A Review of The Contribution of Gut-Dependent Microbiota Derived Marker, Trimethylamine N-oxide (TMAO), in Coronary Artery Disease
Vasanth Konda Mohan and Melvin George*
and Melvin George*
Department of Clinical Pharmacology, SRM Medical College Hospital and Research Centre, Kattankulathur, Chennai, India.
Corresponding Author Email: melvingeorge2003@gmail.com
DOI : http://dx.doi.org/10.12944/CRNFSJ.9.3.01
Download this article as:
![]()
Coronary artery disease (CAD) has a high prevalence and one of the principal drivers of mortality worldwide. Therefore, there is a requirement to develop sensitive diagnostic biomarkers, disease progression control and therapeutic stratification in order to keep a check on the disease rate. Atherosclerosis is a systemic disease, the main cause of heart disease, is associated with hyperlipidemia and lipid oxidation and has always been a common single leading cause of death in well-developed countries. In the attempts to study CAD and the causative agents for the disease, a metabolite circulating in the plasma termed trimethylamine-N-oxide (TMAO) has been found out to be an independent risk factor that increases CAD risk. The use of a metabolomic approach has proven useful in the recent past, as it can aid in the identification and quantification of several metabolites that play a crucial role for diagnosis and exploring therapeutic targets. TMAO is majorly synthesized by a process which involves the bioconversion of gut microbiota and hepatic flavin monooxygenases (FMOs) from nutrient-containing dietary trimethylamine (TMA). TMA is synthesized by gut bacterial fermentation from the components present in meat such as phosphatidylcholine (PC), betaine, choline, and L-carnitine. It can accentuate the process of atherosclerosis through the novel meta-organismal metabolic pathway. TMAO leads to atherogenesis by increasing vascular inflammation, reducing vascular functions and disrupting cholesterol homeostasis at various levels. This review article attempts to summarize the pool of evidence collected on the microbiota-dependent TMAO and its association with atherosclerosis. We performed literature search with Medline, PubMed, and Google Scholar, on “TMAO in CAD”, “metabolites in CAD” and “TMAO in other diseases” from the year 1990 to 2020. Although the circulatory TMAO has been identified as an independent marker for CAD, there is still no conclusive evidence to justify its role as a routine marker for CAD diagnosis. Future research must clarify the mechanisms which underpin these complex associations to determine if there is a causal link exists between TMAO and CAD.
Introduction
Coronary artery disease (CAD), is one of the primary causes of death that involves the formation of fatty deposits or plaque on the interior of the arteries of the heart (coronary arteries). The formation of plaque (mostly cholesterol deposits) within the arteries is called atherosclerosis. Its clinical sequelae including myocardial infarction and heart failure are one of the major morbidity and mortality.1 In the last six decades, CAD has, unfortunately, become the largest driver of mortality in India, and has risen from 1% in 1960 to 14% in 2011.2 By the year 2030, the mortality in the Indian subcontinent among individuals below the age of 60, will increase to approximately 17.9 million; data recorded to be higher than that of China, Russia, and the even USA.3
Owing to the complexity of the disease, the underlying mechanisms regarding the more probable development of coronary macrovascular complications in CAD are yet to be entirely comprehended.4 It is well-known that CAD is linked with complex metabolic disorders, such as insulin resistance, diabetes, and obesity.5 Circulating metabolites, such as homocysteine, cholesterol, and triglycerides, have been well established in CAD.6-8 However, it is still puzzling as to how mechanistically these risk factors induce atherosclerosis, and whether independent pathways exist that circumvent these conventional factors altogether.9
Growing evidence has continued to emerge concerning the development of atherosclerosis with respect to gut microbiota alterations. Trimethylamine-N-oxide (TMAO), a major intestinal microbial metabolite, is derived from dietary choline, betaine, and L-carnitine. It gets metabolized to trimethylamine (TMA) by the microbiota of the gut following which, it is further rapidly oxidized into TMAO by hepatic flavin monooxygenases (FMOs) (Equation 1).10 TMAO is a small organic compound, that is present in certain food items such as fish, poultry, red meat, and dairy products.11 The association between atherosclerosis and TMAO has been explored by recent metabolomics and animal studies.12,13
This article compiles the recent developments of gut-dependent microbiota-derived TMAO as an important participant in atherosclerosis and the role it plays in increasing the predilection leading to adverse cardiac events. Additionally, the article also addresses the approach in targeting gut-dependent microbiota and the recently recognized metabolic pathways involved in the formation of trimethylamine – N-oxide (TMAO) for potential CAD prevention and treatment.
Methodology
Search Strategy
We performed literature searches of research papers indexed in PubMed (including MEDLINE through NCBI) and Google scholar systematically. Broadly, the search strategy combined the following key search terms: “TMAO AND CAD”, “metabolites AND CAD” and “TMAO in other diseases” from the year 1990 to 2020. References of retrieved articles were reviewed for additional citations.
Inclusion Criteria
In this analysis, the included studies were to contain the following details i) data analysis on a defined CAD population as an entire cohort or a stratified subset of the mixed cohort; ii) TMAO as an indicator of risk for CAD, either as a single baseline or longitudinal measurements; iii) a measure of association (or ability to calculate) between TMAO and CAD.
Exclusion Criteria
Non-English articles, animal model studies, in-vitro studies, review articles, editorials, commentaries, and duplicate articles were excluded.
Origin and Metabolism of TMAO
The hepatic Flavin-containing monooxygenases (FMO) oxidize the TMA and forms TMAO, a small odorless molecule (MW 75.22g/mol).14,15 Five members of the FMO family are found in humans (FMO1-FMO5), and among them, the oxidation of TMA to TMAO can be catalyzed only by FMO1 and FMO3.16 FMO3 is the major hepatic isoform and it has been noted that certain uncommon deleterious mutations in the FMO3 gene can lead to reduced or no TMAO formation which in turn results in TMA accumulation.17-19 This is known as trimethylaminuria, an autosomal recessive condition, which is also referred to as “fish malodor syndrome” (OMIM 602079).20
Individuals with this syndrome tend to emit foul odors in their urine, sweat, and breath that resemble the smell of rotten fish.21 TMA is generated in the colon by the gut microbiome originating from dietary quaternary ammonium compounds (such as phosphatidylcholine/choline,22 carnitine,12 betaine23), in case they fail to be completely absorbed by the intestinal wall during digestion. TMAO in the blood is mainly eliminated by urinary excretion as well as sweat and breath.24-27 Individuals excrete aliphatic amine TMA in rare metabolic disorders such as primary trimethylaminuria (TMAU), instead of TMAO.28
Equation: Oxidation of TMA to TMAO Catalyzed by the Enzyme Hepatic FMO3.
![]()
Correlation between CAD and TMAO
Atherosclerosis is a condition in which, the inner walls of the arteries tend to become thicker than their normal width and undergo fatty degeneration which causes a reduction in the blood flow.29 The high plasma level of TMAO potentiates the risk of cardiovascular events in established CAD.11 Patients with CAD usually show higher concentrations of the TMAO. Several investigations have revealed that TMAO seems to serve as a biomarker in patients for predicting the prevalence of CAD and increased incidence of major adverse cardiovascular events (MACE), such as recurrent heart failure, stroke, and mortality.30-32
The association between circulatory TMAO and CAD risk was first revealed in a study by Wang et al.22 In this analysis, a targeted metabolomics approach was used to measure the plasma metabolites such as choline, betaine, and TMAO. Measured levels of these metabolites predict the risk of CVD among subjects. An epic pathway has been explained which links the dietary intake of lipids with intestinal micro-flora and atherosclerosis. The identified pathway for TMAO formed by dietary PC/choline through the metabolism of gut-flora is a significant additional nutritional contribution to the pathogenesis of CAD, involving PC and choline metabolism, which plays an essential role for the intestinal microbial population as well as in regulating the surface expression rates of macrophage scavenger receptors known to participate in the atherosclerotic process (Fig 1).
Several studies have opined that increased blood TMAO level is associated with increased CVD risk, consistent with the findings from Wang et al. In 2013, the plasma and urinary levels of TMAO, betaine and choline were estimated by using liquid chromatography procedure and online tandem mass spectrometry. In this study, authors found that the elevated plasma concentration of TMAO had a moderate association with increased incident risks for major cardiovascular events, independent of identified risk factors, and suggested that the intestinal microbes are active in the metabolism of phosphatidylcholine to form circulating plasma and urinary TMAO.33
In another study, TMAO was estimated in Chinese subjects with CAD including those with and without concomitant diabetes. Measurement was carried out by LC-MS/MS and it was observed that the TMAO plasma levels were significantly higher in patients with CAD as compared to subjects in the control group. It was also found out that the plasma levels of TMAO in patients with T2DM associated with CAD were significantly higher than in CAD patients without T2DM.34
In 2019, a study measured the concentration of TMAO by mass spectrometry which was then evaluated for its association with the severity and prognosis of peripheral artery disease. The said study included 262 symptomatic peripheral artery disease (patients (mean age 70 years, 87% men) categorized as intermittent claudication (IC, n = 147) and critical limb ischemia (CLI, n = 115), all of whom were followed up for a mean average of 4 years (min 1-max 102 months). In the study’s result, an increased level of TMAO according to PAD severity as well as an independent association between TMAO and CV mortality were identified. The design of novel therapeutic approaches for gut-derived metabolite regulation in vascular patients needs to be considered not only for intestinal bacterial function but also for the role of key hepatic enzymes for TMA oxidation (FMO3), as well as renal function.35 It has been indicated that increased plasma O concentration in patients who are affected by coronary heart disease was strongly correlated with heavy atherosclerotic stress and can also raise the MACE risk in patients living with CHD by 58%. Additionally, it has been proposed that the TMAO concentration of 5.1 μmol/L may be the ideal cut-off value for prognostication.36
The concentration of TMAO can be associated with many other diseases as well. The elevated serum TMAO level has been associated with advanced chronic kidney disease (CKD) stages as well as an increased number of infarcted coronary arteries in patients undergoing cardiovascular surgery.25 It has been observed that patients with CKD having elevated plasma TMAO levels show a higher risk of all-cause mortality.37 In 2014, Bae et al have stated that plasma TMAO has a positive association with colorectal cancer risk in postmenopausal women.38
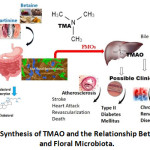 |
Figure 1: Synthesis of TMAO and the Relationship Between Diet and Floral Microbiota. |
Circulating TMAO as Biomarkers of Coronary Artery Disease
A series of cohort studies have demonstrated that raised TMAO levels in patients with either stable CAD or acute coronary syndrome are associated with an increased risk of cardiovascular disease and poor cardiac outcomes.36,39,40 In a recent study, it was revealed that elevated plasma TMAO levels have an association with plaque rupture in patients with CAD. In patients with -segment – elevation myocardial infarction (STEMI) with plaque rupture, there was an association between plasma TMAO levels and culprit lesion morphology than in those with plaque erosion as measured by optical coherence tomography.41 In the diet‐derived, gut microbial–host co-metabolite, it was observed that urinary concentration of TMAO is associated with a higher risk for the general population developing CHD. This was also observed even after adjustment for major CVD risk factors among patients without metabolic conditions such as diabetes mellitus, hypertension, and dyslipidemia.42
Previous research found that choline or L-carnitine plasma levels were associated with TMAO levels, as well as an increased risk of major adverse cardiovascular events in patients with CAD.43 A recent study has demonstrated that TMAO has a stronger association with hemorrhagic stroke as compared to ischemic stroke. TMAO promotes vascular inflammation and endothelial cell dysfunction via various signaling pathways, thereby creating the likelihood that TMAO may play a role in hemorrhagic stroke. Nevertheless, due to the presence of a relatively smaller sample size of the hemorrhagic stroke population, their findings need to be explicitly affirmed (Table 1).44
Table 1: Summary of Studies that Explored TMAO in Cardiovascular and Related Diseases.
| Populace | Sample Size | Study Design | Main findings/outcomes | Study |
| T2DM | 1463 participants | single-center SURDIAGENE cohort | TMAO concentrations were significantly associated with diabetes duration, renal function, high-density lipoprotein cholesterol, soluble tumor necrosis factor receptor 1 (sTNFR1) concentrations (R2 = 0.27) | Croyal et al.45 |
| Untreated and combination anti-retroviral therapy treated human immunodeficiency virus (HIV)-infected individuals. | 50 untreated and 50 combinations antiretroviral therapy treated HIV-infected individuals. | cross-sectional cohort | Similar TMAO levels [3.8 (2.3–6.1), vs. 2.9 μM (1.9–4.8) P = 0.15] were observed in cART treated compared to untreated individuals infected with HIV. | Haissman et al.46 |
| CHD and T2DM patients | 132 control participants, 243 CHD patients, and 175 CHD patients with T2DM | Three classes of the subject: controls, CHD patients, and CHD patients with T2DM | In CHD patients the plasma levels of TMAO were significantly higher than in control subjects (3.08 ± 0.13 μM versus 1.49 ± 0.05 μM; P < 0 01) | Dong et al.34 |
| Peripheral Artery Disease | 262 patients with symptomatic PAD (intermittent claudication n = 147) and critical limb ischemia n = 115) | Case-control study | Patients with TMAO > 2.26 μmol/L exhibited higher risk of cardiovascular death (subhazard ratios ≥2, P < 0.05) | Roncal et al.35 |
| Healthy volunteers | N= 113 (all omnivores, 44 males and 69 females) | Crossover design study of randomized 2-arm (high- or low-saturated fat) | Chronic red meat, but not the consumption of white meat or non-meat, increased plasma and urine TMAO (each >two-fold; P < 0.0001) | Wang et al.47 |
| Peripheral artery disease (PAD) patients | 935 patients with PAD | A single-center prospective cohort study | Elevated TMAO levels were associated with 2.7-times higher mortality risk (fourth versus first quartiles, hazard ratio 2.86, 95% CI 1.82–3.97, P<0.001). | Senthong et al.48 |
| Coronary Heart Disease patients | 275 CHD-incident participants and275 individually matched controls | Nested case-control study | Urinary TMAO was associated with CHD risk but not with its precursors. The odds ratio for the highest versus lowest quartiles of TMAO was 1.91 (95% CI, 1.08–3.35; =0.008) | Yu et al.42 |
| People living with HIV (PLWH) | 175 participants | Cross-sectional analysis and a longitudinal analysis study | The median concentration of serum TMAO were 165 (103-273) ng/mL. An association was observed with age, number of antiretrovirals, serum creatinine, multimorbidity and polypharmacy | Montrucchio et al.49 |
Measurement of TMAO and its Metabolites in CAD
There are several techniques for measuring TMAO in biological samples. In 1990, dimethylamine (DMA), TMA, and TMAO were determined through the use of gas chromatography procedure coupled with the mass spectrometric detection method. These were extracted from samples of blood, urine, liver, and kidney of rats and humans, as well as from fish muscles. In this study, DMA, TMA, and TMAO have been extracted from biological samples into acid after deuterated internal standards were added (DMA-d6, TMA-d6, TMAO-d6). DMA derivative tosylamide was formed using p-Toluene sulfonyl chloride. The TMA derivative carbamate was synthesized using 2,2,2,2-Trichloroethyl chloroformate. TMAO combined with titanium (III) chloride was reduced to form TMA, which was then analyzed.50 However, there are several limitations associated with this particular strategy. TMA is highly liable to quick changes, which precludes its evaluation. Another limitation is that this technique fails to distinguish between TMA, DMA, and TMAO with ease since all produce a similar by-product. The liquid chromatography or mass spectrometry [LC/MS, electrospray ionization (ESI)] was developed to quantify nitrogen osmolytes (N-osmolytes) in the sample fractions of the natural water samples. This was validated using seawater samples of glycine, betaine, choline and TMAO.51 A study in 2018 found serum levels of TMAO were measured in samples stored at −80°C. 52 First, serum proteins were precipitated using methanol (serum: methanol, 1:2, v/v); samples were vortex-mixed for 2 min, centrifuged at 14,000 g for 10 min (4 °C)53 and High-Performance Liquid Chromatography-Mass Spectrometry (HPLC-MS) system was used to separate and analyze the supernatants. According to Beale and Airs, both HPLC-MS conditions and processes were performed.51 The HPLC system was coupled with a single quadrupole mass spectrometer equipped with an ESI source, that functioned in a positive ion mode. In combination with a guard column (HILIC), the chromatographic separation was carried out using a Luna HILIC column (150/3 mm, 5 μm particles). A recent study has authenticated a procedure for measuring urine TMA and TMAO concentration by using liquid chromatography-mass spectrometry (LC/MS) simultaneously. The TMA and TMAO in the urine can be extracted in alkaline pH using hexane/butanol and transferred for LC/MS quantification to the aqueous cycle after acidification. It is to be noted that none of the nutrients having a chemical structure with a TMA moiety were cleaved spontaneously to yield TMA during sample processing. This also showed that urine acidification prevents TMA from rising after extended storage, as was found in non-acidified urine. Finally, it was observed that TMAO can degrade spontaneously to TMA at a very slow rate.54
TMAO and the Risk of Other Diseases
Patients with type 2 diabetes mellitus (T2DM) having an increased concentration of the circulatory gut-based metabolite N-oxide (TMAO) was identified by Tang et al.55 Al-Obaide et al. have demonstrated that gut microbiota-dependent TMAO increases in patients with diabetic CKD with increased gut permeability and inflammatory as well as endothelial dysfunction.56 Serum L-carnitine level was found to be associated with an adverse metabolic syndrome profile. Moreover, in 2019, Gao et al identified the relationships between serum TMAO and L-carnitine levels with metabolic syndrome profiles, including obesity, blood pressure, serum glucose, serum lipids and insulin resistance (IR)-related index in humans.57 In this analysis, serum L-carnitine levels in males with normal fasting glucose (p<0.05 for all) had a positive correlation with serum insulin, serum triglyceride (TG), IR but only serum TG (p<0.05) in male patients with hyperglycemia. In females, significant positive correlations were seen between serum L-carnitine levels with obesity, total serum cholesterol, glucose, insulin, and IR. Serum TMAO level was only identified to be positively correlated with serum insulin level and IR in hyperglycemic males (p < 0.05 for all).57 TMAO levels were significantly associated with the percentage of pro-inflammatory intermediate CD14++CD16+ monocytes in patients with ischemic stroke.58
Research on humans and mice has shown that plasma TMAO levels increase with ageing59 and TMAO levels have been significantly associated with body mass index (BMI) in healthy adults with different risk factors.60 In particular, in untreated HIV-inflicted subjects, sCD14 was independently associated with TMAO.46 Gut microbial-related choline metabolite TMAO, as well as two monocyte activation biomarkers and inflammation biomarkers (SCD14 and sCD163), were also positively associated with carotid artery atherosclerosis in HIV patients.61
Conclusion and Future Prospects of TMAO
TMAO is an important gut-derived metabolite that contributes vital prognostic information in patients with CAD. It was shown to be helpful in predicting adverse cardiovascular events in the short term as well as long term. This was even after adjustment for traditional risk factors such as diabetes, hypertension, and obesity. Even in patients with peripheral artery disease, TMAO showed robust prognostic ability in measuring the risk of cardiovascular death. In patients with diabetes and CAD, there is a higher concentration of TMAO than in non-diabetic CAD patients. Future studies should explore it is usefulness as a pharmacological target in CAD.
Funding Sources
The authors declare no funding supports.
References
- Sanchis-Gomar, F., Perez-Quilis, C., Leischik, R., Lucia, A. (2016). Epidemiology of coronary heart disease and acute coronary syndrome. Ann Transl Med. 4(13):256.
CrossRef - Prabhakaran, D., et al. (2016). Cardiovascular Diseases in India: Current Epidemiology and Future Directions. Circulation 133(16):1605-20.
CrossRef - Rissam, H.S., et al. (2001). Coronary Artery Disease in Young Indians – The Missing Link. Indian Acad Clin Med. 2(3): 128–131.
- Benjamin, E.J., et al. (2017) Heart Disease and Stroke Statistics—2017 Update. A Report From the American Heart Association. Circulation 135(10): e146–e603.
CrossRef - DeFronzo, R.A., (2006). Insulin Resistance, Hyperinsulinemia, and Coronary Artery Disease: A Complex Metabolic Web. J Cardiovasc Pharmacol. 20 Suppl 11, S1-16.
CrossRef - von Eckardstein, A., Assmann, G., (1997). Plasma homocysteine levels and mortality in patients with coronary artery disease. N Engl J Med. 337:1632–1633.
CrossRef - Ballantyne, C.M., et al. (2001). Influence of low high-density lipoprotein cholesterol and elevated triglyceride on coronary heart disease events and response to simvastatin therapy in 4S. Circulation 104:3046–3051.
CrossRef - Rubins, HB., (2000). Triglycerides and coronary heart disease: implications of recent clinical trials. J Cardiovasc Risk. 7:339–345.
CrossRef - Tzoulaki, I., et al. (2019). Serum metabolic signatures of coronary and carotid atherosclerosis and subsequent cardiovascular disease. Eur Heart J. 40(34): 2883–2896.
CrossRef - Yang, S., et al. (2019). Gut Microbiota-Dependent Marker TMAO in Promoting Cardiovascular Disease: Inflammation Mechanism, Clinical Prognostic, and Potential as a Therapeutic Target. Front Pharmacol. 10: 1360.
CrossRef - Janeiro, MH., (2018). The implication of Trimethylamine-N-Oxide (TMAO) in Disease: Potential Biomarker or New Therapeutic Target. Nutrients 10(10):1398.
CrossRef - Koeth, R.A., et al. (2013). Intestinal microbiota metabolism of L-carnitine, a nutrient in red meat, promotes atherosclerosis. Nat Med. 19 (5):576–585.
CrossRef - Chen, K., et al. (2017). Gut Microbiota-Dependent Metabolite Trimethylamine-N-Oxide Contributes to Cardiac Dysfunction in Western Diet-Induced Obese Mice. Front Physiol. 8:139–147.
CrossRef - Chhibber-Goel, J., Singhal, V., Gaur, A. et al. (2018). Structure-Function Analysis of Liver Flavin Monooxygenase 3 that Drives Trimethylaminuria in Humans. Proc Natl Acad Sci India Sect B Biol Sci. 88, 1681–1690.
CrossRef - Hai, X., Landeras, V., Dobre, MA., DeOreo, P., Meyer, TW., Hostetter, TH. (2015). Mechanism of Prominent Trimethylamine Oxide (TMAO) Accumulation in Hemodialysis Patients. PLoS One 10(12): e0143731.
CrossRef - Fennema, D., Phillips, IR., Shephard, EA. (2016). Trimethylamine and Trimethylamine-N-Oxide, a Flavin-Containing Monooxygenase 3 (FMO3)-Mediated Host-Microbiome Metabolic Axis Implicated in Health and Disease [published correction appears in Drug Metab Dispos. 44(12 ):1949]. Drug Metab Dispos. 44(11):1839-1850.
CrossRef - Akerman, BR., Lemass, H., Chow, LM., et al. (1999). Trimethylaminuria is caused by mutations of the FMO3 gene in a North American cohort. Mol Genet Metab. 68:24–31.
CrossRef - Cashman, JR., Bi YA., Lin, J. et al. (1997). Human flavin-containing monooxygenase form 3: cDNA expression of the enzymes containing amino acid substitutions observed in individuals with trimethylaminuria. Chem Res Toxicol. 10:873–41.
CrossRef - Treacy, EP., Akerman, BR., Chow, LM., et al. (1998). Mutations of the flavin-containing monooxygenase gene (FMO3) cause trimethylaminuria, a defect in detoxication. Hum Mol Genet. 7:839–45.
CrossRef - Mitchell, SC., (2005). Trimethylaminuria (fish-odor syndrome) and oral malodor. Oral Dis. 11 Suppl 1:10-13.
CrossRef - Trimethylaminuria In: Chen H. (eds) Atlas of Genetic Diagnosis and Counseling. Springer, New York, NY, 2012.
- Wang, Z., Klipfell, E., Bennett, BJ., et al. (2011). Gut flora metabolism of phosphatidylcholine promotes cardiovascular disease. Nature 472:57-63.
CrossRef - Andreesen, JR. (1994). Glycine metabolism in anaerobes. Antonie Van Leeuwenhoek 66, 223–237.
CrossRef - Zhang, AQ., Mitchell, SC., Smith, RL. (1999). Dietary precursors of trimethylamine in man: a pilot study. Food Chem Toxicol. 37: 515–520.
CrossRef - Mafune, A., Iwamoto, T., Tsutsumi, Y., Nakashima, A., Yamamoto, I., Yokoyama, K., et al. (2016). Associations among serum trimethylamine‐N‐oxide (TMAO) levels, kidney function and infarcted coronary artery number in patients undergoing cardiovascular surgery: a cross‐sectional study. Clin Exp Nephrol. 20(5): 731–739.
CrossRef - Ayesh, R., Mitchell, SC., Zhang, A., Smith, RL. (1993). The fish odor syndrome: biochemical, familial, and clinical aspects. BMJ 307: 655–657.
CrossRef - Smith, JL., Wishnok, JS., Deen, WM. (1994). Metabolism and excretion of methylamines in rats. Toxicol Appl Pharmacol. 125: 296–308.
CrossRef - Schmidt, AC., Leroux, J-C. (2020). Treatments of trimethylaminuria: where we are and where we might be heading. Drug Discovery Today 25(9):1710-1717.
CrossRef - Lusis, AJ. (2000). Atherosclerosis. Nature 407(6801):233-241.
CrossRef - Trøseid, M., Ueland, T., Hov, JR., Svardal, A., Gregersen, I., Dahl, CP., Aakhus, S., Gude, E., Bjørndal, B., Halvorsen, B. et al. (2015). Microbiota-dependent metabolite trimethylamine-N-oxide is associated with disease severity and survival of patients with chronic heart failure. J Intern Med. 277:717–726.
CrossRef - Mente, A., Chalcraft, K., Ak H., Davis, A.D., Lonn, E., Miller, R., Potter, M.A., Yusuf, S., Anand, S.S., McQueen, M.J. The Relationship Between Trimethylamine-N-Oxide and Prevalent Cardiovascular Disease in a Multiethnic Population Living in Canada. Can J Cardiol. 2015;31:1189–1194.
CrossRef - Wang Z., Tang W.H., Buffa J.A., Fu X., Britt E.B., Koeth R.A., Levison B.S., Fan Y., Wu Y., Hazen S.L. (2014). The prognostic value of choline and betaine depends on intestinal microbiota-generated metabolite trimethylamine-N-oxide. Eur Heart J. 35:904–910.
CrossRef - Tang W., Wang Z., Levison BS., Koeth RA., Britt EB., Fu X. et al. Intestinal Microbial Metabolism of Phosphatidylcholine and Cardiovascular Risk. N Engl J Med. 2013; 368:1575-1584.
CrossRef - Dong Z, Liang Z, Guo M, Hu S, Shen Z, Hai X. The Association between Plasma Levels of Trimethylamine-N-Oxide and the Risk of Coronary Heart Disease in Chinese Patients with or without Type 2 Diabetes Mellitus. Dis Markers 2018;2018:1578320.
CrossRef - Roncal, C., Martínez-Aguilar, E., Orbe, J., et al. (2019). Trimethylamine-N-Oxide (TMAO) Predicts Cardiovascular Mortality in Peripheral Artery Disease. Sci Rep. 9.
CrossRef - Yao, M., Liao, P., Zhao, X., et al. (2020). Trimethylamine-N-oxide has prognostic value in coronary heart disease: a meta-analysis and dose-response analysis. BMC Cardiovasc Disord. 20.
CrossRef - Tang, W.H.W., Wang, Z., Kennedy, D.J., Wu, Y., Buffa, J.A., Agatisa-Boyle, B., Li, X.S., Levison, B.S., and Hazen, S.L. (2015). The gut microbiota-dependent trimethylamine-N-oxide (TMAO) pathway contributes to both developments of renal insufficiency and mortality risk in chronic kidney disease. Circ Res. 116(3): 448–455.
CrossRef - Bae, S., Ulrich, C.M., Neuhouser, M.L., Malysheva, O., Bailey, L.B., Xiao, L., Brown, E.C., Cushing-Haugen, K.L., Zheng, Y., Cheng, T.Y.D., Miller, J.W., Green, R., Lane, D.S., Beresford, S.A.A., Caudill, M.A. (2014). Plasma choline metabolites and colorectal cancer risk in the Women’s Health Initiative Observational Study. Cancer Res. 74(24): 7442–7452.
CrossRef - Senthong, V., Li, XS., Hudec, T., et al. (2016). Plasma Trimethylamine-N-Oxide, a Gut Microbe-Generated Phosphatidylcholine Metabolite, Is Associated With Atherosclerotic Burden. J Am Coll Cardiol. 67(22):2620-2628.
CrossRef - Li, XS., Obeid, S, Klingenberg, R., Gencer, B., Mach, F., Räber, L., Windecker, S., Rodondi, N., Nanchen, D., Muller, O., Miranda, M.X., Matter, C.M., Wu, Y., Li, L., Wang, Z., Alamri, H.S., Gogonea, V., Chung, Y.M., Tang, W.H., Hazen, S.L., Lüscher, T.F. (2017). Gut microbiota-dependent trimethylamine-N-oxide in acute coronary syndromes: a prognostic marker for incident cardiovascular events beyond traditional risk factors. 38:814–824.
CrossRef - Tan, Y., Sheng, Z., Zhou, P., et al. (2019). Plasma Trimethylamine-N-Oxide as a Novel Biomarker for Plaque Rupture in Patients With ST-Segment-Elevation Myocardial Infarction. Circ Cardiovasc Interv. 12(1):e007281.
CrossRef - Yu, D., Shu, X.O., Rivera, E.S., et al. (2019). Urinary Levels of Trimethylamine-N-Oxide and Incident Coronary Heart Disease: A Prospective Investigation Among Urban Chinese Adults. J Am Heart Assoc. 8(1):e010606.
CrossRef - Zeisel S.H., Warrier, M. (2017). Trimethylamine-N-Oxide, the Microbiome, and Heart and Kidney Disease. Annu Rev Nutr. 37:157–181.
CrossRef - Nie, J., Xie, L., Zhao, B-x., Li, Y., Qiu, B., Zhu, F., et al. (2018). Serum Trimethylamine-N-Oxide Concentration Is Positively Associated With First Stroke in Hypertensive Patients. Stroke 49:2021–2028.
CrossRef - Croyal, M., Saulnier, P.J., Aguesse, A., et al. (2020) Plasma trimethylamine-N-oxide and risk of cardiovascular events in patients with type 2 diabetes. J Clin Endocrinol Metab. 105(7):dgaa188.
CrossRef - Haissman, JM., Haugaard, A.K., Ostrowski, S.R., et al. (2017). Microbiota-dependent metabolite and cardiovascular disease marker trimethylamine-N-oxide (TMAO) is associated with monocyte activation but not platelet function in untreated HIV infection. BMC Infect Dis. 17(1):445.
CrossRef - Wang, Z., Bergeron, N., Levison, B.S., et al. (2019). Impact of chronic dietary red meat, white meat, or non-meat protein on trimethylamine-N-oxide metabolism and renal excretion in healthy men and women. Eur Heart J. 40(7):583-594.
CrossRef - Senthong, V., Wang, Z., Fan, Y., Wu, Y., Hazen, S.L., Tang, W.H. (2016). Trimethylamine-N-oxide and mortality risk in patients with peripheral artery disease. J Am Heart Assoc. 2016;5(10):e004237.
CrossRef - Montrucchio, C., De Nicolò, A., D’Ettorre, G., et al. (2020). Serum Trimethylamine-N-oxide Concentrations in People Living with HIV and the Effect of Probiotic Supplementation. Int J Antimicrob Agents 55(4):105908.
CrossRef - daCosta, K.A., Vrbanac, J.J., Zeisel, S.H. (1990). The measurement of dimethylamine, trimethylamine, and trimethylamine-N-oxide using capillary gas chromatography-mass spectrometry. Anal Biochem. 187:234–239.
CrossRef - Beale, R., Airs, R. (2016). Quantification of glycine betaine, choline and trimethylamine-N-oxide in seawater particulates: Minimisation of seawater associated ion suppression. Anal Chim Acta. 938:114–122.
CrossRef - Barrea, L., Annunziata, G., Muscogiuri, G., et al. (2018). Trimethylamine-N-oxide (TMAO) is a novel potential biomarker of early predictors of metabolic syndrome. Nutrients 10(12):1971.
CrossRef - Yu, W., Xu, C., Li, G., Hong, W., Zhou, Z., Xiao, C., Zhao, Y., Cai, Y., Huang, M., Jin, J. (2018). Simultaneous determination of trimethylamine-N-oxide, choline, betaine by UPLC-MS/MS in human plasma: An application in acute stroke patients. J Pharm Biomed Anal. 152:179–187.
CrossRef - Jia, X., Osborn, L.J., Wang, Z. (2020). Simultaneous Measurement of Urinary Trimethylamine (TMA) and Trimethylamine-N-Oxide (TMAO) by Liquid Chromatography-Mass Spectrometry. Molecules 25(8), 1862.
CrossRef - Tang, W.H., Wang, Z., Li, X.S., et al. (2017). Increased Trimethylamine-N-Oxide Portends High Mortality Risk Independent of Glycemic Control in Patients with Type 2 Diabetes Mellitus. Clin Chem. 63(1):297-306.
CrossRef - Al-Obaide, M.A.I., Singh, R., Datta, P., et al. (2017). Gut Microbiota-Dependent Trimethylamine-N-oxide and Serum Biomarkers in Patients with T2DM and Advanced CKD. J Clin Med. 6(9):86.
CrossRef - Gao, X., Tian, Y., Randell, E., Zhou, H., Sun, G. (2019). Unfavorable Associations Between Serum Trimethylamine-N-Oxide and L-Carnitine Levels With Components of Metabolic Syndrome in the Newfoundland Population. Front Endocrinol (Lausanne). 10:168.
CrossRef - Haghikia, A., Li, X.S., Liman, T.G., Bledau, N., Schmidt, D., Zimmermann, F. (2018). Gut Microbiota-Dependent Trimethylamine-N-Oxide Predicts Risk of Cardiovascular Events in Patients With Stroke and Is Related to Proinflammatory Monocytes. Arterioscler Thromb Vasc Biol. 38 (9), 2225–2235.
CrossRef - Li, T., Chen, Y., Gua, C., and Li, X. (2017). Elevated Circulating Trimethylamine-N-Oxide Levels Contribute to Endothelial Dysfunction in Aged Rats through Vascular Inflammation and Oxidative Stress. Front Physiol. 8, 350.
CrossRef - Wang, S., Xia, G.H., He, Y., Liao, S. X., Yin, J., Sheng, H.F. (2016). Distribution characteristics of trimethylamine-N-oxide and its association with gut microbiota. Nan Fang Yi Ke Da Xue Xue Bao 36 (4), 455–460.
- Shan, Z., Clish, C.B., Hua, S., Scott, J.M., Hanna, D.B., and Burk, R.D. (2018). Gut microbial-related choline metabolite trimethylamine-N-Oxide is associated with the progression of carotid artery atherosclerosis in HIV infection. J Infect Dis. 218 (9), 1474–1479.
CrossRef
Accepted on: 12 Aug 2021
Second Review by: Sanjin Kovacevic Serbia and Sherif Afifi Egypt





Web of Science Coverage
Emerging Sources Citation Index (ESCI)
2024 Journal Impact Factor: 1.1
Scopus Journal Metrics
CiteScore 2025: 2.6
CiteScore Details
Sustainable Nutrition: Food Systems, Nutrient Retention, and Public Health Impact
![]()
This journal is a member of, and subscribes to the principles of, the Committee on Publication Ethics (COPE)








