Knowledge, Attitude and Practices of Breastfeeding Among Mothers of Children Under 6 Months of Age in Suva, Fiji
Maca D. Temoirokomalani1
and Sabiha Khan3 1Department of Dietetics and Nutrition, Ministry of Health and Medical Services, Fiji.
2Department of Primary Care and Nutrition, School of Public Health and Primary Care, College of Medicine, Nursing and Health Science, Fiji National University, Fiji.
3Department of Epidemiology and Environmental Health, School of Public Health and Primary Care, College of Medicine, Nursing and Health Science, Fiji National University, Fiji.
Corresponding Author Email: pragya.singh@fnu.ac.fj
DOI : http://dx.doi.org/10.12944/CRNFSJ.9.3.27
Download this article as:
![]()
Breastfeeding is a cost-effective public health approach that decreases infant and child morbidity and mortality. Fiji's exclusive breastfeeding rate was 40 percent compared to the global target of 50 percent. The research aims to evaluate mothers’ breastfeeding infants' level of knowledge, attitudes, and practice less than 6 months of age in Suva. A descriptive quantitative cross-sectional study was carried out in 3 randomly selected medical areas in Suva, Fiji. Knowledge, attitude, and practice (KAP) questionnaire was used to gather data from 415 mothers. The overall mean scores for breastfeeding knowledge of mothers were 12.9, the attitude was 33.7, and practice 7.20. Results showed that mothers were generally found to have good levels of knowledge and practice but a fair attitude. Knowledge was associated with the number of children that mothers had and ethnicity. Attitude had a positive correlation with household income. The practice was positively correlated with the mother's status of employment, the number of children, ethnicity, marital status, and household income. To improve breastfeeding knowledge, attitude and practices of mothers, awareness and education should be strengthened in all health facilities. Improvement in health education materials and advocacy is required.
KEYWORDS:Attitude; Breastfeeding; Knowledge; Mothers; Practice
Introduction
Breastfeeding is the foundation of life and is recognized as the best way of feeding infants 1. Breast milk provides the basic building block for optimal growth and development and contains the right amount of nutrients for growth that is easily digested and is readily available. It is the most cost-effective public health strategy to decrease infant and child morbidity and mortality. Given the recognized benefits of breastfeeding for the health of the mother and infants, WHO advocates exclusive breastfeeding for the first half-year after birth followed by sustained breastfeeding with suitable complementary foods after 6 months with ongoing breastfeeding up to 2 years or beyond2.
Breastfeeding has the ability to increase a child’s tolerance to all preventive therapies and is estimated to save 1.4 million lives in developingcountries3. Breastfed babies have a six-fold higher chance of survival in the first six months than non-breastfed babies. Acute respiratory infection and diarrhea, two big infant killers, as well as other infectious diseases, are reduced by breast milk4. The potential impact of appropriate breastfeeding practices is particularly important in developing countries with high disease burdens and limited access to clean water and sanitation. Non-breastfed infants in developing countries are even more likely to die. In a recent study of post-neonatal mortality in the United States, it was discovered that mortality among non-breastfed infants increased by 25%. According to the Millennium Cohort Survey in the United Kingdom (UK), six months of exclusive breastfeeding was linked to a 53 percent reduction in diarrhea hospital admissions and a 27 percent reduction in respiratory tract infections5.
Breastfeeding also has substantial economic benefits. The Economic Review and analysis of the benefits of breastfeeding by the Department of Agriculture (United States) conclude that a minimum of $3.6 billion can be saved if breastfeeding improved from 64 percent to 75 percent in hospitals and 29 percent to 50 percent at six months as recommended by their US Surgeon General. These are the savings from direct expenses such as formula costs and physician, clinic, hospital, laboratory, and procedural fees and indirect expenses such as time and wages lost by caretakers attending to an ill child6.
Apart from the emotional satisfaction that mothers receive through breastfeeding, studies have demonstrated that women that had breastfeeding experience had reduced proportions of breast and ovarian cancer future in their lives7. Maternal health benefits also increase as breastfeeding duration increases and the risk of developing type 2 diabetes, rheumatoid arthritis, and cardiovascular disease, including high blood pressure and high cholesterol levels are also reduced. Mothers need support to improve breastfeeding practices and duration, and these are the targets that most health facilities aim to achieve.
Strong evidence from both developed and developing countries have shown the benefits of breastfeeding for infants, babies, and mothers and despite this positive impact, the rate of Exclusive Breastfeeding (EBF) continues to drop in both developed and developing countries8. Approximately 38 percent of children under the age of six months in developed countries are exclusively breastfed, and only 39 percent of 20-23-month-olds profit from the practice of continued breastfeeding.
Fiji’s overall exclusive breastfeeding rate was below the global target despite an increase in rates from 2004 to 2015. The National Nutrition Survey (NNS) showed that 49 percent of children were exclusively breastfed in 2015 compared to 39.8 percent in 2004. Similarly, the infant mortality rate (IMR) and under-five mortality rate (U5 MR) showed a similar trend from 1990 to 2015 with improved rates of IMR from 25/1,000 live births to 13.8/1,000 live births and U5MR, from 30/1,000 live births to 18/1,000 live births; however, both targets; IMR of 5.5/1,000 live births and U5MR of 7/1,000 was not achieved. Researches have shown evidence on the relationship between exclusive breastfeeding; malnutrition and U5MR and IMR in low- middle-income countries and Fiji is no exception.
Understanding the breastfeeding knowledge, attitude, and practice (KAP) of mothers and factors influencing their breastfeeding practices is important. Many studies were conducted worldwide and this is the first KAP study to be conducted in the Central Division of Fiji. This study will provide information on mothers’ breastfeeding KAP and determine the factors influencing their practice. Also, the results of this study will be communicated to the Ministry of Health and other relevant stakeholders for future planning and decision-making for improved activities and programs, and it will also serve as a basis for future research.
Methodology
This descriptive cross-sectional study was performed in the Central Division, from May to August 2019. Suva, Samabula and Raiwaqa Medical Areas in the Suva subdivision were randomly selected for data collection out of seven medical areas in the Suva subdivision.
Sampling
All mothers of infants under six months of age attending the maternal and child health clinics in the medical area of the study were considered during the study period. All breastfeeding mothers of infants under 6 months of age that were registered in the study medical areas and consented to participate were included in the study. All eligible mothers who visited MCH clinics in the three medical areas were contacted by the researcher and information regarding the study was given to them. Those who agreed to participate were given the consent form and asked to sign the consent form. The research excluded non-registered, non-consenting, and mothers of infants older than 6 months.
Sampling Procedure and Sample Size
The sample size was determined by applying the 40% prevalence of exclusive breastfeeding with 5% margin error; 95% confidence interval and 10% non-respondent rate. The sample size required was 410. The sample size distribution was based on the total population and was proportionally selected as 80 mothers from Suva, 77 mothers from Samabula and 253 mothers from Raiwaqa. The total population per medical area was 12,075 for Suva, 17,413 for Samabula and 32,349 for Raiwaqa. 372 out of 415 registered mothers gave consent to take part in this research. Participants for Suva, Samabula and Raiwaqa were 90, 85 and 240 respectively, and the overall response rate was 89.6 %.
Data Collection
Data collection was done using a self-administered questionnaire that was adopted from similar studies to collect information. The questionnaire consisted of 47 questions and had four sections. The first section was the socio-demographic characteristics of the mother and baby; the second section was on knowledge with 15 knowledge-related questions on BF with optional answers ‘True’, ‘False’ or ‘Don’t know’ where True was the correct answer and was recorded as 1; False was the incorrect answer and was recorded as 0. The minimum score was 0 and the maximum score was 15. Correct answers were quantified and were assessed as 0 – 4 as Poor knowledge; 5 – 10 as Fair knowledge; and 11 – 15 as Good knowledge.
The third section was on attitude towards breastfeeding with 10 attitude related questions about BF and answers were based on a Likert Scale of 5 to 1 with 5 as Strongly Disagree, 4 as Disagree, 3 as Neutral, 2 as Agree and 1 as Strongly Agree were used to assess the attitude of mothers. The maximum score assessed was 50 while the minimum score was 10 and quantification of the Attitude was assessed as: < 22 as Poor Attitude; 23– 35 as Fair Attitude; and > 35 as Good Attitude. The fourth section was on the practice with 9 related questions for mothers towards BF. The answer was optional ‘Yes’, ‘No’ or ‘Don’t know’ whereby Yes was the correct answer and was recorded as 1 and No was the incorrect answer and was recorded as 0. Correct answers were quantified and assessed as: 0 – 2 as Poor Practice; 3 – 5 as Fair Practice; and 6 – 8 as Good Practice. The total score for the three sections; (2, 3 &4) was divided into tertiles, with the lowest tertiles assigned to the worst evaluation and the highest to the best evaluation 9.
The questionnaire was validated by 10 experts in the relevant fields and was pretested on 30 population samples. These samples were from other medical areas and were not part of the study, so were excluded after pretesting. The questionnaire was also translated into I-Taukei Hindi for FID participants. Before beginning data collection, the College Health Research Ethics Committee (CHREC) and the Fiji National Health Research and Ethics Review Committee (FNHREC No. 2018.180.C.D) gave their approval for this study. Consented mothers meeting the inclusion criteria were contacted and given information sheets by medical area nurses. Confidentiality was maintained through the process of this study by giving numbers to the mothers and not their names.
Statistical Analysis
All statistical analysis was done using SPSS Version 25 for all data collected. All continuous data were presented using mean and standard deviation and categorical data were presented in numbers and percentages. Kolmogrov- Smirnov test was used to test the data distribution. The bivariate test was used to assess the difference between the dependent variable (KAPs) and independent variables (socio-demographic characteristics) were tested using ANOVA and Kruskal Wallis test. The Spearman correlation coefficient test was used to identify the association between knowledge and attitude, knowledge and practice, and attitude and practice. The significance level for all statistical analyses was set at 0.05.
Results
Socio-Demographic Characteristics of Mothers and Infants
Tables 1 and 2 show the socio-demographic characteristics of the mothers and infants in the sample, respectively.372 mothers participated in this study with 75% (n=279) I- Taukei. The age range of mothers was between 16 – 51 years old with a mean age of 27.87± 6.1 years. More than half; 60.2% (n=2224) of the mothers were from Raiwaqa Medical Area.
Most infants (78.2 %) were delivered normally and only 21.8% were delivered through cesarean section. The socio-demographic characteristics of the mothers are shown below.
Table 1: Socio-demographic Characteristics of Mothers.
| Socio-demographic Characteristics | Frequency (n= 372) | Percentage (%) |
| Medical Area | ||
| Suva | 80 | 21.5 |
| Samabula | 68 | 18.3 |
| Raiwaqa | 224 | 60.2 |
| Age group | ||
| <18 years | 2 | 0.5 |
| 19-45 years | 367 | 98.7 |
| >45 years | 3 | 0.8 |
| Ethnicity | ||
| I-Taukei | 279 | 75.0 |
| Fijian of Indian descent (FID) | 34 | 9.1 |
| Fijian of other descent (FOD) | 59 | 15.9 |
| Marital Status | ||
| Married | 298 | 80.1 |
| Unmarried Single | 61 | 16.4 |
| Defector | 13 | 3.5 |
| Education Level | ||
| Primary | 3 | 0.8 |
| Secondary | 145 | 39.0 |
| Tertiary | 224 | 60.2 |
| No. of Children | ||
| First | 133 | 35.8 |
| Second | 105 | 28.2 |
| > 3 infants | 134 | 36.0 |
| Employment | ||
| Self Employed | 16 | 4.3 |
| Domestic Duties | 236 | 63.4 |
| Government Worker | 37 | 9.9 |
| Private Employee | 60 | 16.1 |
| Student | 23 | 6.2 |
| Household Income | ||
| <$10,000 | 147 | 39.5 |
| $10,000 – $30,000 | 129 | 34.7 |
| >$30,000 | 33 | 8.9 |
| Don’t know | 63 | 16.9 |
Table 2: Socio-Demographic Characteristics of Infants.
| Socio-demographic characteristics | Frequency (n= 372) | Percentage (%) |
| Age of Infants | ||
| 0-1 month | 175 | 47.0 |
| 1-3 months | 123 | 33.1 |
| 3-6 months | 74 | 19.9 |
| Gestational Age at birth | ||
| Less than 37 weeks | 238 | 64.0 |
| 37-42 weeks | 124 | 33.3 |
| More than 42 weeks | 10 | 2.7 |
| Infant’s Birth weight | ||
| Less than 2.5 Kg | 31 | 8.3 |
| 2.5-4.0 Kg | 294 | 79.0 |
| More than 4.0 Kg | 47 | 12.6 |
| Type of delivery | ||
| Normal Vaginal | 291 | 78.2 |
| Caesarean Section | 81 | 21.8 |
Mothers Breastfeeding Knowledge
The breastfeeding knowledge of mothers in this study is represented in Table 3. Response options 2 & 3 will be combined when reporting if n is less than or equal to 30.
The majority (99.5%) of the mothers knew that breast milk is the first food for the baby. 84.9% of the mothers knew that breastfeeding decreases the diarrhea episodes in children and 84.1 % knew that the colostrum in the breast milk works as a safe vaccine for the baby. 76.6% of the mothers knew that breastfeeding prevents breast cancer and 78.8% believed that breastfeeding is a good family planning method.10.8% (n=40) of mothers responded that breastfeeding should continue once solid foods are introduced, however, 87.9% (n=327) agreed that it should stop.
Table 3: Mothers Breastfeeding Knowledge.
| Knowledge Statements | Responses** | Frequency (n=372) | Percentage | |
| Breast milk has all the nutrients that the baby needs | T | 368 | 98.9 | |
| F | 2 | 0.5 | ||
| DK | 2 | 0.5 | ||
| Colostrum in breast milk works as a safe vaccine for baby | T | 313 | 84.1 | |
| F | 16 | 4.3 | ||
| DK | 43 | 11.6 | ||
| Breast milk is easier to absorb and digest than baby formula | T | 364 | 97.8 | |
| F | 5 | 1.3 | ||
| DK | 3 | 0.8 | ||
| Breastfeeding can be continued for up to 2 years | T | 343 | 92.2 | |
| F | 16 | 4.3 | ||
| DK | 13 | 3.5 | ||
| Breast milk alone is needed for the first six months of life | T | 324 | 87.1 | |
| F | 36 | 9.7 | ||
| DK | 12 | 3.2 | ||
| Breastfeeding mothers should take healthy food to improve breast milk supply and secretion | T | 368 | 98.9 | |
| F | 1 | 0.3 | ||
| DK | 3 | 0.8 | ||
| Baby should be breastfed 2 hourly * | T | 31 | 8.3 | |
| F | 334 | 89.8 | ||
| DK | 7 | 1.9 | ||
| Breastfeeding helps bonding of mother and child | T | 367 | 98.7 | |
| F | 4 | 1.1 | ||
| DK | 1 | 0.3 | ||
| Breastfeeding decreases diarrhea | T | 316 | 84.9 | |
| F | 21 | 5.6 | ||
| DK | 35 | 9.4 | ||
| Breast milk is cheap compared to formula milk | T | 369 | 99.2 | |
| F | 2 | 0.5 | ||
| DK | 1 | 0.3 | ||
| Breastfeeding prevents the mother from breast cancer | T | 285 | 76.6 | |
| F | 14 | 3.8 | ||
| DK | 73 | 19.6 | ||
| The first food for the baby is breast milk | T | 370 | 99.5 | |
| F | 2 | 0.5 | ||
| DK | 0 | 0 | ||
| Breastfeeding is a good family planning method | T | 293 | 78.8 | |
| F | 25 | 6.7 | ||
| DK | 54 | 14.5 | ||
| Once solid foods are introduced, breastfeeding should be stopped* | T | 327 | 87.9 | |
| F | 40 | 10.8 | ||
| DK | 5 | 1.3 | ||
| Health professionals encourage breastfeeding | T | 367 | 98.7 | |
| F | 2 | 0.5 | ||
| DK | 3 | 0.8 | ||
* Statements with a reverse score
** Responses are coded as T indicates True, F indicates False and DK indicates Don’t Know
Mother’s Breastfeeding Attitude
Participants’ attitude towards breastfeeding in this study is presented in Table 4. The majority (58.6 %) of mothers agreed that formula feeding is the best choice if mothers plan to go back to work while only 26.9% (n=100) either disagree or strongly disagree with the statement. More than half (65.4%) either agreed or strongly agreed that bottle feeding is the best choice if a baby refused to suckle on the breast. About 16.4% of mothers found it difficult to breastfeed their infants on demand. More than half (54.7%) agreed that breastfeeding takes a lot of time while 17% of the mothers stated that they had difficulty in breastfeeding infants till six months of age. 10.5% of mothers responded that that formula is just as healthy as breast milk and 23.6% of mothers agree that breastfeeding is an old fashion.
Table 4: Mother’s breastfeeding Attitude.
| Attitude Statements (n=372) | Likert Scale Classification * | |||||||||
| SD = 5 | D =4 | N=3 | A=2 | SA=1 | ||||||
| n | % | n | % | n | % | N | % | n | % | |
| Formula feeding is the best choice if mothers plan to go back to work | 10 | 2.7 | 90 | 24.2 | 54 | 14.5 | 203 | 54.6 | 15 | 4.0 |
| Bottle feeding is the option if the baby refuses to suckle on the breast | 8 | 2.2 | 84 | 22.6 | 37 | 9.9 | 226 | 60.8 | 17 | 4.6 |
| Women should not breastfeed in public places (such as restaurants, markets, etc.) | 176 | 47.3 | 147 | 39.5 | 17 | 4.6 | 26 | 7.0 | 6 | 1.6 |
| I find it difficult to breastfeed my baby on demand | 46 | 12.4 | 242 | 65.1 | 23 | 6.2 | 57 | 15.3 | 4 | 1.1 |
| The benefits of breastfeeding last only for a shorter time | 65 | 17.5 | 239 | 64.2 | 21 | 5.6 | 46 | 12.4 | 1 | 0.3 |
| Breastfeeding takes a lot of time | 27 | 7.3 | 147 | 39.5 | 32 | 8.6 | 149 | 40.1 | 17 | 14.6 |
| I find it difficult to exclusively breastfeed my baby till 6 months | 36 | 9.7 | 250 | 67.2 | 23 | 6.2 | 55 | 14.8 | 8 | 2.2 |
| The formula is just as healthy as breast milk | 67 | 18.0 | 239 | 64.2 | 27 | 7.3 | 32 | 8.6 | 7 | 1.9 |
| A maternity leave of 2 months is enough to successfully breastfeed** | 3 | 0.8 | 57 | 15.3 | 22 | 5.9 | 219 | 58.9 | 71 | 19.1 |
| Breastfeeding is old fashion | 141 | 37.9 | 131 | 35.2 | 12 | 3.2 | 83 | 22.3 | 5 | 1.3 |
*SD refers to Strongly Disagree, D refers to Disagree, N refers to neither agree nor disagree, A refers to agree and SA refers to strongly agree
**Statements with a reverse score
Mothers Breastfeeding Practice
The mother’s breastfeeding practice is presented in Table 5. The majority (97.6%) of the mothers responded to infants receiving breast milk as good practice as the first feed. The majority (92.5%) of infants were fed with other foods apart from breast milk before six months of age. 97% of the infant were introduced to solid foods at four months of age. 90.1% of mothers gave colostrum to their infants. Initiation of breastfeeding within an hour of birth was practiced by 86.8% of mothers in this study whereas. 13.9% of infants were no longer breastfed during the period of study. More than two-thirds of infants, 69.6% (n= 259) were given other milk at home apart from breast milk, while only 29% continued with breastfeeding.
Table 5: Mothers Breastfeeding Practice.
| Practice Questions | Options** | Frequency (n) | Percentage |
| Colostrum was given to my baby | Y | 335 | 90.1 |
| N | 34 | 9.1 | |
| DK | 3 | 3 | |
| Breastfeeding initiation was done within an hour of birth | Y | 323 | 86.8 |
| N | 47 | 12.6 | |
| DK | 2 | 0.5 | |
| The first feeding given to the baby was breast milk | Y | 363 | 97.6 |
| N | 9 | 2.4 | |
| DK | 0 | 0 | |
| From birth till discharge, the baby was fed with breast milk | Y | 354 | 95.2 |
| N | 13 | 3.5 | |
| DK | 5 | 1.3 | |
| The baby was given other milk apart from breast milk at home | Y | 259 | 69.6 |
| N | 108 | 29.0 | |
| DK | 5 | 1.3 | |
| The baby was given other foods apart from breast milk | Y | 344 | 92.5 |
| N | 25 | 6.7 | |
| DK | 3 | 0.8 | |
| The baby was introduced with solid food at 4 months | Y | 361 | 97.0 |
| N | 11 | 3.0 | |
| DK | 0 | 0 | |
| Are you still breastfeeding your child | Y | 320 | 86.0 |
| N | 31 | 8.3 | |
| DK | 21 | 5.6 |
** Responses are coded as Y indicates Yes, N indicates No and DK indicates Don’t know
Reasons for not Breastfeeding
The reasons given by mothers for not breastfeeding are presented in Fig 1. The majority of the mothers 29.8% stated “others” (include family factors eg mother in law not permitting the daughter in law to breastfeed as she wants her to do household work or husband not permitting his wife to breastfeed or mother does not want to breastfeed as it hinders her to complete her household work) as the reason for stopping breastfeeding. About one-quarter of those who had stopped breastfeeding, 25.5 % gave poor lactation as the reason. About 23.4% gave “returned to work” as their reason and 8.5% made a personal choice to change other types of milk feed. About 8.5% of participants stopped breastfeeding because the baby was sick or irritable and crying. 2.1 % of the mothers stopped breastfeeding because of some family problems or were sick.
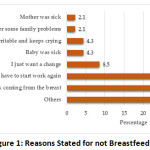 |
Figure 1: Reasons Stated for not Breastfeeding. |
Levels of Knowledge, Attitude, and Practice (KAP)
Table 6 presents the response distribution in relation to the levels of knowledge, attitude, and practice of mothers towards breastfeeding in this study. 94.1% of mothers showed good levels of knowledge and 5.9% had either poor or moderate levels of breastfeeding knowledge. The majority; 65.9% of mothers showed fair attitudes towards breastfeeding; 34.1% had a good attitude and only 0.3% had a poor attitude towards breastfeeding. 89% of mothers showed good breastfeeding practice; 10.5% had fair breastfeeding practice and only 0.5% had poor breastfeeding practice.
Table 6: Distribution of KAP.
| Knowledge | Attitude | Practice | ||||||
| Levels | (n=372) | (%) | Levels | (n= 372) | % | Levels | (n= 372) | % |
| Poor(< 4) | 1 | 0.3 | Poor(< 22) | 1 | 0.3 | Poor(< 2) | 2 | 0.5 |
| Fair(5-10) | 21 | 5.6 | Fair(23 -35) | 244 | 65.9 | Fair(3-5) | 39 | 10.5 |
| Good(11-15) | 350 | 94.1 | Good( > 35) | 127 | 34.1 | Good(> 6) | 331 | 89 |
KAP Overall Mean Scores
The level of mothers’ knowledge, attitude, and practice scores towards breastfeeding is presented in Table 7.The mean knowledge score was 12.9 ± 1.5 which showed good levels of breastfeeding knowledge amongst the study population. The mean attitude score was 33.7 ± 4.2 which demonstrates that mothers participating in this study had fair attitudes towards breastfeeding and the mean practice score of 7.2 ± 1.2 showed good breastfeeding practices.
Table 7: KAP Overall Mean Scores.
| KAP | Mean | SD |
| Knowledge | 12.9 | ± 1.5 |
| Attitude | 33.7 | ± 4.2 |
| Practice | 7.2 | ± 1.2 |
Correlation between Knowledge, Attitude and Practice
The correlation between knowledge and attitudes, knowledge and practice, and attitude and practices of mothers concerning breastfeeding is presented in Table 8. The correlation between knowledge and attitude), knowledge and practice, and attitudes and practice were all significant, but a weak positive correlation existed. For knowledge and attitude, the correlation demonstrated that when knowledge increases, attitude also increases (r=0.234; p=0.001). Similarly, when knowledge increases, the practice also increases, and the same is the pattern with attitude and practice.
Table 8: Correlation between KAP.
| Variable | r | p-value |
| Knowledge vs. Attitude | 0.234 | 0.001* |
| Knowledge vs. Practice | 0.162 | 0.002* |
| Attitude vs. Practice | 0.191 | 0.001* |
* Spearmen correlation coefficient
Correlation between Socio-Demographic Characteristics and KAP
Bivariate analysis between socio-demographic characteristics and KAP is presented in Table 9. In this study; the mothers breastfeeding knowledge has a highly significant association with the number of children (p=0.006) and ethnicity (p=0.021). Mothers belonging to the I-tukeli ethnicity had significantly higher knowledge scores as compared to the mothers of FID and FOD. Mothers having two children had a higher knowledge score compared to others. No significant relationship was found between mothers’ breastfeeding knowledge and their age, marital status, education level, mother’s employment and household annual income.
For breastfeeding attitude, the study showed that household annual income is significantly associated with the mother breastfeeding attitude (p=0.004) and the number of children that mothers have (p=0.029). Mothers with annual household income between $10 thousand to $30 thousand had significantly higher mean attitude scores as compared to mothers belonging to other annual household income groups. Mothers with two children had a significantly good breastfeeding attitude with a mean score of 34.6 ± 3.71 compared to others. No significant association was found between mother attitudes towards breastfeeding and mother age, mother’s ethnicity, marital status, mother education level, and mother’s employment.
For breastfeeding practice of mothers, the number of children, employment status, level of household income, marital status, and ethnicity showed a highly significant relationship with mean practice scores. In this study, the I-taukei mothers had significantly higher breastfeeding practice scores compared to FID and FOD mothers. Mothers with more than one child had significantly higher breastfeeding practice scores as compared to others. Mothers who stayed at home with no form of employment had good breastfeeding practice compared to those that were employed. For household income, mothers with annual household income between $10 thousand to $30 thousand had significantly higher mean breastfeeding practices as compared to other groups. For marital status, mothers with a defector relationship had significantly higher breastfeeding practice scores compared to those who were either married or were single. No significant association was found between mothers breastfeeding practice with their age and education level.
Table 9: Correlation between Socio-Demographic Characteristics and KAP.
| Socio-demographic | Knowledge | Attitude | Practice | ||||||
| Characteristics | Mean | SD | P-Value | Mean | SD | P-Value | Mean | SD | P-Value |
| Medical Area | |||||||||
| Suva | 12.8 | ± 1.45 | 0.366* | 33.8 | ± 4.52 | 0.483 | 7.2 | ± 1.27 | 0.508* |
| Samabula | 12.9 | ± 1.85 | 33.2 | ± 4.49 | 7.3 | ± 1.21 | |||
| Raiwaqa | 12.9 | ± 1.31 | 33.9 | ± 3.90 | 7.1 | ± 1.21 | |||
| Age | |||||||||
| <18 years | 12 | ± 1.41 | 0.410* | 37 | ± 1.41 | 0.368* | 6.5 | ± 2.12 | 0.862* |
| 19-45 years | 12.9 | ± 1.45 | 33.7 | ± 4.16 | 7.2 | ± 1.21 | |||
| >45 years | 13.3 | ± 1.16 | 34 | ± 3.46 | 6.7 | ± 2.3 | |||
| Ethnicity | |||||||||
| I-Taukei | 12.99 | ± 1.51 | 0.021* | 33.8 | ± 4.04 | 0.645 | 7.2 | ± 1.16 | 0.041* |
| FID | 12.74 | ± 1.14 | 33.7 | ± 4.96 | 6.8 | ± 1.54 | |||
| FOD | 12.68 | ± 1.31 | 33.3 | ± 4.21 | 6.9 | ± 1.27 | |||
| Marital Status | |||||||||
| Married | 12.9 | ± 1.45 | 0.556* | 33.7 | ± 4.14 | 0.435* | 7.2 | ± 1.23 | 0.031* |
| Unmarried Single | 12.8 | ± 1.50 | 34 | ± 4.19 | 6.9 | ± 1.23 | |||
| Defector | 13.2 | ± 1.21 | 32.9 | ± 4.26 | 7.4 | ± 0.87 | |||
| Education Level | |||||||||
| Primary | 12.0 | ± 1.0 | 0.154* | 37.3 | ± 1.16 | 0.151* | 5.7 | ± 2.08 | 0.328* |
| Secondary | 12.8 | ± 1.68 | 33.6 | ± 4.17 | 7.2 | ± 1.04 | |||
| Tertiary | 13.0 | ± 1.27 | 33.8 | ± 4.15 | 7.1 | ± 1.31 | |||
| No. of Children | |||||||||
| One child | 12.6 | ± 1.76 | 0.006* | 33.1 | ± 4.52 | 0.029 | 6.9 | ± 1.31 | 0.005* |
| two children | 13.2 | ± 1.20 | 34.6 | ± 3.71 | 7.2 | ±1.23 | |||
| 3 and above children | 13.1 | ± 1.22 | 33.7 | ± 4.02 | 7.3 | ±1.09 | |||
| Employment | |||||||||
| Self Employed | 13.06 | ±1.12 | 0.748* | 32.9 | ± 4.83 | 0.893 | 7.0 | ± 1.46 | 0.007* |
| Domestic Duties | 12.86 | ±1.53 | 33.7 | ± 4.14 | 7.3 | ± 1.11 | |||
| Government Work | 13.14 | ±1.32 | 34.1 | ± 4.43 | 6.7 | ± 1.49 | |||
| Private Employee | 12.97 | ±1.33 | 33.9 | ± 4.23 | 6.9 | ±1.29 | |||
| Student | 12.87 | ±1.33 | 33.6 | ± 3.23 | 6.9 | ± 1.25 | |||
| Household Income | |||||||||
| <$10,000 | 12.86 | ± 1.33 | 0.284 | 33.4 | ± 3.53 | 0.004 | 7.2 | ±1.09 | 0.030* |
| $10,000 – $30,000 | 13.04 | ± 1.57 | 34.8 | ± 4.42 | 7.4 | ± 1.19 | |||
| >$30,000 | 13.12 | ± 1.19 | 32.7 | ± 4.07 | 6.5 | ±1.77 | |||
| Don’t know | 12.68 | ± 1.56 | 32.9 | ± 4.59 | 7.2 | ± 1.11 | |||
* Kruskal Wallis test
Discussion
The level of practice of breastfeeding in this study was generally high with a rate of 86%; however, the national exclusive breastfeeding rate was 40% in Fiji. This result was higher than the study conducted in Calabar, Nigeria, which was 80%10; 11, and 43.6% 12 and Abha city, Saudi Arabia, which was 8.3% 13. However, all of these studies showed lower breastfeeding rates than this study that was conducted in Suva, Fiji.
Knowledge of Mothers Towards Breastfeeding
The majority (90%) of the participating mothers responded correctly to the following breastfeeding knowledge related statements that include; breast milk is the first food for baby; it has all the nutrients that the baby needs; it is easier to absorb and digest than baby formula; it is cheap compared to formula milk; breastfeeding helps to the bond of mother and child; mothers who breastfeed should have good nutrition to improve breast milk supply and secretion; health professional encouraged breastfeeding and breastfeeding can be continued up to two years.
Although the overall breastfeeding knowledge of mothers was good, there were some notable gaps found in this study and this was related to the continuity of breastfeeding after complementary feeding was introduced after six months. 87.9% of mothers responded that breastfeeding should stop once solid food was introduced. A correct knowledge response of 10.8% signified both poor or inadequate knowledge and the World Health Organization recommended that breastfeeding continue until the infant reached 2 years of age. More awareness and education on infant and young child feeding practices with an emphasis on continuing breastfeeding after complementary could help encourage mothers to continue breastfeeding after six months.
Knowledge gaps were also found on the statements related to the maternal benefits of breastfeeding that it prevents the mother from breast cancer and a good family planning method. About 12.9% of mothers lacked the knowledge that breast milk alone is needed for the first six months of life. Education with emphasis on the maternal benefits of breastfeeding and exclusive breastfeeding for the first six months of life could also help encourage mothers to breastfeed their infants at antenatal clinic visits and MCH clinics. Awareness about the maternal health benefits of breastfeeding is important for all adolescents’ health services, especially for female adolescents.
The knowledge mean score 12.9 ±1.5 showed that mothers had good breastfeeding knowledge. Similar results conducted by Ukegbu14; Mekuria15 showed that mothers with good knowledge have higher rates of exclusive breastfeeding. With more education, mothers’ knowledge on breastfeeding will improve and this will enable them to understand and appreciate the benefits and the seriousness of health challenges associated with suboptimal breastfeeding16.
The Attitude of Mothers Towards Breastfeeding
The overall attitude of mothers towards breastfeeding was fairly 65.9%, while 34.1% had a good attitude which is a majority of those recruited in this study from several ethnic and socio-economic backgrounds. This is the strength of the mothers involved, which should be encouraging for those that might like to study further the attitude of mothers in Suva. Similar studies that showed breastfeeding attitudes rates of more than fifty percent were conducted in Jima town in Ethiopia with 73.9% 17 had favorable breastfeeding attitude. ; MizanAman town, also in Ethiopia with 89.5% 18 and Rwanda, Kigali, with 71.1% 19. The attitude scores of this study were lower than these studies.
About 58.6% of mothers participating in this study agreed to opt for bottle feeding if the baby refuses to suckle on the breast, but this study has not explored whether this is special to first-time mothers, working mothers or all mothers. The study that supported these findings were reported by Lamontagneand his colleagues20; Raffle21 ; Jessy V. Thomas22, who stated that negative attitudes are caused by negative and painful experiences that mothers commonly experienced which includes low milk production; sucking difficulties and refusal by infants; infection of the breast and maternal illness by Doherty, Sanders, 23 and stress by Ugbaoja,24. Mothers need confidence and the desire to successfully breastfeed and such negative experiences affect the attitudes of mothers towards breastfeeding. Expression of breast milk should be demonstrated and taught to mothers as this could help encourage them to continue giving breast milk to their infants even though infants refuse to suckle on the breast. Mothers need to be educated and informed on the risks associated with formula feeds for their infants.
Even though only 8.6% of mothers found breastfeeding in public places unacceptable, the results probably showed the effects of culture. Advocacy and awareness on breastfeeding support from families and communities are important as the community and families need to create conducive environments that support breastfeeding mothers and their infants. The study conducted by Ugbaoja24 supported this finding that the cultural acceptance of breastfeeding can increase its practice given the support they need from the family, community, etc. to overcome the barriers.
Another notable gap found with breastfeeding attitude was the 16.1% of mothers felt that 2 months of maternity leave was not enough to successfully breastfeed their infants if they have to return to work. While maternity leave entitlement for working mothers in Fiji was 84 working days, and equivalent to three months leave reports showed that exclusive breastfeeding in Fiji is still low, especially in the Central Division. The Health workers needed to teach mothers and families how to express breast milk, appropriate storage, and cup feeding for those mothers who have to start work again, the babies continue to receive breast milk. The 2017 World Bank report showed that the female labor force in Fiji was 34.94 % and even though the employment distribution was not recorded, the provision of Crèche rooms for working mothers are important at the workplace to sustain and promote exclusive breastfeeding for first 6 months of life 25.
The Practice of Mothers Related to Breastfeeding
Generally, the mothers’ practice towards breastfeeding in this study was good as the majority (86%) had good scores for breastfeeding practice. 86.0% of mothers were practicing breastfeeding at the time of the study. Some studies were conducted that did not show similar positive results as found in this study. The study conducted by Dun-Dery&Laar in 26 showed that 91 % of participants had knowledge about exclusive breastfeeding but only 10.3 % of them only breastfeed their infants till the sixth month of age. Similar studies conducted by Zhang and Tewabe27 also showed low practice results despite the widespread campaigns about exclusive breastfeeding. This study recorded a result of 55.8% practice of exclusive breastfeeding for the first six months which is quite low when compared with their awareness rate of 92.4% in exclusive breastfeeding.
A notable challenge found in the study regarding mothers’ breastfeeding practice was the significant reduction of breastfeeding rates from birth till discharge (95.2%) with 29%, percentage of infants that were only breastfed before six months of age at home. More than two-thirds of infants (69.6%) were given other milk apart from breast milk at home. The exclusive breastfeeding rate dropped to more than fifty percent from breastfeeding at discharge from the hospital. Like any other activity, breastfeeding can be quite challenging for mothers, especially for young and inexperienced mothers 28, and this is one of the limitations of this study when the status of mothers about this practice was not shown. About 58.6% of mothers in this study had shown that bottle feeding is the appropriate choice they will opt for if they have to return to work and this could be the probable reason why mothers started to bottle feed their infants once they reached home. Working mothers were left with no choice but to feed their infants with breast milk substitutes to be able to meet up their job expectations. Expression of breast milk, storing it in the fridge at the workplace, and bringing the milk at home was a choice for working mothers and this could only be possible if mothers were taught how to express breast milk and how to store breast milk and the workplace had the capacity and provisions for fridges for storage of breast milk for these working mothers. The Public Health Information system (PHIS) of the Ministry of Health and Medical Service 2017/2018 also reflected a similar trend. Lack of confidence in breastfeeding and lack of support for mothers on breastfeeding could have contributed to the giving of formula milk at home for infants. Health workers need to support mothers at postnatal wards and at maternal and child health clinics on a one-to–to-one basis or with their family members and caregivers to ensure that mothers are confident, empowered, and receive support to continue breastfeeding after discharge from the hospital. Networking between health staff and community health workers is very important and should be strengthened to create enabling and supportive environment for breastfeeding in the community. In Ethiopia, the study showed that the cause of low EBF practice was due to the various maternal and child factors and one of those enabling factors related to this study was the receiving of breastfeeding counseling and advice by mothers from the health worker 29.
Determinants of KAP
In this study, five determinants of breastfeeding knowledge, attitudes, and practices were found. Mothers’ number of children was an important determinant in this study as it influenced all; knowledge, attitude, and practices towards breastfeeding. Mothers with more than one child were more likely to have good breastfeeding KAPs than mothers with only one child. The literature reviewed was consistent with the results of this study where mothers with more children were found to have higher rates of exclusive breastfeeding. This was supported by a study conducted in Nigeria that showed that mothers having more children gained more experience and confidence and this positively influenced their breastfeeding practice14. Health workers and family support are needed for mothers with only one child to build their confidence and empower them to positively breastfeed their infants exclusively.
Ethnicity is another important determinant of breastfeeding knowledge and practice in the study. Significantly, the I-taukei mothers were more likely to report good breastfeeding knowledge and practice than mothers with FID and FOD. Ethnicity reflects a cultural characteristic with beliefs and values that set the standard of practice of a group of people or community and society. The cultural environment of I-taukei was more communal and mothers were supported by families and communities, unlike the FID and FOD where communal culture or lifestyle does not exist. The study conducted by Ugbaoja24 and Ajibade30 showed that exclusive breastfeeding was not culturally acceptable and for some was due to husband refusal30. Most women, however, can breastfeed as recommended if they are provided the help they need to overcome breastfeeding barriers related with breastfeeding such as support from in-laws in household chores and promotion of breastfeeding in any public place which is not acceptable by some ethnicities due to their culture31.
Another important determinant of good breastfeeding attitudes and practices in this study was household annual income. Mothers with lower household annual income were more likely to report good breastfeeding attitudes and practices than those with higher household annual income. The study conducted in the Inner-City US showed similar findings that household income had a positive correlation with attitude32. A similar study conducted by Duong16 also supported these findings that income levels affect the feeding choices of mothers, and in this study, more mothers choose other milk apart from breast milk because they can afford and have access to the supplies or the product. Mothers’ status of employment was found to be another factor associated with breastfeeding practices in this study. Significantly, unemployed mothers were more likely to report good breastfeeding practices than mothers that were employed, including mothers that were still schooling. Most studies showed similar findings to this study. The study conducted in Timor-Leste showed a strong association between nonworking mothers and exclusive breastfeeding33. Similarly, in Jordan, the study showed that employed women were less likely to practice full breastfeeding in contrast to unemployed women34. The study further stated that despite the positive attitude women had, the workplace and short maternity leaves negatively impacted breastfeeding. In the United Arab Emirates, a study showed that housewives are more likely to practice exclusive breastfeeding than those mothers who are employed35. However, a study conducted in Hail District, North-Western Saudi Arabia, showed that most mothers stopped breastfeeding because they had to go back to work. In Tanzania, infants were introduced to other foods at the age of three months due to short maternity leave and mothers had to return to work early 36. This finding suggests more support and education on expressed breast milk and cup feeding to working mothers and their families and MOHMS on the promotion of crèche rooms in the workplace.
Another determinant of breastfeeding practice was mothers’ marital status. Mothers with husbands or partners have the additional possibility to exclusively breastfeed their infants compared to single mothers. Similar findings were found in Malawi, which showed the importance and the significant roles of partners for financial support that enabled the mother to have access to the health facility, a positive determinant of exclusive breastfeeding37. Some studies were similar to the findings of this study, but factors like defector relationships showed highly significant breastfeeding practice from married women might require future research.
Conclusion and Recommendations
This breastfeeding knowledge, attitude, and practice (KAP) study provide an important link to the Child Health Policy and Strategy (2015-2020), NCD Strategic Plan (2015-2019); Fiji Wellness Policy (2016) and the Nutrition Strategic Plan 2019 of the Ministry of Health and Medical Services, Fiji. The findings of this KAP study have provided the necessary baseline information and evidence for prioritizing key activity interventions in health centers imparting maternity and newborn services. In this study, knowledge and practices were rated as good while attitudes were rated as fair, however, there were gaps in mother KAPs towards breastfeeding.
Mothers had inadequate knowledge of the maternal health benefits of breastfeeding. Suggested platforms for awareness include the antenatal clinic, women’s reproductive programs coordinated by the local health workers, community health programs, non-governmental and faith-based and women’s group outreach programs in vulnerable areas. Considerable avenues would be in World Health Day celebration centers where our people come freely for health consultation and screening because that is where our public health staff come in numbers to meet with the public and assist them with their needs besides people flocking in numbers for festivity. Ministry of Health and Medical Services staff needs to increase awareness on these important health benefits of breastfeeding to mothers as this would support and increase the exclusive breastfeeding rates for the first 6 months of age. Strengthening family and community support is important to encourage mothers on breastfeeding at home after discharge from the hospital. More advocacy and communication on breastfeeding are needed to bring about the sustainable behavioral change of mothers towards breastfeeding. A supportive environment, especially support from the family, plays an important role in sustaining breastfeeding.
The study makes the following major recommendations based on the results that are expected to enhance and improve the knowledge, attitude, and practices (KAPs) of mothers regarding breastfeeding, and thus improve the breastfeeding rates in Fiji. Strengthen and improve breastfeeding awareness and education in all health care centers and hospitals providing maternity and newborn services. More advocacy and awareness are needed at the community level and faith-based organizations to create and improve positive attitudes towards breastfeeding. Community health workers can be trained to conduct training and awareness on breastfeeding that will help increase the exclusive breastfeeding rates in Fiji. Health workers need to provide more support at the first Maternal Child Health (MCH) clinic visits and thorough breastfeeding assessment to determine the breastfeeding problems that mothers encountered. This support can provide reassurance to breastfeeding mothers and encourage them to re-lactate in the event they have decided or just started to give formula feeding. They may also train mothers to express out breast milk and store it in refrigerators that can be fed to the babies when mothers are separated from their babies as they have to return to work. Further research to be conducted on the 2 main ethnicities; I-taukei and Fijian of Indian Descent (FID) to determine the effects of culture on breastfeeding behavior and practice.
Strength and Limitations of the Study
Firstly, this study has validated the items of the questionnaire to improve the credibility of the researcher’s findings. The second strength of this study was that; it was the first KAP study to be conducted for breastfeeding mothers of babies under six months of age in Suva. This knowledge, attitude, and practice (KAP) study will be used as a baseline to improve exclusive breastfeeding rates in Fiji where the focus is directed to where the gaps are and can be used to strengthen breastfeeding practices among mothers. Breastfeeding is recognized globally as a cost-effective public health approach for the reduction of child and infant morbidity and mortality, so this study can be used by policymakers of the Ministry of Health for planning purposes. The findings of this study can help to develop IEC materials for future mothers which can help to improve and sustain breastfeeding rates among them.
This study had a few limitations that should be taken into consideration as it could affect the results. The findings of this study may not be representative of the breastfeeding situation in other medical areas and other divisions. Therefore, it is vital to conduct a divisional and rural medical area study to explore the levels of knowledge, attitude, and practice (KAPs) for comparative study since Suva is representative of urban medical area settings. Additionally, the sample distribution was more of I Taukei than FID and FOD, therefore, the comparison of knowledge, attitude, and practices (KAPs) with ethnicity cannot be generalized in this study. Working women were not equally represented as they had to rush back to the workplace and could not participate in the study. The response to the questions was based on the memory of the mother, which sometimes may not be accurate.
Acknowledgments
The authors would like to thank all the mothers who participated in the study. The authors will like to thank Fiji National University for providing the necessary support for this study.
Funding Source
This research was conducted as a part of M.T.’s Master of Public health degree at Fiji National University. This research received no external funding.
Conflicts of Interest
The author(s) declare(s) that there is no conflict of interest regarding the publication of this paper.
Author Contributions
Conceptualization, M.T. and P.S.; methodology, M.T. and P.S.; Data analysis, M.T. and S.K. writing—original draft preparation, M.T. review and editing, P.S.; supervision, P.S.; and S.K.; project administration, M.K. All authors have read and agreed to the published version of the manuscript.
References
- World Breastfeeding Week 2020 Message. 2020:2020.
- Reviews S. Evidence on the long-term effects of breastfeeding.
- Black RE, Morris SS, Bryce J. Child survival I Where and why are 10 million children dying every year ? 2003;361:2226-2234.
CrossRef - Seid AM, Yesuf ME, Koye DN. Prevalence of Exclusive Breastfeeding Practices and associated factors among mothers in Bahir Dar city, Northwest Ethiopia : a community-based cross-sectional study. 2013:1-8.
CrossRef - Sibeko L, Dhansay MA, Charlton KE, Johns T, Gray-donald K. Beliefs, Attitudes, and Practices of Breastfeeding Mothers From a Periurban Community in South Africa Beliefs, Attitudes, and Practices of Breastfeeding Mothers From a Periurban Community in South Africa. 2005;(January 2015). doi:10.1177/0890334404272388.
CrossRef - Alamirew MW, Bayu NH, Tebeje NB, Kassa SF. Knowledge and Attitude towards Exclusive Breast Feeding among Mothers Attending Antenatal and Immunization Clinic at Dabat Health Center, Northwest Ethiopia : A Cross-Sectional Institution Based Study. 2017;2017.
CrossRef - Abbreviations LOF. The protective benefit of predominant breastfeeding against otitis media may be limited to early childhood : results from a prospective birth cohort study. :1-24.
- Fein SB, Roe B. The Effect of Work Status on Initiation and Duration of Breast-Feeding. 1998;88(7).
CrossRef - Turconi G, Guarcello M, Maccarini L. Eating Habits and Behaviors, Physical Activity, Nutritional and Food Safety Knowledge and Beliefs in an Adolescent Italian Population Eating Habits and Behaviors, Physical Activity, Nutritional and Food Safety Knowledge and Beliefs in an Adolescent It. 2008;(March). doi:10.1080/07315724.2008.10719672.
CrossRef - Mogre V, Dery M, Gaa PK. Knowledge, attitudes and determinants of exclusive breastfeeding practice among Ghanaian rural lactating mothers. Int Breastfeed J. 2016:1-8. doi:10.1186/s13006-016-0071-z.
CrossRef - Mo O, As U, Ahmed H. Knowledge and practice of exclusive breastfeeding in Kware, Nigeria. 2011;11(3).
- Boateng MF. Knowledge, Attitude and Practice of exclusive breastfeeding among mothers in Techiman, Ghana. Reprod Health. 2018;15(May):140-150. doi:10.1186/s12978-018-0579-3.
CrossRef - Al-binali AM. Breastfeeding knowledge, attitude and practice among school teachers in Abha female educational district, southwestern Saudi Arabia. 2012:1-6.
CrossRef - Ukegbu PO, Ubajaka CF, Bs MB, Medicine C, Azikiwe N, State A. Determinants of breastfeeding patterns among mothers in Anambra. 2011;5(4):112-116.
- Mekuria G, Edris M. Exclusive breastfeeding and associated factors among mothers in Debre Markos, Northwest Ethiopia : a cross-sectional study. 2015:1-7. doi:10.1186/s13006-014-0027-0.
CrossRef - Duong D V, Binns CW, Lee AH. Breastfeeding initiation and exclusive breastfeeding in rural Vietnam Breast-feeding initiation and exclusive breastfeeding in rural Vietnam. 2004;(January 2014). doi:10.1079/PHN2004609.
CrossRef - Months S. Prevalence of Exclusive Breast Feeding and its Predictors Among Infants Aged Prevalence of Exclusive Breast Feeding and its Predictors Among Infants Aged Six Months in Jimma. 2014;(October). doi:10.15406/jpnc.2014.01.00017.
CrossRef - Akinremi ZO, Samuel FO. Knowledge and Attitude of Exclusive Breastfeeding among Hairdresser Apprentices in Ibadan, Nigeria. 2015;5(3):376-385. doi:10.9734/BJMMR/2015/12822.
CrossRef - Jino GB, Munyanshongore C, Birungi F. Knowledge, Attitudes and Practices of exclusive breastfeeding of infants aged 0-6 months by urban refugee women in Kigali. 2013;70(March):7-10.
- Lamontagne C, Hamelin A, St-pierre M. The breastfeeding experience of women with major difficulties who use the services of a breastfeeding clinic : a descriptive study. 2008;13:1-13. doi:10.1186/1746-4358-3-17.
CrossRef - Method AM, Based C, Maonga AR. Factors Affecting Exclusive Breastfeeding among Women in Muheza District, Factors Affecting Exclusive Breastfeeding among Women in Muheza District Tanga Northeastern Tanzania : A Mixed-Method Community Based Study. Matern Child Health J. 2015;(August). doi:10.1007/s10995-015-1805-z.
CrossRef - Thomas J. Barriers to exclusive breastfeeding among mothers during the first four weeks postpartum. Walden Diss Dr Stud. 2016;4(5):1-108.
- Doherty T, Sanders D, Jackson D. Early cessation of breastfeeding amongst women in South Africa: an area needing urgent attention to improve child health. BMC Pediatr. 2012;12(May 2014). doi:10.1186/1471-2431-12-105.
CrossRef - Ugboaja J, Berthrand N, Igwegbe A, OBI-Nwosu A. Barriers to postnatal care and exclusive breastfeeding among urban women in southeastern Nigeria. Niger Med J. 2013;54(1):45. doi:10.4103/0300-1652.108895.
CrossRef - MINISTRY OF HEALTH & MEDICAL SERVICES, Fiji. http://www.health.gov.fj/breastfeeding/
- Dun-dery EJ, Laar AK. Exclusive breastfeeding among city-dwelling professional working mothers in Ghana. Int Breastfeed J. 2016:1-9. doi:10.1186/s13006-016-0083-8.
CrossRef - Tewabe T, Mandesh A, Gualu T, Alem G, Mekuria G, Zeleke H. Exclusive breastfeeding practice and associated factors among mothers in Motta town, East Gojjam zone, Amhara Regional State, Ethiopia, 2015 : a cross-sectional study. 2017:1-7. doi:10.1186/s13006-017-0103-3.
CrossRef - Smith PH. Social Justice at the Core of Breastfeeding Protection, Promotion, and Support : A Conceptualization. 2018. doi:10.1177/0890334418758660.
CrossRef - Arage G, Gedamu H. Exclusive Breastfeeding Practice and Its Associated Factors among Mothers of Infants Less Than Six Months of Age in Debre Tabor Town, Northwest Ethiopia : A Cross-Sectional Study. 2016;2016.
CrossRef - Rn BLA, Ph.D., Rn FOMO, Rn EAO, Ed M. Factors Influencing Initiation of Breast Feeding among Post- Partum Mothers in a Teaching Hospital of Osun State, Nigeria. 2013;3(17):9-15.
- FROM THE FIRST Making the Case for FROM THE FIRST.
- Merewood A, Patel B, Newton KN. Breastfeeding duration rates and factors affecting continued breastfeeding among infants born at an inner-city US Baby-Friendly hospital. Journal of Human Lactation. 2014;(May). doi:10.1177/0890334407300573.
CrossRef - Senarath U, Dibley MJ, Agho K. Breastfeeding practices and associated factors among children under 24 months of age in Timor-Leste. 2007;(October 2014). doi:10.1038/sj.ejcn.1602536.
CrossRef - Khassawneh M, Khader Y, Amarin Z. Jordan : a cross-sectional study. 2006;(May 2014). doi:10.1186/1746-4358-1-17.
CrossRef - Radwan H. Patterns and determinants of breastfeeding and complementary feeding practices of Emirati Mothers in the United Arab Emirates. BMC Public Health. 2013;13(1):1. doi:10.1186/1471-2458-13-171.
CrossRef - Mgongo M, Mosha M V, Uriyo JG, Msuya SE, Stray-pedersen B. Prevalence and predictors of exclusive breastfeeding among women in Kilimanjaro region, Northern Tanzania : a population-based cross-sectional study. Int Breastfeed J. 2013;8(1):1. doi:10.1186/1746-4358-8-12.
CrossRef - Kamudoni P, Maleta K, Shi Z. Exclusive breastfeeding duration during the first 6 months of life is positively associated with length-for-age among infants 6 – 12 months old, in Mangochi district, Malawi. 2014;69(1):96-101. doi:10.1038/ejcn.2014.148.
CrossRef
Accepted on: 02 Sep 2021
Second Review by: Dr. Hasanain Habasha
Final Approval by: Dr. Neha Sanwalka





Web of Science Coverage
Emerging Sources Citation Index (ESCI)
2024 Journal Impact Factor: 1.1
Scopus Journal Metrics
CiteScore 2025: 2.6
CiteScore Details
Sustainable Nutrition: Food Systems, Nutrient Retention, and Public Health Impact
![]()
This journal is a member of, and subscribes to the principles of, the Committee on Publication Ethics (COPE)








