Effects of Chewing Gum Stimuli on General and Emotional Stroop Test
Sung-Yoon WON1 and Dong-Eun LEE2*
and Dong-Eun LEE2*
1Department of Occupational Therapy, Semyung University, Chung-buk, South Korea.
2Department of Dental Hygiene, Ulsan College, Ulsan, South Korea.
Corresponding Author Email: delee@uc.ac.kr
DOI : http://dx.doi.org/10.12944/CRNFSJ.9.2.11
Download this article as:
![]()
The aim of this study was to determine whether chewing gum affects cognitive function and stress relief. Sixty volunteers (mean age 23.3±3.01 years) without general or neuropsychiatric disease were recruited, and Stroop tests and stress surveys were conducted. Volunteers were administered performed a General and Emotional Stroop test with and without chewing gum, and the response time was recorded. The response time after chewing gum was significantly faster while conducting the General Stroop test. Stimulation of chewing gum may increase blood flow to the brain, which results in increased cognitive function. The response time was longer in the incongruent stimuli test compared to the congruent stimuli test, due to the effect of Stroop interference. However, when the chewing gum stimulus was introduced, the possibility of effectively reducing this effect. Stress index and response time of negative stimuli test showed weak positive correlation. This study suggests that chewing gum may play a positive role in increasing cognitive function and relieving stress.
KEYWORDS:Chewing Gum; General and Emotional Stroop Test; Mastication; Stroop Test
Introduction
The aging of the population is accelerating1, and the negative effects caused by tooth loss2 and senile disorder, such as cognitive impairment are increasing3. Also, psychiatric-related diseases caused by stress are increasing recently4. An analysis of recent articles indicates that there is an important correlation between mastication and cognitive function. Chewing gum during the workday increases productivity while reducing cognitive problems5 and it has positive effects on sustained attention in over half of the related existing articles.6 Moreover, there was also an increase in the learning performance in chewers.7 There is a significant association between teeth and cognitive function, for example, tooth loss is a risk factor of dementia.8 Furthermore, the remaining teeth and occlusal balance have a significant correlation with cognitive function in older adults.9 Chewing could also be an active coping strategy for relieving stress.10
The Stroop test is a widely used method for evaluating cognitive function. The General Stroop test (GST) is composed of three conditions: congruent, incongruent, and color stimuli. The Emotional Stroop test (EST) also consists of three conditions: positive, negative, and neutral stimuli. In EST, depressed subjects have a longer response time than non-depressed subjects in negative stimuli.11 For this reason, the EST is widely used in clinical studies related to alcoholism, anxiety, and fear.12
The aim of this study was to determine whether chewing gum affects response time when performing GST and EST. In addition, the relationship between response time of negative stimuli and the subject’s stress index was evaluated. In this study, we evaluated whether chewing gum could help with cognitive function and relieve stress.
Materials and Methods
Participants
This study was approved by the Ethics Committee of Ulsan College (No. 1044363-E-2019-002). After thoroughly explaining the purpose and method of the study, 60 volunteers (mean age 23.3±3.01 years, no personal or family history of general disease, no personal history of neuropsychiatric illness, free of medication) were recruited with written informed consent.
Masticatory Stimuli
A piece of xylitol gum weighing 1.45 g (Seoul, South Korea) was used for masticatory stimuli. Xylitol gum was distributed by researchers to all subjects, therefore the gum was uniform for the population. The duration of chewing was determined by the subjects themselves.
Stroop Test
The Stroop test is divided into GST and EST. GST consists of congruent, incongruent, and color stimuli. In case of the congruent stimuli, the meaning and the word’s font color are matched. Word meaning and font color are not matched in incongruent stimuli. Color stimuli consist of color recognition only (without text). EST consists of positive, negative, and neutral stimuli. In positive and negative stimuli, a word has a positive or negative meaning, individually, whereas the neutral stimuli consist of common words that are neither positive nor negative.
The participants read out the color of the font, ignoring the meaning of the word, in the Stroop test. The time was recorded during the test.
Experimental Protocols
Considering that the time span may be shortened by the effect of experience when implementing the Stroop test, the participant group was randomly divided in half. In the first group (30 participant), the time was recorded after performing the Stroop test. The next day, the Stroop test was repeated with participants chewing gum, and the time was recorded again. The second group (the remaining 30 participant) was examined in the reverse order. Then, participants randomly selected one of six stimuli (three in GST, three in EST) and participated in a test. They took a break with or without chewing gum before the start of the tests, which were performed in a blind manner. Recorded data were collected and then statistically processed (Figure 1).
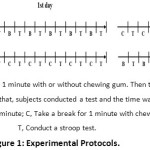 |
Figure 1: Experimental Protocols. |
Questionnaire for Measuring Stress Index (Table 1)
Stress response inventory (SRI) is one questionnaire used for stress self-diagnosis.13, 14 It was used to measure the subjects’ stress index. SRI contains emotional, somatic, cognitive, and behavioral stress responses with 39 questions under the seven subscales (tension, aggression, somatization, anger, depression, fatigue, and frustration). In the subscales, tension includes six items (questions 2, 16, 17, 30, 31, and 37), aggression includes four items (questions 18, 28, 29, and 33), somatization includes three items (questions 6, 7, and 10), anger includes six items (questions 4, 24, 25, 26, 27, and 34), depression includes eight items (questions 5, 15, 19, 22, 23, 35, 38, and 39), fatigue includes five items (questions 1, 12, 13, 14, and 36), and frustration includes seven items (questions 3, 8, 9, 11, 20, 21, and 32).
The SRI consists of 39 questions that are answered using a rating scale (Never: 0, Almost Never: 1, Sometimes: 2, Fairly Often: 3, and Very Often: 4 points for a total of 0 to 156 points). After the participants had answered the questionnaire, the total score was calculated by summing up the points for each question.
Table 1: Stress Response Inventory (SRI)
| Questions | Never | Almost Never | Some-times | Fairly Often | Very Often |
| 1. I make many mistakes at work | □ | □ | □ | □ | □ |
| 2. I don’t feel like talking | □ | □ | □ | □ | □ |
| 3. My chest feels tight | □ | □ | □ | □ | □ |
| 4. I feel angry | □ | □ | □ | □ | □ |
| 5. I feel agitated and restless | □ | □ | □ | □ | □ |
| 6. I suffer from indigestion | □ | □ | □ | □ | □ |
| 7. My stomach hurts | □ | □ | □ | □ | □ |
| 8. I feel like screaming | □ | □ | □ | □ | □ |
| 9. I often sigh | □ | □ | □ | □ | □ |
| 10. I feel dizzy | □ | □ | □ | □ | □ |
| 11. Everything bothers me | □ | □ | □ | □ | □ |
| 12. I have distracting thoughts | □ | □ | □ | □ | □ |
| 13. I am easily fatigued | □ | □ | □ | □ | □ |
| 14. I feel totally exhausted | □ | □ | □ | □ | □ |
| 15. I have lost my self-confidence | □ | □ | □ | □ | □ |
| 16. I feel tense | □ | □ | □ | □ | □ |
| 17. My body trembles | □ | □ | □ | □ | □ |
| 18. I feel like hitting someone | □ | □ | □ | □ | □ |
| 19. I have lost incentive to do anything | □ | □ | □ | □ | □ |
| 20. I feel like crying | □ | □ | □ | □ | □ |
| 21. I feel on edge | □ | □ | □ | □ | □ |
| 22. I have no future in my current work | □ | □ | □ | □ | □ |
| 23. I often stare blankly | □ | □ | □ | □ | □ |
| 24. I hate someone | □ | □ | □ | □ | □ |
| 25. I can’t get that thought out of my head | □ | □ | □ | □ | □ |
| 26. My voice is louder than it usually is | □ | □ | □ | □ | □ |
| 27. I easily get impatient | □ | □ | □ | □ | □ |
| 28. I act violently(such as reckless driving, cursing, fighting | □ | □ | □ | □ | □ |
| 29. I feel like breaking something | □ | □ | □ | □ | □ |
| 30. I talk less than I used to | □ | □ | □ | □ | □ |
| 31. My head hurts or it feels heavy | □ | □ | □ | □ | □ |
| 32. My heart throbs | □ | □ | □ | □ | □ |
| 33. I feel like killing someone | □ | □ | □ | □ | □ |
| 34. My face gets flushed or it feels hot | □ | □ | □ | □ | □ |
| 35. I feel bored | □ | □ | □ | □ | □ |
| 36. I have lost my patience | □ | □ | □ | □ | □ |
| 37. My face looks rigid | □ | □ | □ | □ | □ |
| 38. I am useless (or unworthy) | □ | □ | □ | □ | □ |
| 39. I don’t like moving any part of my body | □ | □ | □ | □ | □ |
Data Analysis
All statistical analyses were performed using SPSS 12.0 (SPSS Inc., Chicago, IL, USA). Data were evaluated by paired T-test and regression and correlation analysis. p<0.05 was considered statistically significant.
Results
General Stroop Test (Figure 2)
As a result of time measurement during the congruent stimuli test without chewing gum, the average recorded time was 21.7 s. After chewing gum, the average recorded time was 18.6 s with masticatory stimuli, the time required for the test was reduced by 3.2 s, which is statistically significant (p<0.01). For the incongruent stimuli recorded in subjects with and without chewing gum, the average times were 29.6 s and 34.6 s, respectively. The time reduction was 5.1 s (p<0.01). For the color stimuli, the average times with and without masticatory stimuli were 21.0 and 24.0 s, respectively and the time reduction was 3.0 s (p<0.01). The average time was longer for incongruent stimuli than congruent stimuli (without chewing gum: 12.9 s more, with chewing gum: 11.0 s more). The color stimuli test took more time than the congruent stimuli and less time than incongruent stimuli tests regardless of the presence of masticatory action. (data not shown).
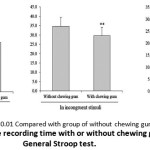 |
Figure 2: Average Recording Time With or Without Chewing Gum in General Stroop Test. |
Emotional Stroop Test (Figure 3)
As a result of measuring time during positive stimuli test without chewing gum, the average duration was 27.5 s. After chewing gum, the average time was 23.3 s. This means that with masticatory stimuli, the time required for the test reduced by 4.1 s, which is statistically significant (p<0.01). For the negative stimuli, the average recorded times in subjects with or without chewing gum were 24.8 s and 28.9 s, respectively, with a time reduction of 4.1 s (p<0.01). In case of the neutral stimuli, the average times with or without masticatory stimuli were 24.6 s and 27.4 s, with a time reduction of 2.7 s (p<0.05). The average time was longer for negative stimuli than positive stimuli (without chewing gum: 1.4 s more, with chewing gum: 1.5 s more). The neutral stimuli test took more time than the positive stimuli and less time than the negative stimuli tests, without the effect of chewing gum (data not shown).
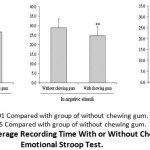 |
Figure 3: Average Recording Time With or Without Chewing Gum in Emotional Stroop Test. |
Questionnaire Results for Stress Self-Diagnosis (Table 2)
All participants responded to the SRI questionnaires, and the total scores were calculated by adding the points assigned to each question. The average score was 33.2 (±9.90) points. Among the seven subscales, the most common response was fatigue, followed by depression, frustration, anger, and tension. There were few responses of aggression (Table 2).
Table 2: Questionnaire Results for Stress Self-Diagnosis.
| Subscales | Response rate after summing up the points |
| Fatigue | 25.2% |
| Depression | 19.6% |
| Frustration | 19.6% |
| Anger | 14.6% |
| Tension | 11.9% |
| Somatization | 7.7% |
| Aggression | 1.5% |
Relationship Between Stress Index and Stroop Test Results
The correlation between the individual stress index and the time required for the negative stimuli test without chewing gum showed a weak positive correlation (r=0.166) and no significant correlation. In addition, the test showed a weak positive correlation (r=0.256) when measuring the connection between the reduced time in the negative stimuli test, with or without chewing gum, and the stress index.
Discussion
Previous research has shown that the response time was faster when the Stroop test was performed after the participants had chewed gum.15 However, that pilot study was conducted with 14 participants and, accordingly, there was no statistically significant difference. In addition, there is no existing research showing whether chewing gum affects the response time for EST. To bridge this gap, 60 volunteers were recruited for this study, and the effect of chewing gum on the EST was evaluated.
In this study, the response time after chewing gum was significantly faster while conducting the GST. The reason for this can be deduced from a comparison to previous studies. Chewing increases regional cerebral blood flow in the sensorimotor16-18, supplementary motor16, 17, insula16, 17, thalamus16-18, cerebellum16-18 and striatum19, bilaterally. Moreover, chewing increases blood oxygenation level dependent signals in the right prefrontal area, unilaterally.17 Existing research also suggests that mastication increases blood flow in the prefrontal cortex and hippocampus, which are related to learning and memory function.20 From the results of these studies, it can be interpreted that chewing gum stimulation increased blood flow to the brain, increasing cognitive function and reducing the response time when the Stroop test was administered.
Loss of teeth decreases gray matter volume around the hippocampus and the amount of the frontal lobe20, which then affects cognitive function.8 Extraction and decreasing of the height of the occlusal reduced hippocampal nerve reduces learning and spatial memory in rats.21 In the Mini-Mental State Examination, the score was higher in patients with natural teeth than patients with prosthetic treatment20, and this kind of brain activity was influenced by the type of prosthetic treatment.22 In rats, the number of hippocampal dentate gyrus cells decreased in the soft diet feeding group compared to the hard diet feeding group22, 23, and a hard diet was more conducive to learning and memory recovery than a soft diet.22 Therefore, chewing gum may play a positive role in maintaining cognitive function, and restoration of tooth loss will be important for cognitive function.
In this study, the longer response time in the incongruent stimuli test compared to the congruent stimuli test may be due to the Stroop interference effect.24 This is because there is a semantic relationship between words and colors. The longer response time is due to the suppression process of the frontal lobe, which means that this process requires cognitive attention. Interestingly, response time for congruent stimuli decreased by 3.2 s after chewing gum, but it decreased by 5.1 s for incongruent stimuli after chewing gum. This suggests that the incongruent stimuli test process takes more time due to the Stroop interference effect, but when the chewing gum stimulus is introduced, there is a possibility that this effect is reduced.
Interestingly, depressed subjects have a longer response time when performing the negative stimuli test than the positive stimuli test in EST. Consequently, EST is used to measure selective attention, cognitive flexibility, processing speed, and executive functions. In particular, it has most frequently been used to measure selective attention, which is when an individual focuses on a specific target while ignoring other elements of the environment.25
We hypothesize that the performing of the negative stimuli test in higher stress index groups takes more time. However, the stress index and response times on the negative stimuli test showed weak positive correlation. Considering the characteristics of the volunteers, it seems that this correlation was due to their young age, with no relation to personal or family history of general disease and neuropsychiatric illness.
This study provides evidence for applying chewing gum to clinical situations. First, chewing gum is non-invasive, familiar, and easy to use. Second, through the use of chewing gum, social costs for senile disorder treatment can be reduced. Due to the increase in the population of older adults, medical costs such as prosthetic treatments and drug treatments for dementia are increasing. Chewing gum stimulates saliva secretion, increasing the autopurification in the oral cavity and protecting oral health. Furthermore, it can also increase mastication, and cognitive ability can thus be maintained. Chewing gum cannot be applied to older adults who have already lost their teeth, but it can be applied as a simple tool to prevent further tooth loss, at least for those who have remaining teeth. Third, chewing gum is a simple and easy way to reduce stress. One of the most common ailments in modern society is psychiatric disease caused by stress. Breathing, exercise, meditation, drug therapy and expert counseling are used to address these problems, and treatment can take a long time (particularly with a lack of will) and be expensive. However, chewing gum requires a relatively low cost and effort. Therefore, more research on chewing gum should be conducted, and this study will provide a solid foundation for future research.
This study has several limitations. First, the duration and force of chewing were not uniform (because focusing on the chewing would have interfered with the cognitive tests). Second, if the number of samples would be increased, the reliability of the data would further improve.
Further studies will need to determine whether chewing gum has a positive effect on patients with cognitive impairment and stress-induced mental illness.
Conclusion
The response time after chewing gum was significantly faster while conducting the GST. It could be that chewing gum stimulus increased blood flow to the brain, which increased cognitive function. Moreover, the response time was longer in the incongruent stimuli test than in the congruent stimuli test, which could be due to the Stroop interference effect. It is possible to effectively reduce the Stroop interference effect through the introduction of a chewing gum stimulus. Finally, the stress index and response times on the negative stimuli test showed a weak positive correlation.
Conflict of Interest
The authors declare that there are no conflicts of interest.
Acknowledgement
This study was not supported by funding from any foundation in the commercial, private, or not‐for‐profit sectors.
Funding Sources
The authors received no financial support for the research, authorship, and or publication of this article.
References
- Korea Social Statistics. Estimation of future population (Population Estimates and Population Projections). Statistics Korea, 2019.
- Lima Saintrain MV, Souza EHA. Impact of tooth loss on the quality of life. Gerodontology, 2012;29:e632-e636.
CrossRef - Dal Forno G, Kawas CH. Cognitive problems in the elderly. Curr Opin Neurol, 1995;8:256-261.
CrossRef - Marin FM, Lord C, Andrews J, Juster RP, Sindi S, Arsenault-Lapierre G, Fiocco AJ, Lupien SJ. Chronic stress, cognitive functioning and mental health. Neurobiol Learn Mem, 2011;96(4):583-595.
CrossRef - Allen AP, Smith AP. Chewing Gum: Cognitive Performance, Mood, Well-Being, and Associated Physiology. Biomed Res Int, 2015,654806.
CrossRef - Hirano Y, Onozuka M. Chewing and Attention: A Positive Effect on Sustained Attention. Biomed Res Int, 2015:367026.
CrossRef - Wilkinson L, Scholey A, Wesnes K. Chewing gum selectively improves aspects of memory in healthy volunteers. Appetite, 2002;38(3):235-236.
CrossRef - Luo J, Wu B, Zhao Q, Guo Q, Meng H, Yu L, Zheng L, Hong Z, Ding D. Association between Tooth Loss and Cognitive Function among 3063 Chinese Older Adults: A Community-Based Study. PLoS One, 2015;10(3):e0120986.
CrossRef - Park TJ, Jung YS, Son K, Bae YC, Song KB, Amano A, Choi YH. More Teeth and Posterior Balanced Occlusion Are a Key Determinant for Cognitive Function in the Elderly. J Appl Oral Sci, 2012;20(1):64-9.
- Kubo KY, Iinuma M, Chen H. Mastication as a Stress-Coping Behavior. Biomed Res Int, 2015,876409.
CrossRef - Gotlib IH, McCann CD. Construct accessibility and depression: An examination of cognitive and affective factors. J Pers Soc Psychol, 1984;47(2),427-439.
CrossRef - Richards A, French CC, Johnson W, Naparstek J, Williams J. Effects of mood manipulation and anxiety on performance of an emotional Stroop task. Br J Psychol, 1992:83(4),479-491.
CrossRef - Kim CH. Questionnaire Methods for Measuring Stress. Korean J Stress Res, 2006:14(2),63-68.
- KB Koh, Park JK, Kim CH, Cho S. Development of the Stress Response Inventory and Its Application in Clinical Practice. Psychosom Med, 2001;63(4):668-78.
CrossRef - Kawakami Y, Takeda T, Konno M, Suzuki Y, Kawano Y, Ozawa T, Kondo Y, Sakatani K. Relationships between Gum Chewing and Stroop Test: A Pilot Study. Adv Exp Med Bio, Chapter 30, 221-226. 2017.
CrossRef - Onozuka M, Fujita M, Watanabe K, Hirano Y, Niwa M, Nishiyama K, Saito S. Mapping Brain Region Activity during Chewing: A Functional Magnetic Resonance Imaging Study. J Dent Res, 2002:81(11),743-746.
CrossRef - Onozuka M, Fujita M, Watanabe K, Hirano Y, Niwa M, Nishiyama K, Saito S. Age-related Changes in Brain Regional Activity during Chewing: A Functional Magnetic Resonance Imaging Study. J Dent Res, 2003:82(8),657-660.
CrossRef - Lin CS. Meta-analysis of brain mechanisms of chewing and clenching movements. J Oral Rehabil, 2018:45(8),627-639.
CrossRef - Momose T, Nishikawa J, Watanabe T, Sasaki Y, Senda M, Kubota K, Sato Y, Funakoshi M, Minakuchi S. Effect of mastication on regional cerebral blood flow in humans examined by positron-emission tomography with 15O-labeled water and magnetic resonance imaging. Arch Oral Biol, 1997:42,57-61.
CrossRef - Krishnamoorthy G, Narayana AI, Balkrishanan D. Mastication as a tool to prevent cognitive dysfunctions. Jpn Dent Sci Rev, 2018:54(4),169-173.
CrossRef - Teixeira FB, Pereira Fernandes LM, Noronha PA, dos Santos MA, Gomes-Leal W, Ferraz Maia CS, Rodrigues Lima R. Masticatory Deficiency as a Risk Factor for Cognitive Dysfunction. Int J Med Sci, 2014:11(2),209-214.
CrossRef - Hara T, Kawanishi K, Ohno A, Iida S. The evolution of research on occlusion and brain function. J Prosthodont Res, 2017:61(1),6-8.
CrossRef - Aoki H, Kimoto K, Hori N, Toyoda M. Cell proliferation in the dentate gyrus of rat hippocampus is inhibited by soft diet feeding. Gerontology, 2005:51(6),369-374.
CrossRef - Gul A., Humphreys G.W. Practice and colour-word integration in Stroop interference. Psicológica, 36,37-67.
- Feist GJ, Rosenberg EL. Psychology: making connections. (p 1-673). JR Son, HJ Kang, KH Kim (Eds.) Kyobobook, Paju: South Korea. 2011.
Accepted on: 16 April 2021
Second Review by: Aditi Chopra India
Final Approval by: Prof. Rajesh Jeewon





Web of Science Coverage
Emerging Sources Citation Index (ESCI)
2024 Journal Impact Factor: 1.1
Scopus Journal Metrics
CiteScore 2025: 2.6
CiteScore Details
Sustainable Nutrition: Food Systems, Nutrient Retention, and Public Health Impact
![]()
This journal is a member of, and subscribes to the principles of, the Committee on Publication Ethics (COPE)








