Artificial Intelligence Approach for Analyzing Anaemia Prevalence in Children and Adolescents in BRICS Countries: A Review
Natisha Dukhi1*
, Machoene Derrick Sekgala1 and Olushina Olawale Awe2, 3 1Human and Social Capabilities Division, Human Sciences Research Council, Merchant House, 116-118 Buitengracht Street, Cape Town, South Africa.
2Department of Mathematical Sciences, Anchor University Lagos, Lagos, Nigeria.
3Institute of Mathematics and Statistics, Federal University of Bahia (UFBA), Salvador, Brazil.
Corresponding Author Email: doctordukhi@gmail.com
DOI : http://dx.doi.org/10.12944/CRNFSJ.9.1.01
Download this article as:
![]()
Anemia prevalence, especially among children and adolescents, is a serious public health burden in the BRICS countries. This article gives an overview of the current anaemia status in children and adolescents in three BRICS countries, as part of a study that utilizes an artificial intelligence approach for analyzing anaemia prevalence in children and adolescents in South Africa, India and Russia. It posits that the use of machine learning in this area of health research is still novel. The weightage assessment of the crosslink between anaemia risk indicators using a machine learning approach will assist policy makers in identifying the areas of priority to intervene in the BRICS participating countries. Health interventions utilizing artificial intelligence and more specifically, machine learning techniques, remains nascent in LMICs but could lead to improved health outcomes.
KEYWORDS:Adolescents; Anaemia; BRICS; Children; Machine Learning
Introduction
In mobilizing cooperation for nutrition and addressing the various forms of malnutrition, including micronutrient deficiencies, the BRICS countries have made some significant strides. The BRICS nations, composed of Brazil, Russia, India, China and South Africa, contributing to 42% of the global population, are making efforts towards achieving declines in undernourishment and reducing hunger. South-South cooperation is instrumental in promoting health and well-being via nutrition and addressing malnutrition and the economic and social burden as it impacts individuals, communities and populations globally1. Common amongst BRICS countries such as Russia, India and South Africa is the issue of anaemia in children and adolescents. Globally, and according to the World Health Organization (WHO), anaemia is a major and common public health concern affecting both the developed and developing countries. The most vulnerable age groups affected are young children aged less than five years old, adolescents and women of childbearing age. An estimated 42% of children under age five and 40% of pregnant women are anaemic globally2. The most recent national surveys in the three BRICS countries indicate the following: in children under the age of five years in South Africa, the anaemia prevalence was 10.7% in 2012, as per the South African National Health and Nutrition Examination Survey (SANHANES-1). The 2016 South African Demographic and Health Survey indicated anaemia prevalence at 61% and a further 2% of children (aged 6-59 months) were severely anaemic 3, 4. In India, anaemia in children aged 6-59 months was recorded at 58% in the National Family Health Survey 2015-2016 5. Russia has no current survey data on child, adolescent and/or adult anaemia prevalence despite the country reporting challenges with iron deficiency disorders6. From the afore-mentioned BRICS countries, only India report anemia prevalence among adolescent males and females, while South Africa reports adolescent anaemia only in the 15-19 year age group and iron deficiency in females only. This is highly concerning, as adolescence is a unique age period whereby a child transitions to an adult, with a possibility of health problems arising in childhood being continued through adulthood, affecting the quality of life.
Anaemia occurs when the number of red blood cells or the haemoglobin concentration within the cells are lower than normal. Haemoglobin is essential for oxygen transportation and a lower than normal level of this protein or abnormal red blood cells results in a decreased capacity of the blood to carry oxygen to the body tissues. A person with anaemia may experience dizziness, weakness, fatigue, and shortness of breath. Optimal haemoglobin concentration in the body essential for physiological needs to be met varies by sex, age, pregnancy status, smoking habits and geographical location. Common causes of anaemia include nutritional deficiencies such as iron deficiency, as well as deficiencies in vitamin B12, folate and Vitamin A; infectious diseases that include malaria, tuberculosis (TB), and Human Immunodeficiency Virus (HIV), , parasitic infections and haemoglobinopathies. Iron deficiency anaemia (IDA) remains the major global cause of anaemia, with sub-Saharan Africa and Asia having a greater iron deficiency and infection burden 2, 7.
An essential micronutrient, iron, is necessary for maintaining the cell structure and function in the body, as well as being a component of proteins such as haemoglobin, that is vital for transportation of oxygen to the body tissues8. During childhood, a common nutrition deficiency form such as iron deficiency, is a result of a constant negative iron balance that is affected by iron utilization or absorption, inadequate dietary intake, an increased requirement of iron during the growth periods, as well as blood loss due to malaria and soil-transmitted helminth infections. Hence, IDA is defined by both anaemia and a deficiency of iron9. In children, IDA impairs both intellectual and growth development. The brain is most vulnerable during the first two years of life and the third pregnancy trimester. Iron deficiency can result in neuropsychological effects associated with cognitive impairment in childhood and during adolescence10.
Experimental and epidemiological data have suggested that while the impairments may occur early in life, they may be reversible through public health interventions that promote dietary diversification with foods rich in micro-and macro-nutrients and vitamins, as well as mass fortification of staple foods, and micronutrient supplementation11. In adolescents, anaemia is a leading cause of morbidity, triggered by various factors such as genetic conditions, nutritional deficiencies and infections. During the adolescent growth period, in addition to energy requirements, there are also increased nutrient and protein needs, including the need for iron, which supports the growth process. As females enter the childbearing years micronutrient deficiencies and insufficient iron stores are a major cause of concern due to the increased nutrient demands during pregnancy and lactation. The adolescent stage of life is a unique time period during which nutrition can be addressed. Adolescent data for dietary intake in low- and middle-income countries (LMICs) is minimal, and data on iron supplementation during pregnancy exists but there is a need for overall nutrition coverage in adolescents12. In women of reproductive age, risk of anaemia increases during menstruation, and during pregnancy, the risk of anaemia may increase due to placental and foetal requirements and bleeding during delivery. Children with an anaemic mother are vulnerable as maternal iron deficiency is associated with increased infant mortality. The deficiency also affects birth weight and gestation duration in women with premature infants or those of low birth weight7.
This review paper gives an overview of the current anaemia status in children and adolescents in three BRICS countries, as part of a study that utilizes an artificial intelligence approach for analyzing anaemia prevalence in children and adolescents in South Africa, India and Russia.
National and regional studies that reported on child and adolescent anemia in the three countries were reviewed to provide an overview of the trends and prevalence of anemia in these countries. The following search strings were used: “anaemia + children + Russia”, “anemia + adolescents + Russia”, “anaemia + children + India”, “anemia + adolescents + India”, “anaemia + children + South Africa”, “anemia + adolescents + South Africa”. The alternate spelling of anaemia, that is ‘anemia’ was also used. Keywords such as ‘Young people’ and ‘teenagers’ was also used in place of adolescents.
The national prevalence rates of anaemia reported in this review were obtained from cross sectional national surveys. These surveys employ stratified cluster probability sampling techniques to ensure that the selection of households and respondents is nationally representative. These surveys also typically apply analysis weights to the estimates that adjust for non-response and sample selection probabilities, to calculate nationally representative estimates of anaemia prevalence. Artificial Intelligence is a huge field that comprises Machine Learning (ML) and Deep Learning (DL). The use of both AI and ML approach has increased recently in many areas of research. AI and ML are often used interchangeably because ML is a subset of AI. ML relies on algorithms to analyze large datasets and it is capable of performing predictive analytics faster than any human can. Machine learning algorithms are modern model-free data analytic methods that provide efficient solutions to classification problems in public health research. Traditional statistical analysis had focused on methods like logistic regression (LR) which is the most widely used statistical method for handling classification problems in medical statistics13. The focal point of many of the anaemia risk analysis techniques is the accurate prediction of the disease. Moreover, machine learning, as a part of AI, is becoming popular in the field of medical and health research for predictive analytics purposes and pattern recognition14. Several machine learning techniques have been applied to predict the prevalence of various diseases including Anaemia15.
Anaemia Prevalence in South Africa
Anaemia prevalence remains relatively high in children in South Africa, as observed in the national surveys. Some South African studies have found that almost a third of children and women were anaemic16, 17. South Africa, whilst undergoing a nutrition transition, is also undergoing an epidemiological transition, whereby together with prevalence of TB and HIV, there is an alarming increase in non-communicable diseases (NCDs) such as some forms of cancers, cardiovascular disease (CVD), chronic respiratory disease and diabetes18, 19. These further contribute to the morbidity and mortality burden. Since 2016, there has been no follow up national survey to identify any further increases in anaemia prevalence in children as well as the reporting of new cases. This may be attributed to the current nutrition transition in South Africa, characterized by increased Westernized diets high in fats, sugar, refined carbohydrates and animal products in place of traditional diets high in fibre; irregular, nutritionally unbalanced meals, aggressive fast food marketing, sedentary lifestyles, and adverse economic, social and environmental conditions20, 21. This has led to suboptimal diets replacing traditional diets, and is further attributed to social inequality and poverty that puts individuals at risk of micronutrient deficiencies17. The most recent national surveys that assessed the prevalence of anaemia in young children and adults were conducted in 20123 and in 20164.
The South African National Health and Nutrition Examination Survey (SANHANES-1), in comparison to the other South African national surveys, provides a more comprehensive picture of anaemia prevalence in children below five years of age. When comparing it to other national surveys, Anaemia prevalence in 1994 was 21.4%, rising to 28.9% in 2005, with a decline in 2012 at 10.7%. IDA has also shown a decrease from 5.0% in 1995, rising sharply in 2005 to 11.3% and declining again in 2012 to 1.9%. However, iron deficiency/depletion did not follow this trend. Iron deficiency in 1995 was recorded at 4.8%, increased further in 2005 to 7.8%, with a further increase in 2012 to 8.1%3.
At both regional and global levels, while South Africa does fare better regarding anaemia prevalence in children in comparison to children in the rest of Africa, there are differences when compared to children in high-income regions22. In 2013, while the global anaemia prevalence was 43.0%, 46% of this was in southern Africa, with only 11.0% in high-income regions9. In a further comparison of SANHANES-1 to NHANES 1999-2000 conducted in the USA23, anaemia prevalence was higher in SANHANES-1 at 10.7% compared to NHANES at 5.1%. Findings of SANHANES-1 indicate that there was a marked reduction in anaemia in children below the age of five years and this may have been attributed to the national food fortification programme, better infant and child feeding practices, better micronutrient supplementation programmes, as well as an improvement in primary healthcare8.
The lattermost South African Demographic and Health Survey (SA DHS) was conducted in 20164. While this was the first DHS to measure anaemia prevalence in children and adults, it did not measure iron status. The study found that anaemia among children aged 6-59 months was 61% and 2% were severely anaemic. The authors noted that these rates were much higher than expected considering the results of other national studies and advised for the findings to be interpreted with caution4.
Furthermore, anaemia prevalence, in an important developing and decision-making group, adolescents, is still not frequently reported /not given priority in South Africa. In the SANHANES 2012, the highest prevalence of anemia in females was found among adolescent girls aged 15-18 years, where 32.5% were anemic (Hb<=12 g/dL). Adolescent girls aged 15-18 also had the highest prevalence of iron depletion (8.8%) and an IDA prevalence (20.2%) that was more than twice that of 19-24 and 25-35 year old women (7.8% and 8.8% respectively). Overweight adolescent girls were three times more likely to be anaemic17. The SA DHS of 2016 found that among 15-19 year olds, 34% of females and 17.2% of males were anaemic4.
Anaemia Prevalence in India
The comprehensive data set on the nutritional status of Indian children aged 0-19 year old is included in the Comprehensive National Nutrition Survey (CNNS). The CNNS surveys considered one of the largest micronutrient survey ever conducted worldwide. Additionally, for the first time in India, CNN employed gold standard methods for assessment of anaemia and other micronutrient deficiencies as well as associated risk factors of non-communicable diseases (NCDs). There was no sufficient data on children aged 5-14 years, while this assumes special significance as this age group encompasses around one-quarter of the whole population yet receive less attention and are considered more vulnerable. More importantly is that these children depend mostly on the school feeding programs24.
Anaemia is a major public health issue affecting most importantly women, girls, and children. Apart from adversely affecting physical well-being and increasing the rate of deaths, slowed mental and motor activities development and high risk of maternal mortality are significantly associated with anaemia25. As reported globally, hemoglobin level measured by iron deficiency is the important cause for anaemia and other forms of nutritional insufficiencies. The shortage of iron in the blood leads to low blood cell levels and negatively affects the development of unborn babies. Another cause of iron deficiency is poor nutrition and contributes to more than 60% of all anaemia cases26. These might be explained by the fact that during adolescence, iron requirements increase to support growth in both girls and boys. Additionally, girls have slightly higher requirements due to menstruation27.
According to the Global Burden of Diseases in 2016, Anaemia cases in India contributed almost one quarter to the global burden26. Moreover, the International Institute for Population Sciences reported that the majority of women aged 12-51 years and children less than 5 years were anaemic28. Although anaemia prevalence is higher among pregnant girls than non-pregnant girls in most regions, the high prevalence of anaemia in both girls and boys continues to indicate a need for interventions to address anaemia in ways that effectively reach all adolescents29. Therefore, the CNNS focused more on collecting data on undernutrition and associated factors among these vulnerable groups.
The prevalence of anaemia in preschoolers aged 1-4 years is 41%, 24% in children between the age of 5-9 years, and 28% in adolescents between the ages of 10-19 years. However, the severity of anaemia differs among age groups. Preschoolers had 22%,18%, and 1% of mild anaemia, moderate anaemia, and severe anaemia, respectively. School-age children had 10%,13%, and 1% of mild anaemia, moderate anaemia, and severe anaemia, respectively. Adolescents had 17%, 10%, and 1% of mild anaemia, moderate anaemia and severe anaemia, respectively. As compared to those currently out of school, the prevalence of anaemia was higher in children between the age of 5-9 years (32% vs. 23%) and adolescents between the age of 10-19 years (36% vs. 26%)24.
When compared with the National Family Health Survey29, in total, 58% of children had some form of anaemia. The prevalence of mild anaemia, moderate anaemia and severe anaemia in children were 28%, 29%, and 2%, respectively. The NFHS-4 shows a substantial decline in anaemia between the age of 6-59 months in children, down started 69% in 2005-2006 to 58% in 2015-20165. Anaemia prevalence in children between the ages of 6-59 months has been persistently higher among rural children30. Similarly, the NFHS 4 (2015-16) reveals that anaemia is more prevalent among children than among older children. Anaemia is higher in children of anaemic mothers than in mothers without anaemia. With the existing different nutrition programs aiming at women and children, India still not achieve the nutrition target. Therefore, machine learning might be a great investment in nutrition to clarify how key malnutrition indicator such as anaemia remained a health problem and which other key factors remain to be overlooked by the existing policy approaches in place among Indian population30.
Anaemia Prevalence in Russia
Despite its public health importance, data on anaemia and its associated risk factors in Russia remains missing or outdated31. Using keywords such as “anaemia,” “children,” “adolescents,” “Russia,” “Russian Federation” did not yield any up to date information on the anaemia status in Russia. We utilized the UNICEF Situation Analysis of Children in the Russian Federation 2007 report to provide some background on the anaemia status within the country6. As per the report, during the 1990’s anaemia prevalence was on the increase in pregnant women, resulting in likely more low birth weight babies and premature delivery occurrences. Women with anaemia in 2002 accounted for 42.8% of all pregnancies that resulted in childbirth and was an increase by a 3.5 factor from 1990 and 11.6 factor from 1980. Iron deficiency disorders (IDDs) are a noted problem in Russia, despite universal salt iodization. A national survey in 2005 indicated 29.0% of Russian households consumed iodized salt32. Inadequate iodine supply to populations was indicated by regional surveys, resulting in endemic goitre6. Russian production process, manufacturing, quality control, packaging and supply of iodized salt has improved. Yet despite these efforts, public awareness on iodized salt benefits have been minimal or absent. The health of children in Russia is also affected by the threat of IDA. Between 1992-2002, anaemia in children quadrupled from 452 to 1 821 per 100 000 children, and then decreased in 2004 to 1 599 per 100 000 children. During their first year of life children are more likely (50%) to have a less than average height. Additionally, their cognitive and physical development may be impaired and their immune systems may be compromised32. This is of great concern as new data on anaemia prevalence in children and adolescents may provide a more comprehensive understanding of anaemia status in BRICS countries, its associated risk factors and the impact on health outcomes.
Artificial Intelligence Approach for Analyzing Anaemia Prevalence
The use of Artificial Intelligence (AI) in medicine entails the utilization and application of modern computer algorithms and software that emulates human cognition in the analysis and interpretation of complicated medical data33. In particular, AI is the ability of computer algorithms to reason like humans and approximate conclusions without direct human involvement. Previous nutrition studies relied largely on outcomes from the statistical analyses conducted. While such studies assist in disease diagnosis, they do not extend to processing of large-scale data that may uncover different relationships and patterns that may be influential34. Currently, most literature regarding anaemia prevalence in young children, adolescents and adults is based on traditional statistical analysis methods such as ANOVA, regression, descriptive analysis, as well as dimension reduction techniques35. If the introduction of using artificial intelligence techniques can be compared to the current technique features and/or create new comparisons or features, this can raise the attention of both researchers and policymakers globally. Machine learning (ML), an area intersecting statistical analysis and artificial intelligence research (see Figure 1), allows for the exploration of big data on nutrition to discover relationships or patterns that are unknown in big data34.
Methods such as support vector machine, random forest, and decision trees have been employed to classify the status of various diseases. However, very few studies have considered the use of machine learning techniques to construct prediction models for childhood and adolescent anemia in BRICS nations13. Recommended AI (Machine Learning) methods for detecting and characterizing Anemia prevalence in children and adolescents include Discriminant Analysis (DA), K-Nearest Neighbors (k-NN), Classification and regression trees (CART), Support Vector Machines (SVM) and Random Forest (RF). What makes machine learning efficient and advantageous over other methods includes the fact that it does not involve human intervention since it means giving machines the ability to learn, it lets them make predictions and also improve the algorithms on their own. Also, machine learning allows for continuous improvement in accuracy and efficiency of the algorithms which also allows for better decisions. Suppose we need to make an anemia prevalence forecast model, as the amount of data we have keeps growing, your algorithms learn to make more accurate predictions faster. Machine Learning algorithms are also good at handling data that are multi-dimensional and multi-variable. They are capable of identifying trends and patterns easily. Machine learning algorithms can be used to characterize large volumes of nutrition data to discover specific trends and patterns that would most often not be discovered by the ordinary statistical model36.
Discriminant analysis (DA) is a supervised machine learning approach for pattern classification, which aims to find a linear combination of features that characterizes two or more classes of events using the Bayes’ classifier37. It assumes that the predictors are drawn from multivariate Gaussian distribution. It is a dimensionality reduction technique used as a pre-processing step in Machine Learning. The ability to accurately classify medical observations and outcomes is highly useful for various policy applications in medicine.
K-Nearest Neighbors (k-NN) is a robust non-parametric classifier which falls into the supervised learning family of machine learning algorithms that stores and classifies all available new data based on a similarity measure. An object would be classified by a majority vote of its neighbors, while being assigned to the class which is most common amongst its k nearest neighbors measured by a distance function15. Classification and regression trees (CART) is a non-parametric machine learning algorithm used for the purpose of classification of a large set of data using the predictive structure of the problem under consideration. It is a predictive method which explains how a response variable’s values can be predicted based on other values (predictors).
When the response variable is continuous, CART produces regression trees, and whenever the response variable is categorical, it produces classification trees38. The Support Vector Machines (SVM) algorithm is a supervised machine learning technique which is widely used in classification and regression problems. Given a set of training data, the SVM algorithm constructs a model that separates the training data perfectly according to their categories39. Apart from being able to perform linear classification and regression, SVM can also perform a non-linear classification by separating data input variables into high-dimensional feature spaces (also known as feature selection).
Random forest (RF) is a supervised machine learning classification technique, which is based on “growing” an ensemble of tree structured classifiers40. It is one of the most powerful supervised machine learning algorithms which can also perform regression tasks if the outcome is a continuous variable. This algorithm creates a forest with a number of decision trees. It basically consists of a several separate decision trees that operate as an ensemble which can be used for model prediction. To classify a new individual, features of this individual are then used for classification41. It can handle large datasets with high dimensionality.
When medical data are unlabeled, supervised machine learning techniques such as classification and regression are not feasible, otherwise, unsupervised machine learning techniques (clustering methods) are required, which attempts to find new natural clustering of the data into separate new groups38. These machine learning techniques occupy the heart of AI and would be mostly used in future studies of anaemia prevalence in BRICS nations. Figure 1 depicts the definition of the major parts of AI.
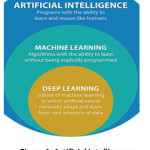 |
Figure 1: Artificial Intelligence, Machine Learning and Deep Learning42 |
Advances in both mobile computing power and information technology infrastructure in LMICs give hope to utilizing artificial intelligence to address the current public health challenges43. As we see a rise in global health challenges, AI can enable researchers to observe and understand behaviour and health states of individuals as well as their feeding patterns44. Regarding anaemia, the proper diagnosis and interventions may assist in reducing anaemia risk with the development of medical tools for risk assessment. In risk assessment techniques, the focal point is the accurate prediction of the disease or condition. In some countries and studies, machine-learning techniques have been used in the classification status of diseases such as acute appendicitis41, diabetes38, 45, 46 and multiple sclerosis15.
However, construction of predictive models for childhood anaemia prevalence using machine learning is minimal47. Machine learning, a fast becoming popular model in health research, is able to assist in the development of models for prediction purposes and is utilized in some nutrition studies34. For example, machine-learning algorithms have been used to integrate blood parameters, physical activity and gut microdata to accurately predict the human response to actual meals48.
Techniques such as random forest machine learning models have been used to find correlation between obesity and microbiome changes49. Furthermore, supervised machine learning approaches have been used to track blood sugar levels in check by targeted nutritional models50. While the use of machine learning to investigate nutritional status in children has been conducted in India35, as far as we are aware of, there is no such study where machine learning was used to understand the issues of anaemia prevalence at multivariate level in these selected BRICS nations.
Concluding Remarks
This article has given an overview of the current anaemia status in children and adolescents in three BRICS countries, as part of a study that utilizes an artificial intelligence approach for analyzing anaemia prevalence in children and adolescents in South Africa, India and Russia. It posits that the use of machine learning in this area of health research is still novel. The weightage assessment of the crosslink between anaemia risk indicators using machine-learning approach will assist policy makers in identifying the areas of priority to intervene. This will also create the space for optimizing a predictive model to ensure a contextualized state action plan at a policy level in the BRICS participating countries. Health interventions utilizing artificial intelligence and more specifically, machine learning techniques, remains nascent in LMICs but could lead to improved health outcomes. Crucial empirical results would be reported in our future works.
Acknowledgements
The authors wish to thank Mr. Dennis Dogbey for his continuous work and support on this study.
Funding Sources
This work is based on the research supported by the National Research Foundation (Ref number BRIC190307422517).
Author Contributions
ND conceptualized and designed the study; ND, RS, MDS and OOA contributed equally to the manuscript.
Conflict of Interest
The author(s) declares no conflict of interest.
References
- Food and Agriculture Organization. Experience of BRICS countries in the development of nutrition-sensitive social protection programmes. Geneva. http://www.fao.org/3/a-i6073e.pdf 2016. (Accessed 12 November 2020)
- World Health Organization, “Anaemia,”Geneva. https://www.who.int/health-topics/anaemia#tab=tab_1 2018. (accessed on 17 June 2020).
- Shisana O., Labadarios D., Rehle T., Simbayi L., Zuma K., Dhansay A., Reddy P., Parker W., Hoosain E., Naidoo P., Hongoro C., Mchiza Z., Steyn N. P., Dwane N., Makoae M., Maluleke T., Ramlagan S., Zungu N., Evans M. G., Jacobs L., Faber M., the SANHANES-1 Team South African National Health and Nutrition Examination Survey (SANHANES-1). 2014 Edition. Cape Town: HSRC Press. 2014.
- National Department of Health (NDoH), Statistics South Africa (Stats SA), South African Medical Research Council (SAMRC), and ICF. South Africa Demographic and Health Survey 2016. Pretoria, South Africa, and Rockville, Maryland, USA: NDoH, Stats SA, SAMRC, and ICF.2019.
- Ram F., Paswan B., Singh S. K., Lhungdim H., Sekhar C., Singh A. National family health survey-4 (2015-2016). Econ Pol Weekly. 2017;52(16):66-70.
- Dedov I. I., Melnichenko G. A., Troshina E. A., Platonova N. M., Abdilkhabirova F. M., Shatnuk L. N., Apanasenko B. P., Kavtaradze S. R., Arbuzova M. I., Dzhatoeva F.A. Iodine Deficiency: Threats to the Health and Development of Children in Russia. Ways to Resolving the Problem: National Report, Moscow. 2006.
- Thejpal R. Iron deficiency in children. S. Afr. Med. J. 2015;105(7):607.
CrossRef - Hlatswayo B.P.S., Ntshangase S. and de Villiers F.P.R. The effects of iron deficiency and anaemia on primary school learners’ scholastic performance. S Afr J Child Health. 2016; 10 (2):111-115.
CrossRef - World Health Organization. “Serum ferritin concentrations for the assessment of iron status and iron deficiency in populations.” Vitamin and Mineral Nutrition Information System. Geneva: World Health Organization (WHO) (WHO/NMH/NHD/MNM/11.2), 2011. http://www.who.int/vmnis/indicators/serum_ferritin.pdf (accessed on 17 June 2020).
- Grantham-McGregor S., Ani, C. A review of studies on the effect of iron deficiency on cognitive development in children. J Nutr. 2001; 131: 649S-648S.
CrossRef - DeMaeyer E.M., Dallmanm P., Gurney J.M., Hallberg L., Sood S.K., Srikantia S.G. Preventing and controlling iron deficiency anaemia through primary health care. Geneva. WHO, 1989. http://www.who.int/nutrition/publications/micronutrients/anaemia_iron_deficiency/
9241542497/en/index.html (accessed on 17 June 2020). - Benedict R. K., Schmale A., and Namaste S. Adolescent Nutrition 2000-2017: DHS Data on Adolescents Age 15-19. DHS Comparative Report No. 47. Rockville, Maryland, USA: ICF. (2018).
- Khan J.R., Chowdhury S., Islam H. & Raheem E. Machine learning algorithms to predict the childhood anemia in Bangladesh. Journal of Data Science. 2019; 17(1):195-218.
- McLachlan G.J. Discriminant Analysis and Statistical Pattern Recognition. New York: Wiley Interscience. (2004).
- Zhao Y., Healy B.C., Rotstein D., Guttmann C.R., Bakshi R., Weiner H.L., Brodley C.E. & Chitnis T. Exploration of machine learning techniques in predicting multiple sclerosis disease course. PloS one. 2017; 12(4): e0174866.
CrossRef - Mamabolo R.L. & Alberts M. Prevalence of anaemia and its associated factors in African children at one and three years residing in the Capricorn District of Limpopo Province, South Africa’, Curationis. 2018;37(1): 9.
CrossRef - Mchiza Z.J., Parker W., Sewpaul R., Job N., Chola L., Mutyambizi C., Sithole M., Stokes A. and Labadarios D. Understanding the determinants of hemoglobin and iron status: adolescent–adult women comparisons in SANHANES-1. Ann. N.Y. Acad. Sci. 2018; 1(1416): 31–47.
CrossRef - Franks P., Hanson R.L., Knowler W., Sievers M., Bennett P.H. and Looker H.C. Childhood Obesity, Other Cardiovascular Risk Factors, and Premature Death. New England Journal of Medicine. 2010; 1: 362.
CrossRef - Hanvey A.N., Mensah F.K., Clifford S.A. & Wake M. Adolescent Cardiovascular Functional and Structural Outcomes of Growth Trajectories from Infancy: Prospective Community-Based Study. Childhood Obesity. 2017; 13(2): 154-163.
CrossRef - Waxman A. & Norum K.R. Why a global strategy on diet, physical activity and health? The growing burden of non-communicable diseases, Public Health Nutrition. 2004; 7(3): 381–383.
CrossRef - Popkin B.M. Global nutrition dynamics: the world is shifting rapidly toward a diet linked with non-communicable diseases, American Journal Clinical Nutrition. 2006; 84: 289.
CrossRef - Stevens G.A., Finucane M.M., De-Regil L.M., Paciorek C.J., Flaxman S.R., Branca F., Peña-Rosas J.P., Bhutta Z.A. & Ezzati M., (on behalf of Nutrition Impact Model Study Group (Anaemia). Global, regional, and national trends in haemoglobin concentration and prevalence of total and severe anaemia in children and pregnant and non-pregnant women for 1995–2011: A systematic analysis of population-representative data. Lancet Global Health. 2013; 1: e16–25.
CrossRef - Baker R.D., Greer F.R., & The Committee on Nutrition. Diagnosis and prevention of iron deficiency and iron-deficiency anemia in infants and young children (0–3 Years of Age). Pediatrics. 2010; 126(5): 1040–1050.
CrossRef - Ministry of Health and Family Welfare (MoHFW), Government of India, UNICEF and Population Council. Comprehensive National Nutrition Survey (CNNS) National Report. New Delhi. (2019)
- World Health Organization. “Indicators for assessing infant and young child feeding practices: part 2: measurement,” 2010. https://www.who.int/nutrition/publications/infantfeeding/9789241599290/en/ (accessed on 17 June 2020).
- Kassebaum N.J. The global burden of anemia. Hematology/Oncology Clinics. 2016; 30(2): 247-308.
CrossRef - Spear B.A. Adolescent growth and development. Journal of the Academy of Nutrition and Dietetics. 2002; 1: S23.
CrossRef - Kotecha P.V. Nutritional anemia in young children with focus on Asia and India. Indian journal of community medicine: official publication of Indian Association of Preventive & Social Medicine. 2011; 36(1): 8.
CrossRef - Rao S., Joshi S., Bhide P., Puranik B. and Kanade A. Social dimensions related to anaemia among women of childbearing age from rural India. Public Health Nutrition. 2011; 14(2): pp.365-372.
CrossRef - Ncogo P., Romay-Barja M., Benito A., Aparicio P., Nseng G., Berzosa P., Santana-Morales M.A., Riloha M., Valladares B. & Herrador Z. Prevalence of anemia and associated factors in children living in urban and rural settings from Bata District, Equatorial Guinea, 2013. PloS one. 2017; 12(5).
CrossRef - Bikbov M.M., Kazakbaeva G.M., Zainullin R.M., Salavatova V.F., Gilmanshin T.R., Yakupova D.F., Uzianbaeva Y.V., Arslangareeva I.I., Panda-Jonas S., Mukhamadieva S.R., Khikmatullin R.I., Aminev S.K., Nuriev I,F., Zaynetdinov A.F. and Jonas J.B. Prevalence and associated factors of anemia in a Russian population: the Ural eye and medical study. BMC Public Health. 2019; 19:762, 1-15.
CrossRef - UNICEF. Situation Analysis of Children in the Russian Federation, 2007. https://www.unicef.org/sitan/files/ru_en_situation-analysis_170907.pdf (accessed on 17 June 2020).
- Mitchell R.S., Michalski J.G. & Carbonell T.M. An artificial intelligence approach. Springer, Berlin. (2013).
- Witten I.H., Frank E., Hall M.A. & Pal C.J. Data Mining: Practical machine learning tools and techniques. 3rd edition. Science Direct. 2011; 607-629.
CrossRef - Khare S., Kavyashree S., Gupta D. & Jyotishi A. Investigation of Nutritional Status of Children based on Machine Learning Techniques using Indian Demographic and Health Survey Data. Procedia Computer Science. 2017; 115: 338–349.
CrossRef - Ali J., Ahmad A., George L. E., Der C. S., & Aziz S. A Review Of Machine Learning Techniques And Statistical Models In Anaemia. International Journal of Scientific & Technology Research. 2013; 2(2), 171-175.
- Izenman A.J. Linear discriminant analysis, Modern Multivariate Statistical Techniques, Springer. 2008; 237-280.
CrossRef - Choi S.B., Kim W.J., Yoo T.K., Park J.S., Chung J.W., Lee Y.H., Kang E.S. & Kim D.W. Screening for prediabetes using machine learning models. Computational and Mathematical Methods in Medicine. 2014; 618976.
CrossRef - Guyon I., Weston J., Barnhill S. & Vapnik V. Gene selection for cancer classification using support vector machines. Machine Learning. 2002; 46:389–422.
CrossRef - Breiman L. Random forest. Machine Learning. 2001; 45:5–32.
CrossRef - Hsieh C.H., Lu R.H., Lee N.H., Chiu W.T., Hsu M.H. & Li Y.C. Novel solutions for an old disease: diagnosis of acute appendicitis with random forest, support vector machines, and artificial neural networks. Surgery. 2011; 149(1):87-93.
CrossRef - IBM. Model Asset eXchange on IBM Developer, 2020. https://www.ibm.com/za-en (accessed on 17 June 2020).
- Schwalbe N. and Wahl B. Artificial intelligence and the future of global health, 2020. https://www.sciencedirect.com/science/article/pii/S0140673620302269 (accessed on 17 June 2020).
- Bullock J., Pham K.H., Lam C.S.N. and Luengo-Oroz M. Mapping the landscape of artificial intelligence applications against COVID-19. arXiv preprint arXiv:2003.11336. (2020).
CrossRef - Yu W., Liu T., Valdez R., Gwinn M. & Khoury M.J. Application of support vector machine modeling for prediction of common diseases: the case of diabetes and pre-diabetes. BMC Medical Informatics and Decision-Making. 2010; 10(1):16.
CrossRef - Meng X.H., Huang Y.X., Rao D.P., Zhang Q. & Liu Q. Comparison of three data mining models for predicting diabetes or prediabetes by risk factors. The Kaohsiung Journal of Medical Sciences. 2013; 29(2):93-9.
CrossRef - Sanap S.A., Nagori M. & Kshirsagar V. Classification of anemia using data mining techniques. In International Conference on Swarm, Evolutionary, and Memetic Computing. 113-121. Springer, Berlin, Heidelberg. (2011).
CrossRef - Zeevi, D., Korem, T., Zmora, N., Israeli, D., Rothschild, D., Weinberger, A., Ben-Yacov, O., Lador, D., Avnit-Sagi, T., Lotan-Pompan, M. & Suez, J. Personalized nutrition by prediction of glycemic responses. Cell. 2015; 163(5):1079-94.
CrossRef - Sze, M.A. & Schloss, P.D. Looking for a signal in the noise: revisiting obesity and the microbiome. MBio. 2016; 7(4):e01018-16.
CrossRef - McDonald, D., Glusman, G. & Price, N.D. Personalized nutrition through big data. Nature Biotechnology. 2016; 34(2):152.
CrossRef
Accepted on: 10 Dec 2020
Second Review by: Zoobi Khanam
Final Approval by: Neha Sanwalka





Web of Science Coverage
Emerging Sources Citation Index (ESCI)
2024 Journal Impact Factor: 1.1
Scopus Journal Metrics
CiteScore 2025: 2.6
CiteScore Details
Sustainable Nutrition: Food Systems, Nutrient Retention, and Public Health Impact
![]()
This journal is a member of, and subscribes to the principles of, the Committee on Publication Ethics (COPE)








