Impact of Mother-to-Mother Support Groups in Promoting Exclusive Breastfeeding in a Low-Resource Rural Community in Kenya: A Randomized Controlled Trial
Joseph Kobia M’Liria
and Sophie Ochola Department of Foods, Nutrition and Dietetics, Kenyatta University, Nairobi, Kenya.
Corresponding author email: mwitiliria@gmail.com
DOI : http://dx.doi.org/10.12944/CRNFSJ.8.2.26
Download this article as:
![]()
Breastfeeding is the single most effective intervention for growth, health, development and survival of infants. Exclusive breastfeeding (EBF) for 6 months alone can reduce under-five child mortality by up to 13%. Community-based strategies such as Mother-to-Mother Support Groups (MTMSGs) have improved the rates of EBF by increasing the length of maternal support before and after delivery. The rate of EBF in the study area was 18.6%, which was lower than national rate of 32% at the time of the study. Currently, the Kenyan national rate is 61% but with high regional variability. This study was designed to assess the impact of community-based MTMSGs with or without income generating activities in promoting EBF in low socio-economic rural setting in Kenya.
This was a cluster randomized controlled trial in which 3 health centres in Igembe South Sub-County in Meru County, Kenya were randomly allocated to three study groups, on a ratio of 1:1:1; to two treatment groups and a control group. The target population was pregnant mothers in their third trimester (33-37 weeks) and registered at ante-natal clinics in any of the 3 health centres. Total sample size was 249. Mothers in the first treatment group received breastfeeding education and support during seven monthly meetings by trained breastfeeding peer educators. Mothers in the second treatment group received breastfeeding education and support at the same frequency as those in first group in addition to conducting income generating activities facilitated by the research team. Mothers in the control group received no breastfeeding education. Infant feeding practices were determined based on 24–hour recall. Data was collected on monthly basis for 6 months postpartum by interviewers blinded to the study hypotheses. The primary outcome was EBF prevalence at six months while secondary outcome was cumulative EBF at six months.
Mothers in the first and second treatment groups were two times more likely to exclusively breastfed at 6 months compared to mothers in the control group [RR=2.42;CI 1.36-4.28;(p=0.004] and [RR=1.89;CI 1.02-3.49;(p=0.033)] respectively. There was no significant difference in the EBF rates at 6 months in the 2 treatment groups. Median duration of cumulative EBF for the control group was significantly lower at 0.7 months compared with first treatment group at 2.8 months (p<0.001) and second treatment group at 3.4 months (p<0.001). Mother-to-mother support groups is an effective strategy in promoting exclusive breastfeeding in low socio-economic rural settings and should therefore be strengthened in Kenya and similar circumstances.
Breastfeeding; Breast-Feeding Promotion; Exclusive Breastfeeding; Mother-to-Mother Support Groups; Randomized Controlled Trial
Background
Breastfeeding is the single most effective intervention for growth, health, development and survival of infants. Exclusive breastfeeding (EBF) provides infants with optimal nutrition requirements. Studies have demonstrated a number of short-term and long-term nutrition, health and socio-economic benefits associated with breastfeeding. EBF protects infants against illnesses such as: respiratory diseases, diarrhoea, allergies, asthma, obesity and human immune-deficiency virus (HIV) infection. Mothers who exclusively breastfeed their infants have delayed onset of menstrual periods, have less risk of breast/ovarian cancers and experience better bonding with their infants.1-5 Early initiation to breastfeeding within one hour of birth, a critical indicator of EBF, saves 22% of infants from neonatal deaths. Combined with EBF, they would reduce neonatal mortality by 35%.(6-7) Globally the rates of EBF have been increasing in the recent past with UNICEF reporting that 39% of the world’s newborns aged 0-5 months were exclusively breastfed for 6 months in 2015.8-9 Recently, there has been improvement in the EBF rates in Kenya from 32% to 61 % (between 2009 and 2014).10-11 however, the country still has one of the lowest EBF rates in Sub-Saharan Africa. The study also showed that 15% of the infants had been introduced to complementary feeding before the age of six months. Slightly over one in ten (13%) of children less than 6 months were introduced to liquid feeds other breast milk of which 10% were given milks like formula milk while 3% were given non-milk liquids. One-tenths (10%) of the infants were on predominant breastfeeding with only water being given with breast milk.11
EBF is one of the cardinal components of the Baby Friendly Hospital Initiative (BFHI) aimed at protecting, promoting and supporting breastfeeding for optimal maternal and child health globally.12 BFHI has been widely promoted across the world by UNICEF and WHO as one of the strategies of ensuring optimal breastfeeding practices among the mothers. The 10th step of BFHI recommends fostering the establishment of breastfeeding support groups and refer mothers to them on discharge from the hospital or clinic. Upon discharge from the hospital, the mothers are referred to organised community-based support groups such as mother-to-mother support groups (MTMSGs), peer-counselling groups and mother support groups (MSGs). These groups offer support to the mother on breastfeeding and other aspects of childcare. The goal of these community-based approaches is to increase the length of infant breast-feeding support the mother gets before and after delivery.13
Community-based strategies improve the rates of EBF by increasing the length of maternal support before and after delivery. These strategies have been demonstrated by several studies to improve the rate of EBF. In a study carried out in Ghana using peer counsellors, the intervention group with the longest period of maternal support pre-, peri- and post-natally was found to have the highest rate of EBF at 6 months (90.4%).14 In a different study involving community health workers in Burkina Faso and Uganda,15 the intervention groups (in Burkina Faso) showed significant improvement in rates of EBF. Another community strategy that has demonstrated significant impact in increasing the rates of EBF is the Baby Friendly Community Initiative (BFCI) which was implemented in Cambodia and has led to improvement of EBF from 11.4% to 73.5% between 2000 and 2010. Notably, BFCI- Cambodia involves multiple strategies including MSGs, health providers and media but it did not include MTMSGs.16 Peer-counseling has demonstrated that the frequency of the counseling sessions received from a trained breastfeeding counselor significantly influences the length of exclusive breastfeeding.17-18
In Kenya, two studies carried out using peer counseling approach; first study in an informal settlement in Nairobi, Kenya17 and second study involving couple counseling in Nyando- a rural district in Kenya18; demonstrated the positive impact of using trained peer counselors to promote EBF. In a case study of MTMSGs conducted by Muruka and Ekisa19 on impact of MTMSGs on maternal, infant and child nutrition (MIYCN) in Wajir and Habaswein Districts in Kenya, EBF rate improved from 21.1% to 53.7% after one year of intervention. The design of the Habaswein study was a case study; it had no control group, neither was it randomized.
Mother-to-Mother Support Groups (MTMSGs) is one of the community-based approaches to improving optimal breastfeeding rates. MTMSGs are composed of pregnant, lactating mothers as well as care-givers that come together to support one another as and to learn more on infant and young child feeding practices. Usually a professional facilitator (peer counsellor) or one member of the group, who is trained in facilitation skills as well as on infant and young child feeding practices, facilitates the meetings13
MTMSGs are one of the strategies promoted by UNICEF worldwide for the improvement of infant young child feeding practices. In Kenya, there is paucity of information on the role of MTMSGs in improving infant and young child feeding despite the fact that the Ministry of Health (MoH) and UNICEF are promoting their use.21 There is no scientific study, to the knowledge of the authors, investigating the impact of the MTMSGs in promoting EBF in Kenya. One of the major challenges identified in MTMSGs is the sustainability of the groups and it has therefore been suggested that there may be need to introduce an income generating activity or activities (IGAs) in addition to the promotion of appropriate EBF practices to motivate women to consistently attend the meetings.20 Prior to this study, there were no breastfeeding MTMSGs in the study area (Igembe South Sub-County) as demonstrated by the findings of a preliminary study in the study area conducted by the researcher in 2011. The rate of EBF in the study area was 18.6%, which was much lower than the national rate of 32% at the time of the study.21 There was need therefore, to introduce and investigate the impact of MTMSGs (with and without IGAs) in improving the practice of EBF in the study area to provide evidence-based data on the impact of this strategy in promoting exclusive breastfeeding rates.
Methodology
Ethical Approval
Ethical clearance was obtained from Kenyatta National Hospital/University of Nairobi (KNH/UoN) Ethical Review Committee, Nairobi, Kenya (KNH-ERC/A/343).
Trial Registration Number: PACTR201910846018049.
Study Setting
The study was conducted in Igembe South Sub-County in Meru County, Kenya. The area had a high malnutrition rate of 21% underweight compared to national prevalence of 16% and a high childhood mortality of 35 deaths per 1000 live births.21 The study also showed that 15 percent of the infants had been introduced to complementary feeding before the age of six months. Thirteen percent (13%) of children less than 6 months were introduced to liquid feeds other breast milk of which 10% were given other milks like formula milk while 3% were given non-milk liquids. 10% of the infants were on predominant breastfeeding with only water being given with breast milk.11
Study Design
The study adopted a cluster randomized controlled trial research design (22) to assess the impact of community-based MTMSGs in promoting exclusive breast-feeding for the first 6 months of life among mothers participating in the MTMSGs. There were 3 study groups; a control group (CG) and two treatment groups each made up of 6 MTMSGs of at most 15 mothers each. The treatment groups were: Mother-to-mother Support Group with education and support (MES) and Mother-to-mother Support Groups with breastfeeding education and support and income generating activities (MESIGA). In case of MESIGA, care was taken to spend more time on breastfeeding support before the start of income generating activities (IGA) to avoid mind shift among mothers to income rather than breastfeeding.
Sample Size and Sampling
The sample size for this study was derived using formula by Kelsey (23) and Fleiss.(24) Total sample size was calculated using CDC Statistics Calculator with the following parameters put into consideration: power of test at 80%; ratio of sample size, intervention/control ratio of 2, and pre-intervention prevalence of 19% EBF rate, post-intervention prevalence of 40% and significance level of 5%. The calculated sample size was 180 participants inflated by 23% to make 222 mothers due to possible attrition from still births, low birth weights and defaulters. During the recruitment exercise, slightly more mothers were recruited into the 3 groups (CG-79, MES-82 and MESIGA-88). The total number of mothers recruited was 249; however, the difference was not significant between the 3 study groups.
Randomization
Three health centres were randomly assigned to the three study groups: MES, MESIGA and CG. Randomization was computer generated on a 1:1:1 ratio using Micro-Soft Excel 2003 Software by an independent biostatistician without knowledge of the study area and the study hypotheses. Health centres rather than the study participants were randomized to minimize cross-contamination of expected outcomes if mothers from the same health centre were assigned to different study groups. The study participants were recruited from the records of antenatal clinics (ANC) at the 3 health centres they were attending. The recruitment was done by the principal investigator assisted by the ANC nurse at each of the 3 health centres.
Study Participants
The study participants were pregnant mothers in their third trimester (33-37 weeks gestation) attending ANC clinics at the 3 health centres. Inclusion criteria were: a) Mothers who were HIV negative b) been residents in the study area for at least 6 months c) planning to continue staying in the study site for at least 7 months from the time of recruitment into the study; and d) no history of complications of the current pregnancy based on medical records. The participants were informed of the study purpose but not the hypotheses. The recruitment was done by informed consent by signing or thumb print. Screening and recruitment of mothers was carried out continuously until all the 3 study groups attained the required sample size.
Selection and Training of MTMSGs’ Facilitators and Enumerators
Five females with a minimum of secondary school education (12 years) and residents of the study area were recruited as MTMSGs’ facilitators. The training of facilitators and enumerators was conducted by the principal investigator assisted by a breastfeeding counsellor. The content of this training included: advantages of EBF; breastfeeding myths; early initiation and sustenance of breastfeeding as well as MTMSG facilitation skills.25 The selection criteria for the six enumerators were similar to those of the MTMSGs’ facilitators. The principal investigator conducted a 3-day training using FANTA/WHO Anthropometric Guidelines.26 The content included: interviewing techniques to collect data on maternal infant feeding practices as well as how to take infant anthropometric measurements. The two groups were trained separately.
Blinding Design
The nurses/health staff and data collectors at the 3 health centres involved in the study and mothers were blinded to the study hypotheses. The MTMSGs’ facilitators were aware of the interventions for their specific treatment groups because they were supposed to promote and support EBF. There was no interaction between the enumerators and the MTMSGs’ facilitators to avoid bias during data collection. Only the principal investigator was aware of the study hypotheses.
Description of the Interventions
Control Group- (CG)
Mothers in this study group received only the standard infant and young child nutrition/health education offered at the health facility which was composed of nutrition/health sessions usually given at the ANC/MCH clinics by the nurse-in-charge. Each session lasted 40 minutes with about 10 minutes spent on nutrition issues, with minimal information on breastfeeding. The nutrition/health education was given in group sessions and was conducted irregularly depending on availability of health staff and time. This group received no additional education on breastfeeding issues from the research team.
Treatment Group 1- MES
Mothers in this study group received breastfeeding education (with focus on EBF) and support such as infant attachment to the breast, positioning, rooming in and breastfeeding on demand. The group was composed of 6 MTMSGs of at most 15 mothers each to facilitate easy sharing of breast-feeding information and support for each other. Each discussion session lasted one hour as per the MTMSG Facilitator’s Manual which was used as a standard for all MTMSGs (25). At each meeting, one topic on breastfeeding was discussed in a session moderated by a trained facilitator. The MTMSGs groups met on a monthly basis; once prenatally and 6 times post-natally. The discussion topics included: advantages of EBF; breastfeeding myths; early initiation and sustenance of breastfeeding as well as management of common breastfeeding challenges. Each topic was discussed at a different MTMSG meeting. Participants did not receive any other education or counselling on EBF after the MTMSG meetings but the group members could consult one another or the facilitators any time they encountered challenges on breastfeeding. All group meetings were held at the nearest health facility as agreed by each group members.
Treatment Group 2- MESIGA
The recruitment of mothers and formation of the MTMSGs in this study group; conducting of MTMSG meetings and breastfeeding support were carried out in a similar fashion as in MTMSGs in Treatment Group one. However, after the stipulated one hour meeting was over, mothers in this study group carried out an income generating activity (IGA) for another one hour starting from the second to seventh month of study. They made liquid soap which they used themselves or sold to their neighbours. Before the start of the study, mothers indentified their preferred IGA as liquid soap making. During the second month, a-one day training for liquid soap making was carried out in the 6 MTMSGs in MESIGA study group by the researcher assisted by a volunteer mother with experience in soap making from an established MTMSG in Thika, Kiambu County, Kenya. The content of the IGA training involved; practical mixing of soap ingredients, packing of the soap, selling and utilization of the soap as well as sustaining the income generating activity. Mothers in this group bought soap they made and sold the rest to their neighbours and friends in order to sustain the IGA. IGAs were included to increase MTMSGs attendance by the group members.
Determination of Infant Feeding Practices
The primary outcome of this study was EBF during the first six months as determined by cross-sectional data (based on 24-hour recall) on a monthly basis and EBF determined by cumulative EBF from birth to 6 months. Infants who were fed on only breast milk and received medicine and/or oral rehydration salts were considered as exclusively breastfed.
Interviews
The study used WHO27 and Ochola et al.,17 validated questionnaires. The questionnaires were pre-tested for clarity and accuracy on 10% of the sample size at a different site with similar characteristics to the selected study site. A total of seven interviews were carried out with the mothers from the 3 study groups to establish their infant feeding practices: a baseline interview was conducted within one week after recruitment at the health facility; second interview within the first month postpartum. The third to seventh interviews were conducted on a monthly basis with mothers from the three study groups with the last (seventh) interview being conducted at 6 months after delivery at the health facilities.
Pretesting of Data Collection Tools
The data collection tools were pretested on 11 pregnant mothers in their 3rd trimester (33-37 weeks gestation) and 11 lactating mothers with infants <6 months old. A health centre which was comparable in characteristics to the 3 health centres selected for the study but not part of the study was selected. The pre-testing was conducted on a 10% of the sample.
Statistical Data Analysis
Data was analysed using SPSS version 17.0 and SAS 9.3 version 9.3 software packages. Kruskal-Wallis and Chi-square tests were used to analyse for differences between means of continuous data with non-normal distribution. Kaplan-Meir Survival analysis was used to determine cumulative exclusive breastfeeding among the three study groups. The level of significance was set at a p-value of <0.05 for all statistical tests.
Results
Enrolment Process and Trial Profile for Study Participants
A total of 1,537 pregnant women attending ANC clinics were invited to participate in the study. Of the potential 390 participants who met the inclusion criteria, 141 of them declined to participate in the study resulting to 249 mothers being qualified for the study (63.8% response rate). Slightly more mothers were recruited than the calculated sample size but the difference was not significant. Mothers gave different reasons for declining to participate such as long distance from home, husband did not offer consent for participation in the study and those who expected to relocate within the study period. Of the 249 mothers qualified for the study, 88 (35.6%) were in the MESIGA, 82 (32.9%) were in MES and 79 (31.5%) were in CG) (Figure 1).
 |
Figure 1: A schematic presentation of the participants’ recruitment into the study |
Comparisons of the 3 Study Groups at Baseline
There were no significant differences in the baseline characteristics of the participants in the three study groups indicating that randomization was successful (Table 1).
Table 1: Maternal household socio-demographic and education characteristics by study groups.
| Study Groups | |||||
| Maternal Characteristics | MESGA(N=88) | MES(N=82) | CG(N=79) | Total(N=249) | Chi-sq, KW & Median testp-value |
| n(%) | n(%) | n(%) | n(%) | ||
| Socio-economic characteristics | |||||
| Mean maternal age(SD) | 23.4(5.0) | 23.7(5.3) | 23.7(4.4) | 23.6(4.9) | 0.664 |
| Marital status | |||||
| Married | 80(90.9) | 74(90.2) | 74(93.7) | 228(91.6) | 0.709 |
| Single | 8(9.1) | 8(9.8) | 5(6.3) | 21(8.4) | |
| Median Household-size(Range) | 4.0(1-8) | 4.0(2-10) | 4.0(2-9) | 4.0(1-10) | 0.625 |
| Mother’s level of education | |||||
| No School | 3(3.4) | 2(2.4) | 0(0) | 5(2.0) | 0.667 |
| Primary | 75(85.2) | 68(82.9) | 66(83.5) | 209(83.9) | |
| Secondary | 7(8.0) | 9(11.0) | 11(13.9) | 27(10.8) | |
| College/University | 3(3.4) | 3(3.7) | 2(2.5) | 8(3.2) | |
| House ownership type | |||||
| Owned | 72(81.8) | 63(76.8) | 60(75.9) | 195(78.3) | 0.606 |
| Rented | 16(18.2) | 19(23.2) | 19(24.1) | 54(21.7) | |
| Household Assets | |||||
| Radio | 58(65.9) | 66(80.5) | 52(65.8) | 176(70.7) | 0.059 |
| Television | 13(14.8) | 23(28) | 21(26.6) | 57(22.9) | 0.077 |
| Phone | 67(76.1) | 62(75.6) | 67(84.8) | 196(78.7) | 0.276 |
| Car | 2(2.3) | 1(1.2) | 0(0) | 3(1.2) | 0.776 |
| Motorcycle | 5(5.7) | 6(7.3) | 6(7.6) | 17(6.8) | 0.867 |
| Mean land acreage | 1.2(1) | 1.1(1) | 1(0.8) | 1.1(0.9) | 0.845 |
| Median land acreage | 1(0.2-5) | 1(0.1-5) | 0.8(0.1-4) | 1(0.1-5) | 0.566 |
| Mean number cows | 2(2.1) | 2(1) | 1.5(0.8) | 1.8(1.3) | 0.166 |
| Median number cows | 2(1-12) | 2(1-4) | 2(1-4) | 2(1-12) | 0.301 |
| House Rent (Kshs.) | |||||
| Mean | 921.4(588.6) | 1326.3(983.1) | 1417.6(561.5) | 1244(769.9) | 0.142 |
| Median rent in KShs.(Range) | 500(400-2000) | 1500(300-4000) | 1500(500-2500) | 1500(300-4000) | 0.288 |
KShs=Kenya Shillings (1 US Dollar=Ksh 85 in 2013); Chi-sq=Chi-Square test; KW=Kruskal Wallis test; N= Total number; n=frequency
Impact of the Interventions on the Cross-Sectional Exclusive Breastfeeding Rates
At first month postpartum, significantly higher proportion of mothers in MESIGA exclusively breastfed their infants compared to CG [{RR=2.1; CI (1.48-2.89) p=<0.001}, {RR=1.94; CI (1.38-2.73); p<0.001}] respectively. Infants in MESIGA were more likely to be exclusively breastfeed compared to infants in MES {RR=1.07 CI (0.96-1.18); p=0.232} but the difference was not significant (Table 2). At the second month, the percentages of infants who were exclusively breastfed in the three groups dropped (Table 2). Mothers in MESIGA and MES were significantly more likely to exclusively breastfeed than mothers in CG. There was no significant difference in EBF rates between MESIGA and MES {RR=1.09; CI (0.91-1.3); p=0.343}. Similar trends were observed at the third and fourth months after delivery (Table 2).
Likewise, at the fifth month after delivery, significantly higher percentages of infants in MESIGA and MES were exclusively breastfed than in CG but no significant difference in the EBF rates was observed between MESIGA and MES (Table 2). At the sixth month same trend was observed. Compared to mothers in CG, mothers in MESIGA were significantly 2.0 times more likely to exclusively breastfeed {RR=2.42; CI (1.36-4.28); p=0.0004}. Similarly, infants in MES were significantly 2.0 times more likely to be exclusively breastfed than those in CG {(RR=1.89; CI (1.02-3.49); p=0.033}. There was no significant difference observed in EBF rates between MESIGA and MES groups {RR= 1.28 CI (0.9-1.83); (p=0.174)} (Table 2).
Table 2: Impact of the interventions on the cross-sectional exclusive breastfeeding rates.
| Month | EBF status | Study groups | p-value | Ref=CGMESIGA vs CGRR;(95%CI) | p-value | Ref=CGMES vs CGRR;95%CI | p-value | Ref=MESMESIGA vs MESRR;95%CI | p-value | ||||
| MESIGA N=73 n(%) | MES N=50 n(%) | CG N=41 n(%) | |||||||||||
| 1 | EBF | 70(95.9) | 45(90) | 19(46.3) | <0.001 | 2.1(1.48-2.89) | <0.001 | 1.94(1.38-2.73) | <0.001 | 1.07(0.96-1.18) | 0.232 | ||
| Non- EBF | 3(4.1) | 5(10) | 22(53.7) | ||||||||||
| 2 | EBF | 62(84.9) | 39(78) | 14(34.1) | <0.001 | 2.5(1.61-3.85) | <0.001 | 2.28(1.46-3.58) | <0.001 | 1.09(0.91-1.3) | 0.343 | ||
| Non- EBF | 11(15.1) | 11(22) | 27(65.9) | ||||||||||
| 3 | EBF | 53(72.6) | 33(66) | 13(31.7) | <0.001 | 2.3(1.43-3.67) | <0.001 | 2.08(1.27-3.4) | 0.001 | 1.1(0.86-1.4) | 0.443 | ||
| Non- EBF | 20(27.4) | 17(34) | 28(68.3) | ||||||||||
| 4 | EBF | 53(72.6) | 33(66) | 11(26.8) | <0.001 | 2.71(1.6-4.57) | <0.001 | 2.46(1.43-4.23) | 0.002 | 1.1(0.86-1.4) | 0.443 | ||
| Non- EBF | 20(27.4) | 17(34) | 30(73.2) | ||||||||||
| 5 | EBF | 45(61.6) | 32(64) | 10(24.4) | 0.001 | 2.53(1.43-4.46) | 0.001 | 2.62(1.47-4.68) | 0.002 | 0.96(0.73-1.3) | 0.790 | ||
| Non-EBF | 28(38.4) | 18(36) | 31(75.6) | ||||||||||
| 6 | EBF | 43(58.9) | 23(46) | 10(24.4) | 0.002 | 2.42 (1.36-4.28) | 0.004 | 1.89(1.02-3.49) | 0.033 | 1.28(0.9-1.83) | 0.174 | ||
| Non- EBF | 30(41.1) | 27(54) | 31(75.6) | ||||||||||
EBF= Exclusive Breastfeeding; Non-EBF=Non-Exclusive Breastfeeding
Impact of the Interventions on the Duration of Cumulative Exclusive Breastfeeding
Mothers in CG cumulatively exclusively breastfed their infants for a shorter period compared to mothers in the two treatment groups. The mean duration of cumulative exclusive breastfeeding was significantly shorter at 0.7(±0.15) months in the CG compared to the mean duration of cumulative exclusive breastfeeding for mothers in the MES (2.8 months) and MESIGA (3.4 months) (Table 3). No infants were cumulatively exclusively breastfed for six months in CG. A higher proportion of mothers in MESIGA (27%) compared to MES (10%) cumulatively exclusively breastfed for six months. Kaplan-Meir Survival analysis was used to determine cumulative exclusive breastfeeding among the three study groups (Figure 2).
Table 3: Mean and median months of cumulative EBF by study group.
| Study groups | N | Mean (SD) | Median (range) | Proportion cumulative EBFat 6months | Wilcoxon p-value |
| MESIGA | 73 | 3.4(0.2) | 4.0(2-5) | 27.4% | <0.001** |
| MES | 50 | 2.8(0.24) | 2.5(2-4) | 10.0% | |
| CG | 41 | 0.7(0.15) | 0 (0-1) | 0.0% |
**Significant Association (p<0.001)
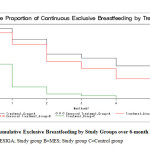 |
Figure 2: Cumulative Exclusive Breastfeeding by Study Groups over 6-month Period |
Discussion
Few scientific studies have been carried out globally to test the impact of MTMSGs in the promotion of EBF. The current study was the first to utilise the randomized trial design to assess the impact of MTMSGs with and without IGAs in promoting exclusive breastfeeding in Kenya. The MTMSGs strategy had a significantly positive impact in promoting EBF rates throughout the 6 months period of intervention. Compared to the control group, the two intervention groups (MESIGA and MES) significantly improved the exclusive breastfeeding rates throughout the sixth-month period. Notably, there were no significant differences in the impact of the two MTMSGs intervention strategies in promoting EBF and therefore both strategies can be considered in the promotion of EBF.
The cross-sectional EBF rate at 6 months was significantly higher in the intervention groups; MES at 46% and MESIGA at 58.9% compared to CG at 24%. The EBF rates reported in the current study were higher compared to a similar study on MTMSG carried out in Guatemala by Dearden et al. (28) where the rate in the intervention group was 45% at 6 months after delivery. In 1999, a trial intervention (28) was started in two program areas and two non-program (control) areas in Guatemala. Their targets were both pregnant and lactating mothers in the study area unlike in the Kenyan (this) study where all participants in the two intervention groups as well as the control group were recruited during their third trimester of pregnancy. Mothers in the latter study had prolonged contact time with their peers and facilitator through the MTMSGs. This could be one of the explanations for the difference in findings. At baseline in Guatemala, the two intervention groups had existing MTMSGs which were not active while the control groups had none. In case of the Kenyan study, all intervention and control groups were established in areas where there were no MTMSGs.29
Results from Guatemalan study showed that MTMSGs had impact on exclusive breastfeeding at six months post delivery while in the Kenyan study; the MTMSG intervention had impact on EBF at every month, for six months post delivery. It is important to note that in the Kenyan study, data was collected on a monthly basis while in the Guatemalan study, the data was collected at baseline and at the end of the study (6 months postpartum) hence there was more contact with the mothers in the Kenyan study. Increased contact with the mothers may have led to positive modification of responses hence increased rates of exclusive breastfeeding.17
Currently, in Kenya, there are no clear guidelines for hospital discharge of the mothers to the community-based groups as well as health care support for the mothers who enrol in the community-based groups. During the present study, mothers were referred for recruitment in the MTMSGs by mothers who were already members or by the health facility nurses. This was one of the limitations of the current study since mothers who did not attend health facility or never got into contact with any of the MTMSG members could not be recruited. Secondly, members of the MTMSGs with medical problems which affected breastfeeding were referred by the research team to the nearest health facility for treatment. The study team did not collect data on the types of treatment offered nor the results of the treatment since this was not an objective of the study. Finally, the control group, like the two intervention groups, had seven monthly contacts with the study team for data collection which may have positively influenced their responses on EBF. Similar number of interviews for control group and the intervention groups were necessary due to the need to collect monthly data on mothers’ challenges in breastfeeding for comparison to those in the intervention groups on monthly basis.
Recent studies on the promotion of exclusive breastfeeding using community-based interventions have demonstrated significant positive impact on rates and duration of exclusive breastfeeding.15, 17, 18, 19, 28 and 29 A recent community-based study conducted in Uganda15 demonstrated that EBF promotion in sub-Saharan Africa is feasible and can be implemented at sustainable cost using community-based models. However, it is important to note that the above studies did not use the MTMSG approach as was the case in the current study.
The current study findings provide further scientific evidence for the implementation and strengthening of community-based strategies for promoting exclusive breastfeeding. The study findings will further support the already existing initiatives in the promotion of breastfeeding such as the Baby-Friendly Hospital Initiative (BFHI) by UNICEF and WHO27 and community-based strategies.17 The Kenya Ministry of Health in conjunction with African Population Health Research Centre (APHRC) has also implemented the Baby Friendly Community Initiative and is undertaking a randomized control study to test its impact at promoting infant and young feeding practices at the community level but the impact of this intervention on EBF of this study are yet to be published.30
Conclusions
The MTMSGs had significant positive influence in promoting EBF rates throughout the 6 months period of intervention. This shows that both MTMSG strategies (MES and MESIGA) were effective in increasing the rates of EBF in a low socio-economic rural set up. Notably, there was no significant difference in the impact of the two MTMSG intervention strategies in promoting EBF and therefore both strategies can be considered in the promotion of EBF. Despite the continued support offered to mothers throughout the seven months period; only a modest proportion of mothers exclusively breastfeed their infants continuously until the recommended six months. This shows that there is need to find new ways to increase support to mothers in order to improve the EBF rates to WHO recommendations. It is recommended that further MTMG studies be carried out in different socio-economic environments to determine their feasibility and impact under different contexts.
Acknowledgements
This study was supported by the National Council of Science and Innovation- Kenya, but the funder had no input or influence on the conception, design or implementation of the trial or in the writing of this manuscript.
Conflict of Interest
Source of funding: This study was supported by the National Council of Science and Innovation- Kenya, but the funder had no input or influence on the conception, design or implementation of the trial or in the writing of this manuscript. The authors declare no conflict of interest.
References
- Tylleskär T., Jackson, D., Meda, N., Engebretsen, I. M. S., Chopra, M., & Diallo, A. H. PROMISE-EBF Study Group. Exclusive breastfeeding promotion by peer counsellors in Sub-Saharan Africa (PROMISE-EBF): a cluster-randomised trial. 2011; 378 (9789), 420–427.
- Mother-to-Mother Support for Breast-Feeding: Frequently Asked Questions. Academy for Educational Development, Washington, D.C. 2004; www.Linkagesproject.Org Accessed On 20th November 2011.
- WHO/UNICEF. Baby-Friendly Hospital Initiative Revised, Updated and Expanded For Integrated Care. World Health Organisation, Geneva, Switzerland. 2009.
- Kenya National Bureau of Statistics (KNBS) & ICF Macro. Kenya Demographic and Health Survey 2008-9, Calverton Maryland: KNBS and ICF Macro. 2010.
- Kenya National Bureau of Statistics (KNBS) & ICF Macro. Kenya Demographic and Health Survey2014, Calverton Maryland: KNBS and ICF Macro. 2014.
- UNICEF. The State of the World’s Children. United Nations Children’s Fund. New York, USA. 2016.
- Every Child Counts: revealing disparities, advancing children’s rights. United Nations Children’s Fund. New York, USA. 2014.
- Statement from the World Health Organization on exclusive breast-feeding. World Health Organization. Geneva, Switzerland. 2014.
- Lauer J. A., Betra´n A. P., Barros A. J. D., et al.. Deaths and years of life lost due to sub-optimal breast-feeding among children in the Developing World: A Global Ecological Risk Assessment. Public Health Nutrition. 9(6), 673–685.
- Brown A., Paynor P. & Lee M. Healthcare professionals’ and mothers’ perceptions of factors that influence decisions to breastfeed or formula feed infants: A Comparative Study. Journal of Advanced Nursing. 2011; Sep; 67(9):1993-2003.
- Singhal A. & Lanigan J. Breast-feeding, Early Growth and Later Obesity Childhood Nutrition Research Centre. 2006. Institute of Child Health. London, UK.
- The State of the World’s Children. United Nations Children’s Fund. New York, USA. 2014.
- National Institute of Statistics, Directorate General for Health, and ICF Marco. Cambodia Demographic and Health Survey 2010. Phnom Penh, Cambodia and Calverton, Maryland, USA: National Institute of Statistics, Directorate General for Health, and ICF Marco. 2011.
- Ochola S.A., Labadarios D., Nduati R.W. Impact of counselling on exclusive breast-feeding practices in a poor urban setting in Kenya: a randomized controlled trial. Public Health Nutr. 2012; Oct 8:1-9. Doi: 10.1017/S1368980012004405 4.
- Irene Awuor Ogada. Effectiveness of couple counselling versus maternal counselling in promoting exclusive breast feeding: a randomised controlled trial in Nyando District, Kenya. Doctoral thesis, Kenyatta University, Kenya. 2014.
- Muruka C. & Ekisa H. A Case Study on the Impact of Mother-to-Mother Support Groups on Maternal, Infant and Young Child Nutrition and Care Practices in Habaswein and Wajir South Districts of North Eastern Kenya Food and Nutrition Sciences. 2013; 4, 31-35.
- Child Y. Infant and Young Child Feeding. Nutrition. 2011. Retrieved: http://www.unicef.org/aids/files/hiv_IYCF_programmingguide_2011.pdf
- Kenya National Bureau of Statistics. Meru North District Multiple Indicator Cluster Survey 2008, Nairobi, Kenya. Kenya National Bureau of Statistics. 2009.
- Schulz K. F., Altman D. G. & Moher D. CONSORT 2010 Statement: Updated Guidelines for Reporting Parallel Group Randomized Trials. British Medical Journal. 2010.
- Kelsey J. L., Whittemore A. S. & Evans A. S. Methods in Observational Epidemiology. Oxford University Press, 1996.
- Fleiss J.L. Statistical methods for rates and proportions. John Wiley & Sons. 1997.
- PATH/UNICEF. Mother-to-mother Support Groups Facilitators’ Manual with Discussion Guide. http://iycn.wpengine.netdna-cdn.com/files/IYCN_Mother-to-Mother-Support-Group-Facilitator-Manual. 2011; pdf
- Cogill B. Anthropometric Indicators Measurement Guide. Food and Nutrition Technical Assistance Project, Academy for Educational Development, Washington, D.C. 2003.
- WHO/UNICEF. World Health Organization, Geneva, Switzerland. 2008. http://whqlibdoc.who.int/publications/2008/9789241596596_eng.pdf?ua=1.
- M’liria J. K. Effectiveness of mother-to-mother-support groups in promoting exclusive breastfeeding in Igembe South Sub-county, Meru County, Kenya: a randomized controlled trial. Doctoral thesis, Kenyatta University, Kenya. 2015.
- Masibo P., Kimani-Murage E., Wekesah F., et al. “Establishing innovative community engagement approaches in Baby Friendly Community Initiatives Project”, a public engagement project by APHRC in Collaboration with the Unit of Nutrition and Dietetics, Ministry of Health, Kenya. 2014.
Accepted on: 14/04/2020
Second Review by: Monica Romania
Final Approval by: Suhad Maatoug Bahijri





Web of Science Coverage
Emerging Sources Citation Index (ESCI)
2024 Journal Impact Factor: 1.1
Scopus Journal Metrics
CiteScore 2025: 2.6
CiteScore Details
Sustainable Nutrition: Food Systems, Nutrient Retention, and Public Health Impact
![]()
This journal is a member of, and subscribes to the principles of, the Committee on Publication Ethics (COPE)








