Impact of Dietary Magnesium on Oral Health Status Among Adults in Arar and Riyadh, Saudi Arabia: A Cross-Sectional Analysis
 and Amer Alenezi
and Amer Alenezi Community Health Department, Northern Border University, Arar, Saudi Arabia.
Corresponding Author Email: nalqahtaniphd@gmail.com
DOI : http://dx.doi.org/10.12944/CRNFSJ.14.1.18
Download this article as:
![]()
Magnesium is important for bone metabolism, immune regulation and integrity of the enamel and dentin. Worldwide, there is evidence of a significant association between higher magnesium intake and the low risk for caries or periodontitis; however, there is not enough data from regional studies in the Middle East (and specifically Saudi Arabia). The objectives of in the present study were to evaluate the relationship of dietary magnesium intake with oral health index, dental caries and periodontitis among adults residing in Arar and Riyadh cities, and also test whether this association was modified by BMI. A cross-sectional study was carried out among 401 adults (aged 18–45 years) selected by stratified sampling from Arar (rural) and Riyadh (urban). Dietary magnesium was determined from a validated semi-quantitative food frequency questionnaire. Oral health status was assessed in terms of Decayed, Missing and Filled Teeth (DMFT) index and Community Periodontal Index (CPI). Anthropometric data were used to determine BMI. Chi-square tests, correlations and multiple regression were used in the analyses. The mean magnesium intake was 281.8 ± 56.9 mg/day, which was lower than the recommended dietary allowances. Among subjects with higher magnesium intake, there was a significant decrease in DMFT (0.99 ± 1.14 vs 2.32 ± 1.56) and CPITN scores (0.60 ± 0.49 vs 2.55 ± 0.50; p < 0.001). There was an inverse correlation between magnesium intake and DMFT (r = –0.277) and CPITN (r = –0.808). Magnesium intake was an independent predictor of oral health determined by multiple regression analysis, whereas BMI did not modify the associations significantly. An interactive exploration of the analysis is available at: https://cnpdata.shinyapps.io/magnesium_project/. Higher consumption of dietary magnesium is linked with better oral health marked by a decrease in caries and periodontal disease. These results underscored the necessity for nutrition centered approaches in oral health care in Saudi Arabia.
KEYWORDS:Body Mass Index (BMI); Magnesium Intake; Nutrition; Oral Health; Saudi Adults
Introduction
Oral health is an essential aspect of human wellbeing, impacting on both day-to-day function and systemic health.1,2 At the global level, more than 3.5 billion people are affected by oral diseases, which are the most common non-communicable diseases.1 Dental caries and periodontitis are major causes of tooth loss, discomfort and diminished quality of life as well as having associations with certain systemic conditions including cardiovascular illness, diabetes and neurodegenerative diseases.1,2 Poor oral health places a socioeconomic burden in terms of decreased productivity and loss of opportunities and higher treatment costs.3,4
There is a two-way connection with nutrition and oral health. Fermentable carbohydrates in the diet increase risk of caries and exposure to fruits, vegetables, whole grains, and minerals is protective.5,6 Of the vital nutrients, magnesium has been identified as a key player in enamel competence, bone mass and inflammatory balance.7 Magnesium is a part of more than 300 enzymatic reactions and is stored in bone (60%), where it has a role in bone mineralization as maintaining skeletal strength.8–10 Inadequacy increases oxidative stress and inflammation,11,12 modulates immune responses,13,14 and disrupts the enamel and dentin architecture.15 Observational researches have consistently observed an association between low magnesium intake and high severity of periodontitis, susceptibility to caries, whereas supplementation ameliorates periodontal status.16,17
Despite a global evidence showing an inverse correlation between magnesium consumption and oral health, very little data are available in Middle Eastern populations. One cross- sectional survey in Saudi Arabia’s Eastern Province demonstrated a high prevalence of low dietary magnesium intake amongst adult participants,18 and a study in Qassim determined that serum magnesium levels were significantly lower among people suffering from high caries history,19 emphasizing the importance of locally relevant research within this area.
The objective of this study is to explore the association between magnesium consumption from diet, and oral health (dental caries and periodontitis) in Adults residing in Riyadh and Arar. The results will provide locally applicable evidence to inform preventive oral health strategies and nutrition focused interventions.
Materials and Methods
Study Design and Setting
We used a cross-sectional analytical study design to investigate the association between dietary magnesium (Mg) intake and oral health outcomes in Saudi adults. The data was collected in two different geographically and demographically cities: Riyadh (Urban) and Arar (rural). These areas were chosen to ensure variability in diet, healthcare accessibility and environmental exposures that could be expected to affect oral health and magnesium balance.
Study Population
Eligible participants were 18–45 years adults, with more than one year of living in the study setting. Participants also had to be able to give consent.19 Exclusion criteria excluded pregnant and lactating women; patients with systemic diseases associated with oral health, mineral metabolism that could compromise the control of treatment (e.g., chronic kidney disease, uncontrolled diabetes); intake of magnesium supplements or drugs that prevent absorption or modify the balance of magnesium and treated by a dentist in the last 6 months. Sample Size Estimation
Sample size was calculated by formula for estimations of a single proportion (N = (Z²pq)/d²). Taking the most conservative estimate, the population proportion (p=0.5,q=0.5), we could thus be most variable assuming it fifty percent of uncertainty and that the confidence level was 95%(Z = 1.96) with a margin of error equal to 5% (d = 0.05). A total of at least 385 respondents were therefore needed. Considering the 10% dropout/ non-response, the total sample was about at least 422 participants.
Sampling Technique
A stratified sample size was used to have representation from both urban and rural areas in Saudi Arabia. The study sample was stratified into two strata, Riyadh (urban area) and Arar (rural area). This categorization was rationalized on the basis of variations in dietary habits, lifestyle variables and availability of an applied oral health care system in both regions. In each level participants were chosen by way of random sampling based on availability in healthcare facilities, community centres and at workplaces. For the cases where random sampling was not feasible especially in hard to reach rural areas with constrained sampling frame, convenience sampling method was used. This Mixed-method strategy resulted in sufficient participant recruitment with regard to socio-demographic diversity.
Data Collection Tools and Procedures
Socio-demographic and lifestyle characteristics (age, sex, education, income and smoking) were obtained using a standard questionnaire. Dietary magnesium consumption was evaluated with a semi-quantitative Food Frequency Questionnaire (FFQ), which incorporated magnesium from local food sources, such as green leafy vegetables, nuts and whole grains. Consumption frequency and portion size in the past month were self-reported by the participants. Daily intakes were estimated using standard food composition tables and classified as low (< 250 mg/day), medium (250–319 mg/day) or high (≥ 320 mg/ day), according to Recommended Dietary Allowances.4,8 The FFQ was based on questionnaires which were validated in Middle Eastern populations and compared with local food composition tables. Its content validity and cultural relevance were reviewed by experts, and was piloted for clarity and feasibility. Standardized portion aids were used to improve accuracy, aligning with best practices for dietary assessment tools.3,18
Oral Health Assessment
Patients were examined orally, using the criteria of the World Health Organization (WHO). Two indices were employed:
DMFT: Decayed, Missing, Filled Teeth which was used as an index to the number of instances of dental caries.
These include:
Periodontal Status as assessed by CPITN.20
Calibration was done for all examiners in order to maintain inter-ratter reliability.
Ethical Considerations
Ethical clearance was taken from local committee of Northern Border University, Saudi Arabia (Code No.: HAP-09-34). Written informed consent was obtained from all subjects. Confidentiality was assured and participation was completely voluntary with the option to withdraw at any time.
Dietary Assessment
Dietary magnesium intake was measured by a validated semi-quantitative Food Frequency Questionnaire (FFQ) based on that designed by21 and adapted for use in regional populations.22 The FFQ was used to assess typical intake of magnesium-containing foods over the past three months.
Anthropometric Measurements
Height and weight were measured using standard protocol of anthropometric measurements. The body mass index (BMI) was defined as the weight in kilograms divided by the square of the height in meters (kg/m²). They were then classified using World Health Organization criteria as normal weight (18.5–24.9 kg/m²), overweight (25.0–29.9 kg/m²) or obese (≥30.0 kg/m²). (World Health Organization, 2000).
Statistical Analysis
Data was collected with Microsoft Excel and analyzed with SPSS (version 25). Means and proportions were used to summarize social demographic variables, BMI, magnesium intake and oral health indicators (DMFT &CPITN). For normally distributed data, the mean and SD were reported, and for non-normally distributed data, we report median and range. Relationships among discrete variables were assessed with chi-square. Differences in non-normally distributed variables between categories of magnesium intake were tested using the Kruskal-Wallis test. The Pearson correlation coefficients were employed to determine the linear correlations between continuous magnesium intake and oral health scorings.
Independent predictors of DMFT scores and CPITN were established by multiple linear regression models. We conducted a receiver operator characteristic (ROC) curve analysis to test the discriminative performance of dietary magnesium intake concerning poor oral health indices (i.e. increasing DMFT and CPITN scores). Youden-index method was used to calculate the cut-off points of magnesium intake, which would maximize the sum of sensitivity and specificity. Results: p < 0.05 was considered as statistical significance.
Results
An interactive version of the analysis conducted can be accessed from here: https://cnpdata.shinyapps.io/magnesium_project/
Participant Characteristics and Response Rate
A total of 401 of the 422 respondents finished the study and contributed usable data for analysis (response rate: 95%). The study recruited 401 patients (mean age 31.8 ± 8.6 years, men: 57.1%). The mean BMI was 24.5 ± 5.9 kg/m², and the average magnesium intake was 281.8±56.9mg/day. ThemeanDMFTwas2. 1±1.5, while the median CPITN was 1.6 (range 1–3) (Table 1).
Table 1: Socio-demographic and clinical characteristics.
|
Variable |
Value (mean ± SD) / n (%) |
|
Age (years) |
31.78 ± 8.62 |
|
Sex |
|
|
Male |
229 (57.1) |
| Female |
172 (42.9) |
|
Education level |
|
| Master’s |
15.2 |
|
Bachelor’s |
21.2 |
| Higher secondary |
18.7 |
|
Secondary |
11.0 |
| Primary |
21.4 |
|
No formal education |
12.5 |
| BMI (kg/m²) |
24.51 ± 5.90 |
|
Magnesium intake (mg/day) |
281.76 ± 56.87 |
| DMFT score |
2.11 ± 1.50 |
|
CPITN (median, range) |
1.63 (1–3) |
|
Smoking status |
|
|
Yes |
25.9 |
| No |
74.1 |
Association of Magnesium Intake with Socio-Demographic and Clinical Factors
A significant association was seen with age (p = 0.001), BMI category (p = 0.007) and education level (p < 0.001), but not with sex (0.16). Overweight participants and those with higher education were more likely to have high magnesium intake (Table 2).
Table 2: Association between magnesium intake and socio-clinical variables.
|
Variable |
Category | Low n (%) | Moderate n (%) | High n (%) | p-value |
| Sex | Male | 56 (13.97) | 113 (28.18) | 60 (14.96) |
0.16 |
|
Female |
59 (14.71) | 86 (21.45) |
27 (6.73) |
||
|
Age (years) |
18–25 | 54 (13.47) | 49 (12.22) | 26 (6.48) | 0.001* |
| 26–35 | 22 (5.49) | 64 (15.96) |
20 (4.99) |
||
|
≥35 |
39 (9.73) | 86 (21.45) |
41 (10.22) |
||
|
BMI category |
Underweight | 8 (1.99) | 24 (5.99) | 11 (2.74) | 0.007* |
| Normal | 73 (18.20) | 84 (20.95) |
39 (9.73) |
||
| Overweight | 34 (8.48) | 91 (22.69) | 37 (9.23) | ||
| Education |
No formal |
17 (4.24) | 27 (6.73) | 6 (1.50) | 0.000* |
| Primary | 27 (6.73) | 36 (8.98) |
23 (5.74) |
||
|
Secondary |
17 (4.24) | 10 (2.49) | 17 (4.24) | ||
| Diploma | 13 (3.24) | 38 (9.48) |
24 (5.99) |
||
|
Bachelor’s |
28 (6.98) | 45 (11.22) |
12 (2.99) |
Association between Magnesium Intake and Oral Health Scores
Mean DMFT and CPITN scores were found significantly lower with more magnesium intake, suggesting better dental and periodontal health. Participants in the high intake group had significantly lower mean DMFT (0.99 ± 1.14) and CPITN (0.60 ± 0.49) scores than their low (DMFT: 2.32 ± 1.56; CPITN: 2.55 ± 0.50) and moderate counterparts (DMFT: 2.48 ± 1.48, P <.00001). CPITN: 1.55 ± 0.49) (Table 3; Figure 1).
Table 3: Oral Health Scores by Magnesium Intake Category.
|
Magnesium Intake Category |
Mean DMFT ± SD | p-value (DMFT) | Mean CPITN ± SD |
p-value (CPITN) |
|
Low |
2.32±1.56 | 2.55±0.50 | ||
| Moderate | 2.48±1.48 | 0.000* | 1.55±0.49 |
0.000* |
|
High |
0.99±1.14 |
0.60±0.49 |
Note: Magnesium intake categories—Low (< 250 mg/day), Moderate (250–319 mg/day), High (≥ 320 mg/day); DMFT = Decayed, Missing, and Filled Teeth; CPITN = Community Periodontal Index.
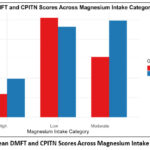 |
Figure 1: Mean DMFT and CPITN Scores Across Magnesium Intake Categories. |
Correlation of Magnesium Intake with DMFT and CPITN Scores
Pearson analysis showed significant negative relationship between magnesium intake with DMFT (r = –0.277) and CPITN score (r = –0.808, p < 0.001), suggesting that increased magnesium intake was negatively correlated with better dental health and periodontal status (Table 4). These results were confirmed by the scatter plots demonstrating a negative correlation between magnesium intake and oral health scores (Figure 2).
Table 4: Correlation between magnesium intake and oral health scores.
|
Variable |
r-value |
p-value |
|
Magnesium vs. DMFT |
-0.277 |
0.000* |
|
Magnesium vs. CPITN |
-0.808 |
0.000* |
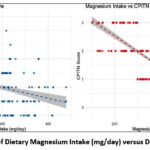 |
Figure 2: Scatterplots of Dietary Magnesium Intake (mg/day) versus DMFT and CPITN Scores. |
Independent Predictors of Oral Health Outcomes: Multiple Linear Regression Analysis
Independent predictors of oral health outcomes were identified by multiple linear regression analyses, controlling for age, BMI, and sex. Two models for DMFT and CPITN scores were statistically negatively associated with magnesium intake (β = –0.662 p < 0.001 and β = –1.009 p < 0.001 respectively). The adjustment explained 14.5% of the variation in DMFT (R² = 0.145) and 67.1% of CPITN (R² = 0.671), showing a good relationship with periodontal condition. Age and BMI were not related to, but male gender predicted the significantly lower CPITN scores (β = – 0.285, p < 0.001) with Table 5).
Table 5: Multiple linear regressions for DMFT and CPITN.
|
Outcome Measure |
Predictor (Independent Variable) | β (Unstandardized) | β (Standardized) | 95% CI | t-value |
p-value |
|
DMFT |
Magnesium intake |
−0.662 | −0.310 | −0.875 to −0.449 | 6.25 |
<0.001 |
|
Age |
0.014 | 0.095 | −0.003 to 0.031 | 1.62 |
0.105 |
|
|
BMI |
0.015 | 0.071 | −0.011 to 0.040 | 1.14 | 0.255 | |
| Sex (1 = Male) | −0.221 | −0.085 | −0.525 to 0.082 | 1.43 |
0.152 |
|
|
CPITN |
Magnesium intake |
−1.009 | −0.785 | −1.078 to −0.941 | 32.1 | <0.001 |
| Age | −0.001 | −0.010 | −0.007 to 0.004 | 0.40 |
0.692 |
|
|
BMI |
0.005 | 0.056 | −0.003 to 0.013 | 1.18 | 0.236 | |
| Sex (1 = Male) | −0.285 | −0.265 | −0.383 to −0.188 | 5.8 |
<0.001 |
Diagnostic Accuracy of Magnesium Intake for Predicting Oral Health Status
CPITN’s optimal cut-off level of 293 mg/day combined improved sensitivity (88.84%), specificity (76.84%) and excellent discrimination (AUC: 89.73%). For DMFT, the cut-off of 318 mg/day had a high sensitivity (91.16%) and lower specificity, where as an a moderate discriminating accuracy was observed (AUC = 66.35%) (Table 6; Figure 3).
Table 6: Diagnostic accuracy of magnesium intake cut-off values for predicting poor oral health outcomes.
|
Variable |
Cut-off point | Sensitivity | Specificity |
Area under the curve |
|
CPITN |
293 | 88.84% | 76.84% |
89.73% |
|
DMFT |
318 | 91.16% | 42.76% |
66.35% |
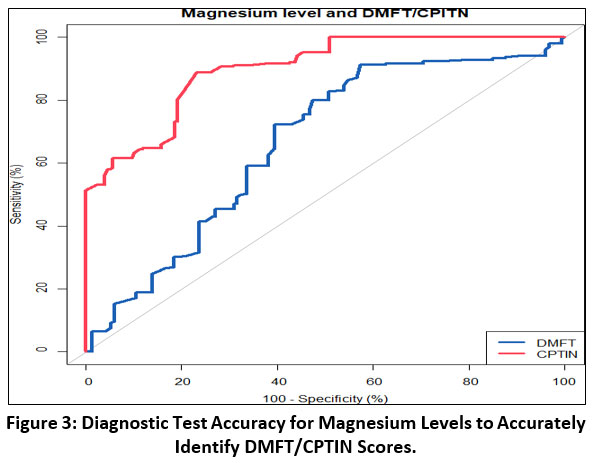 |
Figure 3: Diagnostic Test Accuracy for Magnesium Levels to Accurately Identify DMFT/CPTIN Scores. |
Discussion
This study aimed to the relationship dietary magnesium and oral health among adults in Arar and Riyadh. Results The mean dietary magnesium intake in the subjects (281.76 ± 56.87 mg/day) was less than the RDA for both men (400–420 mg/day) and women (310–320mg/day).6 (National Institutes of Health [NIH], 2022). Magnesium intake was an independent factor associated with oral health status.
Another observation was that low magnesium intake was associated with significantly higher DMFT and CPITN scores suggesting a poorer oral health status compared to those which high magnesium intakes. Correlation investigations further supported these relationships, showing highly negative associations of magnesium consumption with the DMFT and CPITN scores (indicating protection against dental caries and periodontal disease). In addition, regression analyses supported these conclusions.
The results complement evidence from the Middle East. A report from Bahrain had shown a statistically significant reduction in the serum magnesium levels of high-DMFT individuals and suggested its protective effect against dental caries.12 In a similar study recently conducted in the Eastern Region of Saudi Arabia, an interesting finding was that the majority of adults ingested insufficient amounts of dietary magnesium–a characteristic linked with poor eating habits and high intake of refined carbohydrates.1 Complementary to our finding of an association between higher Mg intake and lower CPITN scores, Li and co-authors described a 31 % less odds of periodontitis.
Among adult in the highest as compared to those in the lowest quintile of magnesium intake categories (OR = 0.69, 95% CI: 0.52–0.92).23
Forcing the mechanistic link between low magnesium status and periodontal breakdown, experimental data bring biological plausibility: when they were severely deprived, rats displayed reduced bone mineral density as well as enhanced inflammatory bone resorption.7 By showing these relationships among adults from Arar and Riyadh, the present study expands on the previous observations, which has largely focused on Western and East Asian cohorts and make them applicable to a Middle Eastern setting.
Magnesium is an essential regulator of bone metabolism and approximately 60% of the body’s magnesium stores are found in the skeleton. Deficiency has been shown to cause loss of bone mass, decrease in bone metabolism and deterioration in the alveolar support for teeth, with a higher risk for the development of both caries and periodontal disease.19,23 At the oral cavity hard tissue level, low magnesium has been related to enamel hypoplasia, dentin becomes more friable, and teeth can be lost early.24,25 Magnesium also acts as a major factor in controlling inflammatory mediators.2,14,20 It regulates the secretion of cytokines and oxidative stress leading to influencing periodontal inflammation as well as tissue damage. Low Mg levels have been linked to inflammation, and increased inflammatory response might accelerate progression of periodontitis.19,24 Thus, we speculate that magnesium might reduce caries and periodontal disease by promoting the hardening of teeth as well as bone, and also inhibiting inflammation, providing a biological basis for the lower DMFT and CPITN scores.
This study has a number of strengths that increase confidence in its results. First, sample size was relatively large (>400 subjects), and therefore results had enough statistical power to observe significant relationships between magnesium intake contribution from diet and oral health endpoints. We used validated data collection tools, including the semi-quantitative FFQ for dietary evaluation, DMFT index for dental caries and CPI index for periodontal status to guarantee methodological rigor. In addition, the incorporation of anthropometric measurements, particularly BMI, allowed stratified analyses and consideration of potential effect modification providing a more detailed exploration.
Limitations
There are several limitations to the present study that should be taken into account when interpreting the findings. There were a couple of limitations in this study. First, we are unable to establish the casual relationship between magnesium concentration and PIGD phenotype due to its cross-sectional design.
Intake and oral health outcomes. Although associations were detected, there could have been yet reverse causality or unmeasured confounding. Second, dietary magnesium intake was estimated by an FFQ and although the questionnaire had been validated for use in our study, it is known to be influenced by recall bias and estimates may not have been precise. Third, serum magnesium concentrations were not determined and as a result, dietary intake may not entirely represent true magnesium status or bioavailability.
Fourth, individuals were limited to those aged 18–45 years in the study, and therefore these results may not be generalizable to older participants who could have different dietary behaviours or other systemic diseases and absorption or metabolism of nutrients. Therefore, caution is needed when generalizing these findings to an elderly population and studies in older subjects are required to elucidate age differences with respect to magnesium status and oral health. Finally, despite controlling for the main demographic and clinical characteristics, residual confounding due to socioeconomic or behavioural causes as well as other dietary factors cannot be excluded. These limitations can be tackled by future work based on a longitudinal cohort and controlled interventional design to disentangle the temporal and causality link between magnesium intake and oral health. The addition of a biochemical measure (that is, magnesium in serum, saliva or urine) would increase the accuracy of the assessment as well as decrease subjectivity and reliance on dietary self-reporting. Extensions of this work would include follow-up evaluations in the same study population with comparisons made over time to enhance their internal validity. Intervention or supplementation dietary trials may also advance whether enhancing intake of magnesium brings about demonstrable changes in the rates of caries and periodontal diseases. In addition, studies designed for Saudi and other Middle Eastern populations are warranted due to regional diets, water mineralization differences, and different environmental minerals exposure that may uniquely affect magnesium status and oral health in this region.24
Conclusion
Overall, maintaining optimal magnesium consumption is an easily applicable, cost-effective and long-lasting strategy in promoting oral health. Emphasizing nutrition-oriented interventions in addition to conventional oral health preventive strategies, such as restorative and preventive treatment programs for dental caries, public health plans in Saudi Arabia can prevent the burden of oral diseases including dental caries and periodontal diseases while promoting general health.
Acknowledgement
The author would like to express my sincere gratitude to the dietitians who generously contributed their expertise and support throughout the course of this research. Their guidance and assistance were invaluable in shaping the outcomes of this work. In particular, I am deeply thankful to: Dana Sultan, Rinad Farhan, Arkan, Jude Alkhinani, Lama Anwar and Rimas Nawi. Their dedication and contributions have enriched this study, and I am truly grateful for their time and effort. We would like to thank Dr. Abhishek Gupta and his team for their support in manuscript editing and proofreading. The authors extend their appreciation to the Deanship of Scientific Research at Northern Border University, Arar, KSA for funding this research work through the project number “NBU-FFR-2026-2975-5
Funding Sources
The authors received no financial support for the research, authorship, or publication of this article
Conflict of Interest
The authors do not have any conflict of interest.
Data Availability Statement
This statement does not apply to this article
Ethics Statement
This research did not involve human participants, animal subjects, or any material that requires ethical approval
Informed Consent Statement
This study did not involve human participants, and therefore, informed consent was not required.
Clinical Trial Registration
This research does not involve any clinical trials
Permission to Reproduce Material from Other Sources
Not Applicable
Author Contributions
- Nasser Salem Alqahtani: Conceptualization, Study design, Data collection supervision, Statistical analysis, Interpretation of results, and Manuscript drafting.
- Amer Alenezi: Literature review, Data curation, Methodology validation, Visualization, and Critical revision of the manuscript for intellectual content.
References
- Abualrahi AM, Alhanabi FH, Alalloush RS, et al. Assessment of dietary magnesium intake in the Eastern Province of Saudi Arabia. J Med Life. 2023;16(12):1789-1795. doi:10.25122/jml-2023-0279
CrossRef - Ashique S, Kumar S, Hussain A, et al. A narrative review on the role of magnesium in immune regulation, inflammation, infectious diseases, and cancer. J Health Popul Nutr. 2023;42(1):74. doi:10.1186/s41043-023-00423-0
CrossRef - Belluci MM, de Molon RS, Rossa C, et al. Severe magnesium deficiency compromises systemic bone mineral density and aggravates inflammatory bone resorption. J Nutr Biochem. 2020;77:108301. doi:10.1016/j.jnutbio.2019.108301
CrossRef - Cade JE, Burley VJ, Warm DL, et al. Food-frequency questionnaires: a review of their design, validation and utilisation. Nutr Res Rev. 2004;17(1):5-22. doi:10.1079/NRR200370
CrossRef - Chan AKY, Tsang YC, Jiang CM, et al. Diet, Nutrition, and Oral Health in Older Adults: A Review of the Literature. Dent J (Basel). 2023;11(9):222. doi:10.3390/dj11090222
CrossRef - Cui Q, Xia Y, Wu Q, et al. Validity of the food frequency questionnaire for adults in nutritional epidemiological studies: A systematic review and meta-analysis. Crit Rev Food Sci Nutr. 2023;63(12):1670-1688. doi:10.1080/10408398.2021.1966737
CrossRef - Eghtesad S, Hekmatdoost A, Faramarzi E, et al. Validity and reproducibility of a food frequency questionnaire assessing food group intake in the PERSIAN Cohort Study. Front Nutr. 2023;10:1059870. doi:10.3389/fnut.2023.1059870
CrossRef - El Kinany K, Garcia-Larsen V, Khalis M, et al. Adaptation and validation of a food frequency questionnaire (FFQ) to assess dietary intake in Moroccan adults. Nutr J. 2018;17(1):61. doi:10.1186/s12937-018-0368-4
CrossRef - Fiorillo L. Oral Health: The First Step to Well-Being. Medicina (Kaunas). 2019;55(10):676. doi:10.3390/medicina55100676
CrossRef - Gondivkar SM, Gadbail AR, Gondivkar RS, et al. Nutrition and oral health. Dis Mon. 2019;65(6):147-154. doi:10.1016/j.disamonth.2018.09.009
CrossRef - Li XY, Wen MZ, Liu H, et al. Dietary magnesium intake is protective in patients with periodontitis. Front Nutr. 2022;9:976518. doi:10.3389/fnut.2022.976518
CrossRef - Jawed M, Abdulmonem WA, Alkhamiss A, et al. Role of Serum Magnesium in Dental Caries. Bahrain Medical Bulletin. 2021;43(1).
- Liu L, Luo P, Wen P, et al. The role of magnesium in the pathogenesis of osteoporosis. Front Endocrinol (Lausanne). 2024;15:1406248. doi:10.3389/fendo.2024.1406248
CrossRef - Maier JA, Castiglioni S, Locatelli L, et al . Magnesium and inflammation: Advances and perspectives. Semin Cell Dev Biol. 2021;115:37-44. doi:10.1016/j.semcdb.2020.11.002
CrossRef - Malik R, Tangade P, Kalantharakath T, et al. Nutrition & Oral Health. TMU Journal of Dentistry. 2022;9. doi:10.58358/tmujd.09031
CrossRef - Mazur A, Maier JAM, Rock E, et al. Magnesium and the inflammatory response: potential physiopathological implications. Arch Biochem Biophys. 2007;458(1):48-56. doi:10.1016/j.abb.2006.03.031
CrossRef - Nielsen FH. Magnesium deficiency and increased inflammation: current perspectives. J Inflamm Res. 2018;11:25-34. doi:10.2147/JIR.S136742
CrossRef - Petersen PE, Baez RJ, Organization WH. Oral Health Surveys: Basic Methods. World Health Organization; 2013. Accessed September 3, 2025. https://iris.who.int/handle/10665/97035
- Rondanelli M, Faliva MA, Tartara A, et al. An update on magnesium and bone health. Biometals. 2021;34(4):715-736. doi:10.1007/s10534-021-00305-0
CrossRef - Shahi A, Aslani S, Ataollahi M, et al. The role of magnesium in different inflammatory diseases. Inflammopharmacology. 2019;27(4):649-661. doi:10.1007/s10787-019-00603-7
CrossRef - Willett WC, Sampson L, Stampfer MJ, et al. Reproducibility and validity of a semiquantitative food frequency questionnaire. Am J Epidemiol. 1985;122(1):51-65. doi:10.1093/oxfordjournals.aje.a114086
CrossRef - Sukumar D, DeLuccia R, Cheung M, et al. Validation of a Newly Developed Food Frequency Questionnaire to Assess Dietary Intakes of Magnesium. Nutrients. 2019;11(11):2789. doi:10.3390/nu11112789
CrossRef - Li X, Xue Q, Ma H, et al. Genetically determined gut microbial abundance and 2-year changes in central adiposity and body composition: the POUNDS lost trial. Clinical nutrition (Edinburgh, Scotland). 2022;41(12):2817‐2824. doi:10.1016/j.clnu.2022.11.002
CrossRef - Uwitonze AM, Rahman S, Ojeh N, et al. Oral manifestations of magnesium and vitamin D inadequacy. J Steroid Biochem Mol Biol. 2020;200:105636. doi:10.1016/j.jsbmb.2020.105636
CrossRef - Sahin E, Orhan C, Balci TA, et al. Magnesium Picolinate Improves Bone Formation by Regulation of RANK/RANKL/OPG and BMP-2/Runx2 Signaling Pathways in High-Fat Fed Rats. Nutrients. 2021;13(10):3353. doi:10.3390/nu13103353
CrossRef
Accepted on: 31 Mar 2026
Second Review by: Vijay Shukla
Final Approval by: Dr. Rajesh Jeewon





Web of Science Coverage
Emerging Sources Citation Index (ESCI)
2024 Journal Impact Factor: 1.1
Scopus Journal Metrics
CiteScore 2025: 2.6
CiteScore Details
Sustainable Nutrition: Food Systems, Nutrient Retention, and Public Health Impact
![]()
This journal is a member of, and subscribes to the principles of, the Committee on Publication Ethics (COPE)








