthy-weight girls and boys. No significant advantage of extra dairy servings was seen for the change of bone mineral density, bone mass or bone area for the total-body radius, lumbar spine, and total hip. This study suggests that 2 cups milk or the dairy equivalent is adequate for normal bone gain between ages 8 and 16 year.33
Micronutrient deficiencies are linked to a higher risk of overweight and obesity and other debilitating diseases, which can also have long-term consequences including risk of hypertension in adolescents.34 Antioxidant micronutrients, i.e., vitamin C, E, b-carotene and zinc play a role in hypertension and metabolic syndrome.35 In a RCT for 4 months, 74 overweight school-children were assigned to 3 intervention groups; diet-exercise counselling with multivitamin-zinc supplementation, diet-exercise counselling and placebo. The study demonstrated a significant reduction of about 3-4% in BMI, waist circumference and body fat%. Moreover, favourable changes were observed in arterial stiffness with multivitamin-zinc supplementation together with lifestyle than lifestyle alone.36
Effect of moderate hypocaloric Mediterranean diet with nutritional education was evaluated in children and adolescents with abdominal obesity. Intake of calcium, iodine and vitamin D were high in the intensive care group with enhanced compliance with recommendations.37 Both intensive and usual care groups achieved a significant reduction in BMI for age Z score (BAZ), blood glucose and total cholesterol levels.
Biomarkers
In a 6-months intervention trial, variety of foods with high nutritional quality were introduced in rural Malawian households having stunted children (30–90 months old). The changes were made in food selection patterns and modifications in food processing of maize-based diets. Intervention group received significantly more animal-source foods, especially soft-boned fish, and foods having less phytic acid contents. Results indicated that careful selection of locally available foods combined with modifications of household food preparation practices reduced phytate intake, phytate/zinc and phytate/iron molar ratios and increased dietary intakes of protein, calcium, zinc and vitamin B12, even in rural households with very limited resources. Intervention also resulted in reducing anaemia and common infections.38
New Zealand toddlers diet was modified to include red meat, or fortified milk or non-fortified milk (placebo). In the meat group zinc intakes significantly increased by 0.8 mg/d (95% CI: 0.5, 1.1) and 0.7 mg/d (95% CI: 0.2, 1.1) in the fortified milk group as against a decrease of -0.5 mg/d (95% CI: -0.8, -0.2) in the placebo group.39 However, this modest 14–15% increase in zinc intake was not associated with a corresponding increase in serum or hair zinc concentrations during a 20-week period. Similar results are observed with red meat interventions in America and Kenya and with fortified milk interventions in Chile and Mexico.40-43 This might have happened because; i) children may not be zinc deficient, ii) both serum and hair zinc indices are insensitive measures of change in zinc status in mild zinc deficiency, and iii) coexisting multiple micronutrient deficiencies. Hence, a proper combination of foods providing multiple micronutrients may be more effective rather than a single food intervention.
Spirulina, a good source of β-carotene, was supplemented in daily meals of school-children in rural China for 5 d/week for 10 weeks. Total-body vitamin A stores of the children increased significantly, with a median increase of 0.160 mmol in children taking 2 g spirulina and of 0.279 mmol in children taking 4 g spirulina.44
African leafy vegetables (ALV) were included in the school-meals of south African children. Children were randomly allocated to receive either a 300 g cooked ALV dish with corn starch school-meal or the normal school-meal five times per week for three months. Results indicated that ALV were unable to improve serum retinol, serum ferritin or haemoglobin in case of children having mild deficiencies. Furthermore, despite low zinc status in the study population, ALV consumption did not improve serum zinc concentrations. When adjusted for baseline value, sex, age, school and adherence, no intervention effect of ALV consumption was found on iron, vitamin A and zinc status of children. This might be due to phytate contents in the accompanying corn starch meal, which inhibited absorption of zinc and iron. Daily consumption of mandatory fortified maize-meal porridge and bread, mild deficiencies of iron and vitamin A in the children and relatively short duration of the intervention could have contributed towards the lack of intervention effect.45 This highlights the need for appropriate preparation methods of ALV to increase micronutrient bioavailability.
Relative calcium absorption of i) calcium-rich millet–legume pancake of fermented and malted flour, and ii) same snack fortified with galacto-fructo-oligosaccharide (G-FOS), was evaluated with a standard calcium carbonate supplement in Indian adolescent girls. The study demonstrated that calcium absorption from pancakes was on par with standard calcium supplement. G-FOS fortification of pancakes increased the fatty acid content of food, which further improved calcium absorption.46
Among adolescent girls, 4 weeks of nutrition education combined with an increase in the content and bioavailability of dietary iron for 22 weeks resulted in significantly higher haemoglobin and serum ferritin values in the intervention group than in the control (122 vs.112 g/L, p = .0002 and 32 vs.19 µg/L, p=0.04, respectively). Prevalence of anaemia (32% vs. 85%, p=0.005) and iron-deficiency anaemia (26% vs. 56%, p=0.04) were also significantly lower in the intervention group than in the control group indicating effectiveness of the dietary intervention.47
Children with type-1 diabetes were observed to have compromised antioxidant status as compared to healthy controls. To alleviate their antioxidant status, five snacks; whole wheat-GLV thin crackers, puffed rice with nuts; popped amaranth seeds, sesame sweet balls and fruit-vegetable salad were used as diet supplements. These snacks were rich in antioxidant micronutrients; zinc, b-carotene and vitamin C. Results of the three months RCT indicated that micronutrient supplementation helped to improve antioxidant status of diabetic children, but it was still lower than the healthy controls.48 Though the study duration and sample size are small, these strategies exhibit the potential to alleviate antioxidant micronutrient status in type-1 diabetic children. Furthermore, increasing dietary micronutrient intakes of type-1 diabetic patients may be helpful for avoiding diabetes-related complications.
The school snacks in Kenyan children were devised by augmenting their traditional vegetable dish ‘githeri’ (type of stew) with meat or milk, to increase intakes of mainly animal-source protein, available zinc, available iron and vitamin B12. The impact of the school snacks resulted in significant increase in folate, iron, available iron, energy per body weight, vitamin B12, zinc and riboflavin intake. Moreover, there was a decline in upper respiratory infections.49
Cognitive function
In a 10-weeks intervention study, school girls were fed freshly prepared snacks from zinc-rich foods; millets, pumpkin seeds, sesame, soyabean, chick pea, GLV and using soaking, fermentation, and sprouting to enhance zinc bioavailability. Girls were given either snacks (D-group), or ayurvedic zinc tablet (J-group), or no supplement (control), for 6 days/week. Improvement in plasma zinc levels was seen in J group (61.3%) and D group (9%), while cognitive performance improved by 29.6% (J-group) and 24.5% (D-group) and taste recognition threshold for salt by 50% in both intervention groups as against little or no change in the control group. 50
The school snacks for Kenyan children were devised by augmenting their traditional vegetable dish ‘githeri’ with meat or milk, to increase intakes of mainly animal-source protein, available zinc, available iron and vitamin B12. The impact of the school snacks resulted in significantly better test scores in key academic subjects (Arithmetic, English, Kiswahili and Geography) and total test scores compared with the control group.51
Two-year longitudinal, randomised controlled feeding intervention study using animal-source foods was carried out in children from twelve primary schools in rural Kenya. The schools were randomised in four groups: 1) control (no food supplement); 2) vegetarian supplement (traditional local dish (githeri) of maize, beans and vegetables; 3) milk supplement (githeri plus 200 ml of whole cow’s milk); 4) meat supplement (githeri with 60 g minced beef). The response to four cognitive tests; Raven’s Coloured Progressive Matrices (RCPM), a verbal meaning test, an arithmetic test and digit span (DS)-forward, DS-backward tests, food intake by 24-h recall and morbidity recall were recorded. Interventions resulted in increased intakes of available iron and zinc, vitamin B12 and riboflavin, which had significant beneficial effects on cognitive performance.52
Modification of food provision and dining environment was introduced in secondary school pupils for 15 weeks. Intervention group improved learning-related behaviours in the post-lunch period than the controls.53
Conclusion
This review presents scientific evidence regarding impact of food-based interventions with dietary modification/diversification to improve micronutrient status and associated health outcomes in children from 6 months to 16 years. The food products/ recipes developed in the twelve studies were found to increase the micronutrient contents many-fold as compared to the routine diet/snacks. Two studies demonstrated that the new recipes had a greater in vitro dialysability indicating possible increase in absorption. However, the age-groups in these studies range from 6 months 16 years. Therefore, more studies on formulating age-specific recipes/food supplements are necessary.
Twenty-four food-based intervention studies reported positive impact on micronutrient status and various parameters of growth and health of children and adolescents. Among studies assessing effect on growth parameters, four were in young children and one was in adolescents. There was an improvement in HAZ scores except in Indonesian children. This might be the result of difference in study duration, age group and study design.
Positive effects on bone mass content in school-children and on FFM in infants have been observed after food supplementation in six studies but no effect of dairy supplement was seen in one study in spite of longer duration.
Improvement in micronutrient intakes and biomarkers have been observed in six studies. However, no change was reported not in South African and New Zealand children. Whereas cognitive performance was enhanced after food supplements in all the four studies.
For alleviating micronutrient deficiencies, common strategies implemented are short-term supplementation of fortified foods or multivitamin-mineral tablets. However, the present review highlights the need for long-term strategy based on food-based interventions including dietary diversification with life style modifications to improve micronutrient status and health of growing children. One of the limitations of this review is that number of food-based intervention studies are scarce in literature. Therefore, a small and heterogeneous set of studies could be included in the review. More rigorously designed intervention trials with dietary diversification or modification are necessary in vulnerable age groups for sustainable health benefits and functional outcomes. Key pointers for improvement in micronutrient status of children that emerge from the review are:
- Dietary diversification by improving the nutrition knowledge of mothers/caregivers.
- Dietary modification by including local micronutrient-rich foods
- Improving bioavailability of micronutrients of food products/recipes through sprouting/ malting/
fermentation processes.
Acknowledgement
The principal author Dr. Chiplonkar would like to acknowledge the assistance of the co- authors (Dr. Sanwalka and Dr. Kajale) in the literature search, getting full texts of the selected articles and finalising the manuscript.
Conflict of Interest
All authors declare no conflicts of interest.
Funding Sources
There is no funding sources
References
- Kramadhati Venkata, Rameshwar Sarma. An Essential Aid to Daily Growth in Children. Indian Pediatrics. Micronutrients 2009; 46 Suppl. s12-9.
CrossRef - Bailey RL, West Jr. KP, Black RE. The Epidemiology of Global Micronutrient Deficiencies. Ann Nutr Metab. 2015; 66 Suppl 2:22-33.
CrossRef - Thompson B. Food-based approaches for combating iron deficiency. In: Zimmermann MB, Hurrel RF, eds. Nutritional Anemia. Basel, Switzerland: Sight and Life Press: 2007;337–58.
CrossRef - World Health Organization and Food and Agricultural Organization of the United Nations. Evaluating the public health significance of micronutrient malnutrition. In Allen L, Benoist B de, Dary O, Hurrell R, eds. Guidelines on food fortification with micronutrients. Geneva: World Health Organization; 2009. Available from: http://www.unscn.org/layout/modules/resources/files/fortification_eng.pdf.
- Allen LH. To what extent can food-based approaches improve micronutrient status? Asia Pac J Clin Nutr. 2008;17 Suppl 1:103-105.
- Gibson, R. S. Enhancing the Performance of food-based strategies to improve micronutrient status and associated health outcomes in young children from poor-resource households in low-income countries: challenges and solutions. In Brian Thompson, Leslie Amoroso, eds. Improving Diets and Nutrition: Food–based Approaches. Rome, Italy CAB International and FAO Food and Agriculture Organization of the United Nations (FAO). 2014: 19–31.
- Teye E, Deha CI, Dadzie R, MacArthur RL. Delivering the Nutritional Needs by Food to Food Fortification of Staples Using Underutilized Plant Species in Africa. Int J Food Sci. 2020; 2020:8826693.
- Tupe RP, Chiplonkar SA. Diet patterns of lactovegetarian adolescent girls: need for devising recipes with high zinc bioavailability. Nutrition. 2010;26(4):390-398.
- Keller, I. and Tukuitonga, C. The WHO/FAO fruit and vegetable promotion initiative. Acta Hortic. 2007;744:27-37.
- Darfour-Oduro SA, Buchner DM, Andrade JE. Grigsby-Toussaint DS. A comparative study of fruit and vegetable consumption and physical activity among adolescents in 49 Low-and-Middle-Income Countries. Sci Rep: 2018;8(1):1623.
- Agte VV, Tarwadi KV, Mengale S, Chiplonkar SA. Potential of Traditionally Cooked Green Leafy Vegetables as Natural Sources for Supplementation of Eight Micronutrients in Vegetarian Diets. J Food Comp Anal. 2000;13(6): 885-891.
- Chiplonkar SA, Tarwadi KV, Kavedia RB, Mengale SS, Paknikar KM, Agte VV. Fortification of vegetarian diets for increasing bioavailable iron density using green leafy vegetables. Food Res Intern. 1999;32 (3):169-174.
- Parthasarathy LS, Chiplonkar SA, Khadilkar AV, Khadilkar VV. Dietary modifications to improve micronutrient status of Indian children and adolescents with type 1 diabetes. Asia Pac J Clin Nutr. 2015; 24(1):73-82.
- Glover-Amengor M, Aryeetey R, Afari E, Nyarko A. Micronutrient composition and acceptability of Moringa oleiferaleaf-fortified dishes by children in Ada-East district, Ghana. Food Sci Nutr. 2016;5(2):317-323.
- Gupta Alka, Verma Sushila, Sheikh Sarita, Ranu Prasad, Yadav Neelam. Development of micronutrient rich food product by using indigenous coarse grains and green leafy vegetables. International Journal of Food and Nutritional Sciences. 2015; 4(4): 109-111.
- Wu Q, van Velthoven MH, Chen L, Car J, Rudan D, Saftić V, Zhang Y, Li Y, Scherpbier RW. Improving the intake of nutritious food in children aged 6-23 months in Wuyi County, China — a multi-method approach. Croat Med J. 2013;54(2):157-70.
- Pettifor JM. Calcium and vitamin D metabolism in children in developing countries. Ann Nutr Metab. 2014;64 Suppl 2:15-22.
- Chiplonkar S, Khadilkar A, Pandit-Agrawal D, Kawade R, Kadam N, Ekbote V, Sanwalka N, Khadilkar V. Influence of micronutrient status and socioeconomic gradient on growth indices of 2-18-year-old Indian girls. J Pediatr Endocrinol Metab. 2013;26(9-10):825-32.
- Sanwalka NJ, Khadilkar AV, Chiplonkar SA. Development of non-dairy, calcium-rich vegetarian food products to improve calcium intake in vegetarian youth. Current Science. 2011;101(5):657-663.
- Ekbote VH, Khadilkar AV, Khadilkar VV, Chiplonkar SA, Mughal Z. Dietary patterns with special reference to calcium intake in 2–16-year-old Urban Western Indian children. Indian J Public Health. 2017;61:188-193.
- Teye E, Agbemafle R, Lamptey F. Development and examination of sweet potato flour fortified with indigenous underutilized seasonal vegetables. Beverages. 2018;4(1): 5.
- Olney DK, Talukder A, Iannotti LL, Ruel MT, Quinn V. Assessing impact and impact pathways of a homestead food production program on household and child nutrition in Cambodia. Food Nutr Bull. 2009; 30(4):355-369.
- Roy SK, Jahan K, Iqbal Kabir AKM, Keya NA, Khatoon S, Mannan MA, Bhattacharjee L. Improved recipes provide better complementary feeding in young children: findings of community-based trials in Bangladesh. Eur J Clin Nutr. 2022;76:235–243.
- Christian P, Shaikh S, Shamim AA, Mehra S, Wu L, Mitra M, Ali H, Merrill RD, Choudhury N, Parveen M, Fuli RD, Hossain MI, Islam MM, Klemm R, Schulze K, Labrique A, de Pee S, Ahmed T, West KP Jr. Effect of fortified complementary food supplementation on child growth in rural Bangladesh: a cluster-randomized trial. Int J Epidemiol. 2015;44(6):1862-1876.
- Kulkarni SA, Ekbote VH, Sonawane A, Jeyakumar A, Chiplonkar SA, Khadilkar AV. Beneficial effect of iron pot cooking on iron status. Indian J Pediatr. 2013;80(12):985-989.
- Shenavar R, Sajjadi SF, Farmani A, Zarmehrparirouy M and Azadbakht L. Improvement in Anthropometric Measurements of Malnourished Children by Means of Complementary Food and Nutritional Education in Fars Province, Iran: A Community-Based Intervention. Front. Nutr. 2022; 9:813449.
- Susanto T, Syahrul, Sulistyorini L, Rondhianto, Yudisianto A. Local-food-based complementary feeding for the nutritional status of children ages 6-36 months in rural areas of Indonesia. Korean J Pediatr. 2017 Oct;60(10):320-326.
- Anitha S, Kane-Potaka J, Tsusaka TW, Tripathi D, Upadhyay S, Kavishwar A, Jalagam A, Sharma N, Nedumaran S. Acceptance and Impact of Millet-Based Mid-Day Meal on the Nutritional Status of Adolescent School Going Children in a Peri Urban Region of Karnataka State in India. Nutrients. 2019;11(9):2077.
- Shaikh S, Campbell RK, Mehra S, Kabir A, Schulze KJ, Wu L, Ali H, Shamim AA, West KP, Christian P. Supplementation with fortified lipid-based and blended complementary foods has variable impact on body composition among rural Bangladeshi children: a cluster-randomized controlled trial. J Nutr. 2020;150(7):1924-1932.
- Ekbote VH, Khadilkar AV, Chiplonkar SA, Hanumante NM, Khadilkar VV, Mughal MZ. A pilot randomized controlled trial of oral calcium and vitamin D supplementation using fortified laddoos in underprivileged Indian toddlers. Eur J Clin Nutr. 2011;65(4):440-6.
- Neumann CG, Jiang L, Weiss RE, Grillenberger M, Gewa CA, Siekmann JH, Murphy SP, Bwibo NO. Meat supplementation increases arm muscle area in Kenyan schoolchildren. Br J Nutr. 2013;109(7):1230-1240.
- Cheng S, Lyytikäinen A, Kröger H, Lamberg-Allardt C, Alén M, Koistinen A, Wang QJ, Suuriniemi M, Suominen H, Mahonen A, Nicholson PH, Ivaska KK, Korpela R, Ohlsson C, Väänänen KH, Tylavsky F. Effects of calcium, dairy product, and vitamin D supplementation on bone mass accrual and body composition in 10-12-y-old girls: a 2-y randomized trial. Am J Clin Nutr. 2005;82(5):1115-1148.
- Vogel KA, Martin BR, McCabe LD, Peacock M, Warden SJ, McCabe GP, Weaver CM. The effect of dairy intake on bone mass and body composition in early pubertal girls and boys: a randomized controlled trial. Am J Clin Nutr. 2017;105(5):1214–1229.
- McNaughton SA, Ball K, Mishra GD, Crawford DA. Dietary patterns of adolescents and risk of obesity and hypertension. J Nutr. 2008;.138:364-370.
- Houston MC. The role of cellular micronutrient analysis, nutraceuticals, vitamins, antioxidants and minerals in the prevention and treatment of hypertension and cardiovascular disease. Ther Adv Cardiovasc Dis. 2010;4(3):165-183.
- Khadilkar VV, Pandit DS, Khadilkar AV, Chiplonkar SA, Kinare AS. Diet and exercise intervention, with special reference to micronutrients, reduces cardiometabolic risk in overweight children. Indian J Endocr Metab. 2012;16(1):124-133.
- Ojeda-Rodríguez A, Zazpe I, Morell-Azanza L, Chueca MJ, Azcona-Sanjulian MC, Marti A. Improved Diet Quality and Nutrient Adequacy in Children and Adolescents with Abdominal Obesity after a Lifestyle Intervention. Nutrients. 2018;10(10):1500.
- Gibson RS, Yeudall F, Drost N, Mtitimuni BM, Cullinan TR. Experiences of a community-based dietary intervention to enhance micronutrient adequacy of diets low in animal source foods and high in phytate: a case study in rural Malawian children. J Nutr. 2003;133(11 Suppl 2):3992S-3999S.
- Morgan EJ, Heath AL, Szymlek-Gay EA, Gibson RS, Gray AR, Bailey KB, Ferguson EL. Red meat and a fortified manufactured toddler milk drink increase dietary zinc intakes without affecting zinc status of New Zealand toddlers. J Nutr. 2010;140(12):2221-2226.
- Krebs NF, Westcott JE, Butler N, Robinson C, Bell M, Hambidge KM. Meat as a first complementary food for breastfed infants: feasibility and impact on zinc intake and status. J Pediatr Gastroenterol Nutr. 2006;42:207–214.
- Siekmann JH, Allen LH, Bwibo NO, Demment MW, Murphy SP, Neumann CG. Kenyan school children have multiple micronutrient deficiencies, but increased plasma Vitamin B-12 is the only detectable micronutrient response to meat or milk supplementation. J Nutr. 2003;133(11 Suppl 2):3972S–3980S.
- Torrejo´n C, Castillo-Dura´n C, Hertrampf E, Ruz M. Zinc and iron nutrition in Chilean children fed fortified milk provided by the complementary national food program. Nutrition. 2004;20:177–80.
- Villalpando S, Shamah T, Rivera JA, Lara Y, Monterrubio E. Fortifying milk with ferrous gluconate and zinc oxide in a public nutrition program reduced the prevalence of anemia in toddlers. J Nutr. 2006;136: 2633–7.
- Li L, Zhao X, Wang J, Muzhingi T, Suter PM, Tang G, Yin SA. Spirulina can increase total-body vitamin A stores of Chinese school-age children as determined by a paired isotope dilution technique. J Nutr Sci. 2012;1:e19.
- van der Hoeven M, Faber M, Osei J, Kruger A, Smuts CM. Effect of African leafy vegetables on the micronutrient status of mildly deficient farm-school children in South Africa: a randomized controlled study. Public Hlth Nutr. 2016;19(5):935-945.
- Sanwalka NJ, Khadilkar AV, Chiplonkar SA, Khadilkar VV, Mughal MZ. Galacto-fructo-oligosaccharide fortification of fermented non-dairy snack enhances calcium absorption in healthy adolescent girls. Int J Food Sci Nutr. 2012;63(3):343-352.
- Alaofè H, Zee J, Dossa R, O’Brien HT. Education and improved iron intakes for treatment of mild iron-deficiency anemia in adolescent girls in southern Benin. Food Nutr Bull. 2009;30(1):24-36.
- Parthasarathy L, Khadilkar V, Chiplonkar S, Khadilkar A. Effect of Antioxidant Supplementation on Total Antioxidant Status in Indian Children with Type 1 Diabetes, J Dietary Suppl. 2018; 9;16(4):390-400.
- Neumann CG, Bwibo NO, Jiang L, Weiss RE. School snacks decrease morbidity in Kenyan schoolchildren: A cluster randomized, controlled feeding intervention trial. Public Hlth Nutr. 2013;16(9):1593-1604.
- Tupe RP, Chiplonkar SA. Zinc supplementation improved cognitive performance and taste acuity in Indian adolescent girls. J Am Coll Nutr. 2009;28(4):388-396.
- Hulett JL, Weiss RE, Bwibo NO, Galal OM, Drorbaugh N, Neumann CG. 2014. Animal source foods have a positive impact on the primary school test scores of Kenyan schoolchildren in a cluster-randomised, controlled feeding intervention trial. Br J Nutr. 2015;111(5):875-886.
- Gewa CA, Weiss RE, Bwibo NO, Whaley S, Sigman M, Murphy SP, Harrison G, Neumann CG. Dietary micronutrients are associated with higher cognitive function gains among primary school children in rural Kenya Dietary micronutrients are associated with higher cognitive function gains among primary school children in rural Kenya. Br J Nutr. 2009;101(9):1378-1387.
- Storey HC, Pearce J, Ashfield-Watt PA, Wood L. Baines E, Nelson M. A randomized controlled trial of the effect of school food and dining room modifications on classroom behaviour in secondary school children. Eur J Clin Nutr. 2011;65(1):32-38.

This work is licensed under a Creative Commons Attribution 4.0 International License.