Relationship Between Clinical Indicators of Periodontal Disease and Serum Level of Vitamin D
Dong-Eun Lee1*
1Department of Dental Hygiene, Ulsan College, Ulsan, 44022, South Korea
2Department of Occupational Therapy, Semyung University, Chung-buk, 27136, South Korea
Corresponding Author Email: apolius@naver.com
DOI : http://dx.doi.org/10.12944/CRNFSJ.7.1.04
Download this article as:
![]()
Background: Vitamin D is obtained through food and nutritional supplements, or is synthesized in the skin by sunshine. It is then transferred to the liver and kidney through the bloodstream and hydroxylated by a specific enzyme (cytochrome P450 family 27 subfamilies A member 1, cytochrome P450 family 27 subfamily B member 1) to form 25-hydroxyvitamin D and 1,25-dihydroxy vitamin D. The vitamin D synthesis facilitates calcium and phosphorus absorption from the intestines. The parathyroid hormone helps to synthesize 1,25-dihydroxy vitamin D to aid calcium absorption. Objectives: Many researchers have investigated the relationship between serum vitamin D levels and periodontal disease. And periodontal disease indicators such as bleeding on probing, pocket depth, clinical attachment level, gingival index, and cementoenamel junction-alveolar cresthave been used to identify the effects of vitamin D on periodontal disease. The effects of vitamin D on bacteria or cytokines have also been investigated. In this review article, vitamin D levels according to the status of periodontal disease were summarized. Data sources: PubMed was searched electronically, and randomized clinical trials, cross-sectional studies, and case-control studies were included in the review. Study appraisal and synthesis methods: Articles that the classification of periodontitis was accurately described, indicators for identifying periodontitis was clearly marked, and the form of vitamin D measured in the study was accurately described were selected. Only highly relevant journals were selected and summarized. Results: Most of the research has found positive associations between the serum 25-hydroxyvitamin D level and periodontal health, and the clinical parameters of periodontal disease were reduced by vitamin D. Limitations: Detailed categorization of the characteristics associated with the 25-hydroxyvitamin D level should be needed in future studies. Conclusions: This review article can be used as a guide by clinicians and as a reference book for patients’ education.
KEYWORDS:Periodontal Disease; Vitamin D
Introduction
Vitamin D is obtained through food and nutritional supplements or is synthesized in the skin from theUV-B radiated by sunshine. It is then transferred to the liver through the bloodstream, where it is hydroxylated by 25-hydroxylase to form 25(OH)D (calcidiol, calcifediol). As 25(OH)Disa fairly stable compound in the human body, it is commonly used as an indicator of the blood vitamin D concentration. The 25(OH)D is then transferred to the kidneys, where it undergoes another hydroxylation by 1α-hydroxylase to form 1,25(OH)2D (calcitriol), a biologically active form of vitamin D. The vitamin D synthesis facilitates calcium and phosphorus absorption from the intestines to maintain the serum concentrations within normal ranges. If the calcium levels decrease, the parathyroid hormone (PTH) helps to synthesize 1,25(OH)2D to aid calcium absorption [Figure 1].1
As individuals’ bone mass increases and decreases over their lifetime, calcium is necessary to maintain bone balance. When the bone balance is disrupted, diseases associated with the skeletal bone—such as periodontitis—occur. Therefore, calcium intake is important. However, there are thresholds of calcium utilization even when the calcium intake increases. When calcium levels are too low, the skeletal calcium is resorbed to maintain the body’s calcium homeostasis. This mechanism is mediated by the PTH and vitamin D. Therefore, vitamin D hormones essential to the human body to maintain a healthy and normal condition[Figure 1].1
Sufficient vitamin D level is necessary for the maintenance of periodontal health,2 and intake of vitamin D can decrease the gingivitis and chronic periodontitis.3 Because vitamin D has an anti-bacterial and anti-inflammatory effect,4 and it also has anti-proliferative effects and initiates cell apoptosis. In addition, vitamin D is also important for bone metabolism, alveolar bone resorption and preventing tooth loss.3
The Food and Nutrition Board (FNB) have issued guidelines on the recommended dietary allowances (RDA) for healthy vitamin D concentrations.5 The RDA for vitamin D is as follows 400 IU between 0 and 12 months of age, 600 IU between 1 and 70 years old, and 800 IU after 70 years old. These quantities do not differ between men and women. The serum 25(OH) D concentration can be used as a vitamin D indicator. Less than 12 ng/ml indicates a deficiency, 12-20 ng/ml is an inadequate level, more than 20 ng/ml is an adequate level for bone and overall health, and more than 50 ng/ml signals potential adverse effects from vitamin D in individuals. The Institute of Medicine also concluded that for maximum bone health, a serum 25(OH)D level over 20 ng/ml was adequate.6 In the Endocrine Society’s Practice Guidelines (ESPG) on vitamin D, the deficiency was defined as 25(OH)D<20 ng/ml, insufficiency as 21-29 ng/ml, and sufficiency as at least 30 ng/ml for maximum bone health.7 These criteria are also accepted by the National Osteoporosis Foundation, the International Osteoporosis Foundation, the American Association for Clinical Endocrinologists, and the American Geriatric Society.8, 9
However, establishing an RDA for vitamin D is difficult, as it is synthesized from sunshine and the intake depends on the individual’s lifestyle. The country of residence and the seasons can affect vitamin D synthesis, as they entail different levels of exposure to sunshine. Holick reported that people who live close to the equator and Puerto Rican farmers have high 25(OH)D concentrations.10 Zittermann reviewed the vitamin D status of European populations in summer and winter. The results suggested that vitamin D levels were higher in summer than in winter.11
Many researchers have investigated the relationship between serum vitamin D levels and periodontal disease, and periodontal disease indicators such as the bleeding on probing (BOP),12-14 pocket depth (PD),12, 13, 15-21 clinical attachment level (CAL),13, 14, 16- 21 gingival index (GI),13-16 and cementoenamel junction-alveolar crest (CEJ-AC)13, 14 have been used to identify the effects of vitamin D on periodontal disease[Figure 2]. The effects of vitamin D on bacteria or cytokines have also been investigated.
 |
Figure 1 Click here to View figure |
Vitamin D is obtained through food and supplements or is synthesized in the skin by sunshine. It is then transferred to the liver and kidney through the bloodstream and hydroxylated by specific enzyme (CYP27A1, CYP27B1) to form 25(OH)D and 1,25(OH)2D. The vitamin D synthesis facilitates calcium and phosphorus absorption from the intestines and the PTH helps to synthesize 1,25(OH)2D to aid calcium absorption. Also, 25(OH)D and 1,25(OH)2D can be synthesized by GF and PDL cells to inhibits pro-inflammatory cytokines such as IL-6 and IL-8 produced by Pg-LPS.
T, tooth; GF, gingival fibroblast; PDL, periodontal ligament; GCF, gingival crevicular fluid; IL, interleukin;
PTH, parathyroid hormone; LPS, lipopolysaccharide; TLR, toll-like receptor; Pg, Porphyromonasgingivalis;
Most previous studies have focused on one of the different forms of periodontal disease and suggested a correlation with vitamin D levels.12-21 However, periodontal disease is a progressive disease that can be gradually aggravated by personal habits. Therefore, it is important to understand its overall flow. To this end, this study collected and analyzed data to identify the vitamin D levels for each periodontal disease classification, so as to provide clear information to clinicians and researchers.
Materials and Methods
PubMed (MEDLINE) was searched electronically, and randomized clinical trials, cross-sectional studies, and case-control studies were included in the review. The following terms and combinations were used to search the database:
“gingivitis AND vitamin D”; “gingivitis AND calciferol”;“chronic periodontitis AND vitamin D”; “chronic periodontitis AND calciferol”; “aggressive periodontitis AND vitamin D”; “aggressive periodontitis AND calciferol”; “bleeding on probing AND vitamin D”; “bleeding on probing AND calciferol”; “pocket depth AND vitamin D”; “pocket depth AND calciferol”; “clinical attachment level AND vitamin D”; “clinical attachment level AND calciferol”; “gingival index AND vitamin D”; “gingival index AND calciferol”; “cementoenamel junction-alveolar crest AND vitamin D”; “cementoenamel junction-alveolar crest AND calciferol”;“vitamin D AND review”; “periodontal disease AND review”;
Among 194 articles, 29 papers were finally selected. Articles that the classification of periodontitis was accurately described, indicators for identifying periodontitis was clearly marked, and the form of vitamin D measured in the study was accurately described were selected. To remove the author’s prejudice and convey accurate information, negative correlation results between periodontitis and vitamin D were also selected.
Non-English language studies and those with unavailable full text or unpublished data were excluded. Only highly relevant journals were selected after reading their abstracts.
Results
Vitamin D concentration and periodontal disease
Periodontitis is a chronic inflammatory disease caused by bacteria; whose severity can be affected by cytokines and osteoclasts.22 The American Academy of Periodontology (AAP) criteria are widely used to classify the disease.23 Researchers who study the vitamin D levels in relation to the periodontal disease commonly focus on three categories from the AAP’s classification: gingivitis, chronic periodontitis, and aggressive periodontitis [Table 1].
Table 1: Vitamin D and periodontal disease
| Reference | Type and population | Vitamin Danalysis | concentration of 25(OH)D in serum | Oralstatus | Standard of oral condition | Sites | Clinical parameters | Results | ||||||
| ng/ml | nmol/L | CAL (mm) | PD (mm) | |||||||||||
| HiremathVPet al. (11) | RCTn=96Clinics | Oral supp.(2000 IU/day1000 IU/day
500 IU/day placebo) |
First visit | Final visit | First visit | Final visit | G | Ns. | <3 | GI* | Dose dependentanti-inflammatory effect ofvitamin D
on gingivitis. |
|||
| 22.5±7.026.8±0.724.0±5.1
28.2±3.1 |
52.2±10.2*43.7±8.8*36.8±6.1*
28.5±4.0 |
56.1±17.566.9±1.859.9±12.7
70.3±7.7 |
130.3±25.5*109.0±22.0*91.9±15.2*
71.2±10.0 |
|||||||||||
| Dietrich Tet al. (12) | CSn=6,700NHANESIII | 25(OH)Din serum | 12.5±2.619.2±1.524.4±1.6
30.4±2.0 42.5±8.5 |
31.3±6.647.8±3.860.8±3.9
75.8±4.9 106.0±21.1 |
G | Ns. | MB | BOP* | Positive association between 25(OH)D and periodontal health | |||||
| Miley DDet al. (13) | CSn=51Clinics | Oral supp.≥400 IU/day(+Ca≥1,000 mg/day) | Ns. | Ns. | CP | ≥3(↑2 ip) | Ns. | All | BOP, PD, CAL, GI, CEJ-AC | Borderline statistically significant | ||||
| – Received periodontal maintenance programs | ||||||||||||||
| Garcia MNet al. (14) | Cohortn=51Clinics | Oral supp.≥400 IU/day(+Ca≥1,000 mg/day) | Ns. | Ns. | CP | ≥3(↑2 ip) | Ns. | All | BOP*CAL*GI*
CEJ-AC |
Positive association betweenoral supp. (vitamin D with Ca) and periodontal health | ||||
| – Received periodontal maintenance programs | ||||||||||||||
| Perayil Jet al. (15) | RCTn=77Clinics | Oral supp.≥250 IU/day(+Ca≥500 mg/day) | First visit | 3 months | First visit | 3 months | CP | 3-4(↑1 t) | Ns. | All | PD*CAL*GI* | Positive association betweenoral supp. (vitamin D with Ca) and periodontal health | ||
| (T) 26.0±1.3(N) 25.5±0.2 | (T) 36.0±1.2*(N) 25.6±0.2 | (T) 64.9±3.2(N) 63.7±0.5 | (T) 89.9±3.0*(N) 63.9±0.5 | – Received SRP and curettage | ||||||||||
| Abreu OJet al. (16) | CC, CSn=38Clinics | 25(OH)Din serum | (P) 18.5±4.6*(C) 24.2±7.1 | (P) 46.2±11.5*(C) 60.4±17.7 | MPSP | (MP)≥4(↑2 ip) | (MP)≥5(↑2 ip) | All | PD*CAL* | Positive association between 25(OH)D and periodontal health | ||||
| (SP)≥6(↑2 ip) | (SP)≥5(↑1 ip) | |||||||||||||
| Laky Met al. (17) | CCn=58 | 25(OH)Din serum | (P) 26.0±15.8*(C) 34.9±15.6 | (P) 65.0±39.3*(C) 87.1±39.0 | SP | Ns. | ≥5(↑2 t) | All | PDCAL | Positive association between 25(OH)D and periodontal health | ||||
| AdegboyeARet al. (18) | CSn=3287 | Oral supp.(Ca, vitamin D, casein) | Ns. | Ns. | SP | ≥6(↑2 ip) | ≥5(↑1 ip) | B | CAL | Intake of vitamin D alone was not associated severe periodontitis. | ||||
RCT, randomised clinical trial; CS, cross-sectional study; CC, case-control; NHANESIII, third National Health and Nutrition Examination Survey; Oral supp., oral supplementation;
Ca, calcium; Ns., not suggested; T, taker group; N, non-taker group; P, periodontitis; C, control; CAL, clinical attachment loss; PD, pocket depth; ↑, at least; ip, interproximal; t, teeth;
B, buccal; L, lingual; MB, mesio-buccal; ML, mesio-lingual; DB, disto-buccal; DL, disto-lingual; All, include 6 sites on the teeth (B, L, MB, ML, DB, DL);
GI, gingival index; BOP, bleeding on probing; CEJ-AC, cementoenamel junction-alveolar crest; G, gingivitis; CP, chronic periodontitis; MP, moderate periodontitis; SP, severe periodontitis;
SRP, scaling and root planning;
*Significant differences compared to placebo or control group.
Table 2: Vitamin D and bacterial species or biochemical parameters
| Reference | Type and population | Vitamin Danalysis | Concentration of 25(OH)D in serum | Oralstatus |
Standard of oral condition |
Results | |||
| CAL (mm) | PD (mm) | ||||||||
| ng/ml | nmol/L | ||||||||
| Teles FRet al. (20) | Cohortn=56Clinic | 25(OH)Din serum | 29.8$ | 74.38$ | CP | Ns. | <2.8 | – Red complex:Tannerella forsythia*Porphyromonasgingivalis*Treponemadenticola*- Orange complex:
Prevotellanigrescens Eubacteriumnodatum |
|
| 25.2$ | 62.90$ | Ns. | <3.4 | ||||||
| 25$ | 62.40$ | Ns. | ≥3.4 | ||||||
| Liu Ket al. (21) | Cohortn=178Clinic | 25(OH)Din serum | (AgP) 11.7±6.9* | (AgP) 29.3±17.2* | AgP | Ns. | >6 (↑8 t) | OC | 0.90* |
| ALP | 60.2±18.2 | ||||||||
| (CP) 10.2±5.7 | (CP) 25.5±14.3 | CP | ≥1 (↑2 ip) | ≥5 (↑2 ip) | OC | 0.70 | |||
| ALP | 63.1±24.4 | ||||||||
| (C) 8.7±5.8 | (C) 21.6±14.4 | C | ≤3 | ≤3 | OC | 0.70 | |||
| ALP | 64.1±16.6 | ||||||||
| Liu Ket al. (22) | Cohortn=19Clinic | 25(OH)Din serum | (First visit) 11.7±2.0 | (First visit) 29.3±4.9 | AgP | Ns. | >6 (↑8 t) | OC | 1.03±0.46 |
| IL-1β | 6.71 | ||||||||
| IL-6 | 1.00 | ||||||||
| (2 months) 9.0±1.6* | (2 months) 22.5±3.9* | OC | 1.01±0.37 | ||||||
| IL-1β | 3.23* | ||||||||
| IL-6 | 1.06 | ||||||||
| 25(OH)Din GCF | (First visit) 3,584.5 | (First visit) 8,946.8 | – Received periodontal therapy (TBI and SRP) | OC | 109 | ||||
| IL-1β | 10,592 | ||||||||
| IL-6 | 3,798 | ||||||||
| (2 months) 2,265.8* | (2 months) 5,655.3* | OC | 81 | ||||||
| IL-1β | 5,499* | ||||||||
| IL-6 | 3,730 | ||||||||
| (6 months) 1,380.1* | (6 months) 3,444.8* | OC | 98 | ||||||
| IL-1β | 3,963* | ||||||||
| IL-6 | 4,531 | ||||||||
AgP. aggressive periodontitis; CP, chronic periodontitis; C, control; CAL, clinical attachment loss; PD, pocket depth; Ns., not suggested; ↑, at least; ip, interproximal; t, teeth;
TBI, tooth brushing instruction; SRP, scaling and root planning; OC, osteocalcin; ALP, alkine phosphatase; IL, interleukin; GCF, gingival crevicular fluid;
$ Mesian value
* Significant differences compared to control or first visit group.
** Significantly correlated
The standards for gingivitis weresetasPocket Depth(PD)<315 or not suggested.12 Subjects were recruited in India from June 2010, and they underwent post-recruitment follow-up from February to May 2011. The 25(OH)D concentrations (ng/ml) rose from 22.5±7.0 to 52.2±10.2, 26.8±0.7 to 43.7±8.8, and 24.0±5.1 to 36.8±6.1 after 2000, 1000, and 500 IU/day of vitamin D oral supplementation for 3 months, respectively. All the groups had an adequate vitamin D status according to the FNB’sRDAson their first visit, and the 25(OH)D concentrations increased with the doses of vitamin D. It was particularly highly increased in the group that received a2000 IU dose of vitamin Doral supplementation, and the 25(OH)D concentration was involved in the vitamin D adverse effect group of individuals that showed potential adverse effects. However, according to the ESPG, all the groups had an insufficiency vitamin D status on their first visit and sufficiency vitamin D status on their final visit. And, it has a significant anti-inflammatory effect on the gingival according to the concentrations.15Although the vitamin DRDAs for adults are600 IU, tolerable upper intake levels were found to be 4000 IU (data not shown,8). Therefore, the subjects may not have had health problems. Another team assayed the serum 25(OH)D concentrations in white volunteers in the midwestern United States in October. They divided the subjects into five groups according to their 25(OH)D concentrations (quintile, nmol/l): (1)31.3±6.6, (2) 47.8±3.8, (3) 60.8±3.9, (4) 75.8±4.9, (5) 106.0±21.1. The quintile (1) and (2) groups had inadequate vitamin D levels, while the(3)-(5) groups had adequate vitamin D levels according to the FNB’s RDAs.12 In gingivitis, the serum 25(OH)D levels were linked to an inadequate or adequate vitamin D status. This is probably due to the mild symptoms of gingivitis.
The standards for moderate to severe chronic periodontitis were set as CAL≥3,13, 14withthe PD not suggested.13, 14, 16 In a study, the subjects followed periodontal maintenance programs during the course of the research.13, 14, 16 They were recruited between June 2007 and February 2008,13 and took vitamin D (≥400 IU/day) and calcium (≥1000 mg/day) for >18 months (Taker group) or not (Non-Taker group).13-14 In another study, subjects were recruited inIndiabetweenNovember 2012 and December 2013 and took vitamin D (≥250 IU/day) and calcium (≥500 mg/day) for 3 months (Taker group) or not (Non-Taker group).16 The vitamin D dose was capped based on the FNB’s RDAs on the final visit.13, 14, 16 However, the concentration of 25(OH)D (ng/ml) in the serum increased from 26.0±1.3 to 36.0±1.2 (p=0.001).16 In the chronic periodontitis group, the level of 25 (OH)D in the serum was adequate before and after the therapy and the oral supplementation, but the 25(OH)D level was increased after the therapy and supplementation.16
The standards for moderate and severe periodontitis were set as CAL≥4 and PD≥5, and CAL≥6 and PD≥5, respectively.17-19 In a study of Hispanic adults, the 25(OH) D concentration (ng/ml) was 18.5±4.6 in the periodontitis group and 24.2±7.1 in the healthy control group (p=0.006).17 The periodontitis group had an inadequate vitamin D status, while the healthy control group had adequate vitamin D levels according to the FNB’s RDAs. In this study, the vitamin D status categories (≤12: deficient, 12-19: inadequate, 20-30: adequate, >30: optimal)differed from those defined by the FNB. The adequate group was further divided into adequate and optimal groups.17 In periodontitis group, 63.2% of the subjects had inadequate levels, and 36.8% had adequate levels. In the healthy control group, 31.6% had inadequate levels, 47.4% had adequate levels, and 21.1% has optimal levels of vitamin D.17Another research team recruited subjects from 2008 to 2010, and measured their 25(OH)D concentrations. The 25(OH)D concentrations(nmol/l) were 65.0±39.3 in the severe periodontitis group and 87.1±39.0 in the healthy control group (p<0.05). Both groups had adequate vitamin D levels according to the FNB’s RDAs. However, the levels were higher in the control group than in the severe periodontitis group.18Anotherstudyrecruited subjects in Denmark in 2007-2008 to study the calcium, vitamin D, casein, and whey protein levels of periodontitis patients. However, the serum 25(OH)D concentrations were not reported.19
In another study, the clinical parameters were divided into three groups (PD<2.8, <3.4, ≥3.4)and the bacterial species associated with periodontitis were investigated[24, 25]. The median of 25(OH)D concentrations(ng/ml) in the serum were 29.8, 25.2, and 25.0, respectively, showing no significant differences. All the groups had adequate vitamin D levels according to the FNB’s RDAs.
One research team set standards of PD>6 for aggressive periodontitis, and CAL≥1 and PD≥5for chronic periodontitis.20, 21 The researchers recruited subjects from July 2001 to October 2007. The subjects’ 25(OH)D concentrations (nmol/l) were29.3±17.2 in the aggressive periodontitis group, 25.5±14.3 in the chronic periodontitis group, and 21.6±14.4 in the control group, respectively. All the groups showed vitamin D deficiency according to the FNB’s RDAs.However, the 25(OH)D level was significantly higher in the aggressive periodontitis group than in the control group (p<0.05), and no significant differences were found between the aggressive periodontitis and chronic periodontitis groups or between the chronic periodontitis and control groups.20The same team recruited subjects from November 2006 to February 2007and measured their25(OH)D concentrations(nmol/l) in the serum (systemic) and in the gingival crevicular fluid (GCF, local). The subjects received periodontal therapy from baseline, and their 25(OH)D concentrations were measured at baseline, at 2 months, and at 6 months post-therapy. The serum 25(OH)D concentration was 29.3±4.9 at baseline, and it decreased to 22.5±3.9 after 2 months of therapy (p<0.05). The GCF25(OH)D concentration was 8946.8 at baseline, 5655.3 at 2 months (p<0.05), and 3444.8 at 6 months (p<0.05) after the treatment.21And these results contradicted other data [20, 21]. A possible explanation for this is that the researchers failed to consider the demographic characteristics and the latitude and seasons, habits, and lifestyle, or the exposure time sunshine and the extra vitamin D supply from the subjects’ customary diet. Therefore, researchers should consider control factors such as seasonal changes in future studies. Interestingly, the vitamin D levels were much higher in the GCF than in the serum,21 possibly because 25(OH)D and 1,25(OH)2D can be synthesized by the gingival fibroblast (GF) and periodontal ligament (PDL) cells [Figure 1].
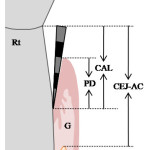 |
Figure 2 Click here to View figure |
Many researchers have investigated the relationship between serum vitamin D levels and periodontal disease, and periodontal disease indexes such as the bleeding on probing (BOP), pocket depth (PD), clinical attachment level (CAL), gingival index (GI), and cementoenamel junction-alveolar crest (CEJ-AC) have been used to identify the effects of vitamin D on periodontal disease.
AB, alveolar bone; CAL, clinical attachment level; CEJ-AC, cementoenamel junction-alveolar crest; Cr, crown
G, gingival; PD, pocket depth; Rt, the root of teeth;
Vitamin D concentration and clinical parameters
-Bleeding on probing
Bleeding on probing (BOP) is one of the symptoms of gingivitis and periodontitis.It is widely used by dental clinics a clinical parameter for oral examination and study. To evaluate the effect of vitamin D concentration on gingivitis, Dietrich et al. performed a cross-sectional study of 6,700 subjects.The authors took venous blood samples and define quintiles according to the vitamin D concentrations. They measured the proportion of bleeding in mesio-buccal teeth and calculated the P value. The bleeding proportion was 0.11±0.18 in the lowest vitamin D quintile and 0.08±0.15 in the highest quintile. The data revealed a negative association between the serum concentration of vitamin D and the bleeding proportion (p<0.001).12 Another team (Miley et al.) studied 51 subjects from clinics to identify the effect of vitamin D and calcium supplementation on chronic periodontitis. They divided the subjects into an aTaker group (intake vitamin D ≥400 IU/day with calcium ≥1,000 mg/day) and a Non-Taker group, and measured the bleeding (%) at six tooth sites (Buccal, Lingual, mesiobuccal, mesiolingual, distobuccal, Disto-Lingual). The mean of the bleeding sites was 60 in the Taker group and 66 in the Non-Taker group. The results showed no significant difference (p=0.08), but a borderline statistical significance. This study had a small population, as the researchers had difficulty finding subjects who took adequate amounts of supplementation to meet their criteria.13 The same team (Garcia et al.) reported a similar study designed to determine whether the differences persisted over a 1-year period. To this end, they measured the BOP at baseline, at 6 months, and at 12 months. The differences between the Taker and Non-Taker groups were 7.90% at baseline, 19.83% at 6 months, and 5.13%at 12 months, and the significant overtime was <0.0001 in the Taker group and 0.002 in the Non-Taker group. These results showed that intakes of calcium and vitamin D can improve periodontal health.14
-Pocket Depth
The mean pocket depth value (PD, mm) was measured by an examiner. It was 7% greater in the Non-Taker group (2.3) than in the Taker group (2.2, oral supplementation).13 In another team, the mean PD values were 6.3±0.5 at baseline, and reduce to 4.3±0.3 after 3 months in Taker group (intake vitamin D ≥250 IU/day with calcium ≥500 mg/day) (p=0.001).The data showed that vitamin D and calcium supplementation had a positive effect on the periodontal health.16 In another team, the PDs were 2.3±0.4 in the periodontitis group and 1.3±0.3 in the control group, respectively, showing statistical significance (p<0.0001).Orlando et al. also investigated that the PD value has a negative correlation with vitamin D level.This result indicates that a lower serum level of vitamin D is significantly associated with periodontitis.17 The PDs were 3.6±0.8 in the periodontitis group and 1.2±0.3 in the control group, respectively, and there was a significant difference between the periodontitis group and the control group (p<0.001).18 However, there is no correlation between vitamin D level and PD value.18 The vitamin D supplementation significantly reduced the PD,13, 16 and the serum 25(OH)D levels reduced periodontal disease by 12%.17 However, the correlation coefficient of the serum 25(OH)D level with the PD was 0.119 (p=0.55), and this result contradicted other data.18
-Clinical attachment level
The clinical attachment loss (CAL, mm) was 12% greater in the Non-Taker (2.0) than in the Taker group (1.8, oral supplementation).13 In another team, the differences in theCAL percentage between the Taker and Non-Taker groups were 11.5 at baseline, 22.8 at 6 months, and 13.0 at 12 months. There was also a significant change over time.14 In another team, the mean CAL values were 6.3±0.7 at baseline, and reduce to 4.5±0.6 after 3 months in Taker group (intake vitamin D ≥250 IU/day with calcium ≥500 mg/day) (p=0.001).16Orlando et al. also investigated that the CAL value has a negative correlation with vitamin D level. This result indicates that a lower serum level of vitamin D is significantly associated with periodontitis.17 The CAL was 3.8±0.8 in the periodontitis group and 0.9±0.6 in the control group, respectively, showing significant differences between the periodontitis and control group (p<0.001). However, there is no correlation between vitamin D level and CAL value.18 Another team also reported that the CAL was calculated as the sum of the PD and gingival level measurements, and the mean CAL—including interproximal sites—was 3.6±1.2 in the periodontitis group and 2.1±0.6 in the control group (p<0.0001).19 The vitamin D supplementation significantly reduced the CAL,13, 14, 16 and the serum 25(OH)D levels reduced the periodontal disease by 12%.17 However, the correlation coefficient of the serum 25(OH)D level with the CAL was 0.139 (p=0.48),18 and the intake of vitamin D alone was not associated with severe periodontitis.19
-Gingival index
The gingival index (GI) is a system for assessment of the gingival condition that distinguishes the quality of the gingival. The GI has 4 grades: 0 indicates a normal condition, 1 indicates mild inflammation (slight change in colour, slight edema, no BOP), 2 indicates moderate inflammation (redness, edema and glazing, no BOP), and 3 indicates severe inflammation (marked redness and edema, ulceration, spontaneous bleeding). In a randomized controlled trial, daily oral supplementations of vitamin D were given in doses of 2000 IU/day to group A, 1000 IU/day to group B, and 500 IU/day to group C and a placebo was given to group D. The serum levels and GI were measured at baseline, on the 2nd visit on the 30thday, on the 3rdvisit on the 60thday, and on the final visit on the 90th day.The mean GI was 2.4±0.5 at baseline and 1.8±0.6 on the 2nd visit in group A (p<0.05), 2.4±0.6 at baseline and 1.2±0.7 on the 3rd visit in group B (p<0.05),2.2±0.5 at baseline and 0.9±1.0 on the final visit (p<0.05). No significant change was observed in group D (placebo). The results revealed a dose-dependent anti-inflammatory effect of vitamin D on gingivitis.15 In another team, the GI was 1.00in the Non-Taker group and 0.73 in the Taker group, showing borderline significance.13 In another team, the differences in the GI percentages between the Taker and Non-Taker groups were 38.0 at baseline, 40.5 at 6 months, and 24.0 at 12 months. There was also significance over time.14 In another team, the mean GI values were 2.1±0.4 at baseline, and reduce to 0.3±0.4 after 3 months in Taker group (intake vitamin D ≥250 IU/day with calcium ≥500 mg/day) (p=0.001).16 The vitamin D supplementation significantly reduced the GI.14-16
-CEJ-AC
Cementoenamel junction-alveolar crest (CEJ-AC, mm) measurements were made in the mesial and distal aspects of posterior teeth. The mean CEJ-AC was 19% greater in the Non-Taker group (2.1) than in the Taker group (1.7, oral supplementation).13 In another team, it was evaluated through radiographic assessment and the differences in the CEJ-AC percentages between the Taker and Non-Taker groups were 17.1 at baseline, 17.3 at 6 months, and 11.6 at 12 months. The CEJ-AC showed no change over time (between baseline, 6 months, and 12 months).14
Vitamin D, bacteria, and cytokines
-Bacteria species
There was an increase in pathogenic bacteria in the subgingival plaque with a greater PD, particularly in the red complex24—including Tannerella forsythia, Porphyromonasgingivalis, andTreponemadenticola—and in the orange complex24—including Prevotellanigrescens,andEubacteriumnodatum. The subjects were assessed at baseline and 6 months after therapy, and the levels of pathogenic bacteria—including Tannerella forsythia, Porphyromonasgingivalis, andTreponemadenticola—were significantly reduced after treatment.25
-Cytokine
Liuet et al., focused on the association between25(OH)D, bone-related markers, and periodontitis.20 Aggressive periodontitis subjects showed significantly higher PD, CAL, and BOP levels than control subjects, reflecting severe bone destruction. The aggressive periodontitis group showed a high level of osteocalcin, which reflected unbalanced bone remodelling and the need for faster bone formation. A correlation trend was found between the 25(OH)D and ALP levels, which also reflected the bone formation. The same researchers measured the 25(OH)D, osteocalcin, IL-1β, and IL-6 in the plasma and in the GCF in the periodontitis group after the initial periodontal therapy.21 The PD and BI, as well as the 25(OH)D and IL-1βlevels, were significantly lower after treatment, at 2 and 6 months. The systemic and local osteocalcin levels did not change before and after therapy.The authors concluded that the initial periodontal therapy focused on the elimination of periodontal inflammation, and therefore had no effect on the bone activity. The IL-1β level was reduced after therapy, which reflected the alleviating effect of the therapy on inflammation.
In the periodontitis group, the 25(OH)D level was extremely higher in the GCF than in the plasma.21Therefore, GF and PDL cell enzyme activity for vitamin D synthesis were suspected. For vitamin D utilization, a transformation by 25-hydroxylation and 1,α-hydroxylation is necessary. Cytochrome P450 enzymes such as CYP27A1 and CYP27B1 have been identified as vitamin D 25-hydroxylases.26 Some researchers have performed experiments with GF and PDL cells to identify enzyme activity. Results have shown that GF and PDL cells generate enzymes (CYP27A1, CYP27B1) in response to vitamin D.27, 28 Tang et al. investigated the effects of 1,25(OH)2D on the expression of IL-6 and IL-8 stimulated by P. gingivalis. 25(OH)2D significantly inhibited the IL-8 (mRNA, protein) in PDL cells both in a dose- and time-dependent manners.29Andrukhovet al. reported that both 25(OH)D and 1,25(OH)2D reduced the levels of IL-6, IL-8, and MCP-1 stimulated by P. gingivalis-LPS and heat-killed P. gingivalisin a dose-dependent manner.30 In De Filippis et al.’s study, 1,25(OH)2D inhibited the P. gingivalis adhesion and infectivity in GF and PDL cells. It also reduced the TNF-α, IL-8, and IL-12 productions, and increased the human β-defensin 3 expressions.31
Discussion
In this review, the relationship between vitamin D and periodontal diseases indicators were analyzed. And the effects of vitamin D on bacteria or cytokines have also been investigated. The data showed a negative association between vitamin D serum concentration with bleeding proportion, CAL, and GI. And intakes of vitamin D supplementation reduced PD, CAL and GI. Therefore, vitamin D can improve periodontal health. Pathogenic bacteria were also significantly decreased after therapy with vitamin D.
Conclusion
Most of the existing research has found positive associations between the serum 25(OH)D level and periodontal health, and the clinical parameters of periodontal disease were reduced by vitamin D oral supplementation. However, some studies have shown contrary results, as the researchers did not consider the demographic characteristics, latitude, seasons, and lifestyle of the subjects. Therefore, a more detailed categorization of the geographic, demographic, and lifestyle characteristics associated with the 25(OH)D level will be needed in future studies. In addition, clinicians need to gain a better understanding of the association between periodontal disease and vitamin D deficiency, and patients need to be better educated about the required vitamin D intake amount and food supplementation. In this regard, this review paper can be used as a guide by clinicians and as a reference book for patients’ education.
Conflict of Interest
The authors declare that there are no conflicts of interest.
Acknowledgement
This work was supported by the 2018 Research Fund of Ulsan College.
References
- Holick, Michael F., Dawson-Hughes, Bess. Nutrition and Bone Health. 1. Humana Press, PA: Humana Press;2004.
CrossRef - Khammissa RAG., Ballyram R., Jadwat Y., Fourie J., Lemmer J., Feller L. Vitamin D Deficiency as It Relates to Oral Immunity and Chronic Periodontitis. Int J Dent. 2018.
CrossRef - Jagelavičienė E, Vaitkevičienė I, Šilingaitė D, Šinkūnaitė E, Daugėlaitė G. The Relationship between Vitamin D and Periodontal Pathology.Medicine (Kaunas). 2018; 54(3), E45.
CrossRef - Krawiec M., Dominiak M. The role of vitamin D in the human body with a special emphasis on dental issues: a Literature review. Dent Med Probl. 2018; 55(4), 419-424.
CrossRef - Institute of Medicine, Food and Nutrition Board. Dietary Reference Intakes for Calcium and Vitamin D. Washington, DC: National Academy Press; 2010
- Institute of Medicine. Dietary reference intakes for calcium and vitamin D. Committee to Review Dietary Reference Intakes for Calcium and Vitamin D Washington DC: The National Academies Press Institute of Medicine; 2011
- Holick M.F., Binkley N.C., Bischoff-Ferrari H.A., Gordon C.M., Hanley D.A., Heaney R.P., Murad M.H., Weaver C.M. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline.J ClinEndocrinolMetab.2011;96(7): 1911–1930.
CrossRef - American Geriatrics Society Workgroup on Vitamin D supplementation for Older Adults. Recommendations abstracted from the American Geriatrics Society Consensus Statement on vitamin D for Prevention of Falls and Their Consequences. J AmGeriatr Soc. 2014; 62: 147.
CrossRef - Fischer PR, Thacher TD, Pettifor JM. Pediatric vitamin D and calcium nutrition in developing countries.Rev Endocr Metab Disord. 2008;9(3): 181–192.
CrossRef - Holick MF. McCollum Award Lecture, 1994: vitamin D–new horizons for the 21st century. Am J ClinNutr.1994;60(4): 619-630.
CrossRef - Zittermann A. Vitamin D in preventive medicine: are we ignoring the evidence? Br J Nutr.2003;89(5): 552-572.
CrossRef - Dietrich T., Nunn M., Dawson-Hughes B., Bischoff-Ferrari H.A. Association between serum concentrations of 25-hydroxyvitamin D and gingival inflammation.Am J Clin Nutr. 2005;82(3): 575-580.
CrossRef - Miley D.D., Garcia M.N., Hildebolt C.F., Shannon W.D., Couture R.A., Anderson Spearie C.L., Dixon D.A., Langenwalter E.M., Mueller C., Civitelli R. A cross-sectional study of vitamin D and calcium supplementation effects on chronic periodontitis.J Periodontol. 2009;80(9), 1433-1439.
CrossRef - Garcia M.N., Hildebolt C.F., Miley D.D., Dixon D.A., Couture R.A., Spearie C.L., Langenwalter E.M., Shannon W.D., Deych E., Mueller C., Civitelli R. One-year effects of vitamin D and calcium supplementation on chronic periodontitis. J Periodontol. 2011;82(1), 25-32.
CrossRef - Hiremath V.P., Rao C.B., Naiak V., Prasad K.V. Anti-inflammatory effect of vitamin D on gingivitis: a dose-response randomised controlled trial. Indian J Public Health. 2013;57(1): 29-32.
CrossRef - Perayil J., Menon K.S., Kurup S., Thomas A.E., Fenol A., Vyloppillil R., Bhaskar A., Megha S. Influence of Vitamin D & Calcium Supplementation in the Management of Periodontitis. J ClinDiagn Res. 2015;9(6): ZC35-38.
CrossRef - Abreu O.J., Tatakis D.N., Elias-Boneta A.R., López Del Valle L., Hernandez R., Pousa M.S., Palacios C. Low vitamin D status strongly associated with periodontitis in Puerto Rican adults.BMC Oral Health.2016;16(1): 89.
CrossRef - Laky M., Bertl K., Haririan H., Andrukhov O., Seemann R., Volf I., Assinger A., Gruber R., Moritz A., Rausch-Fan X. Serum levels of 25-hydroxyvitamin D are associated with periodontal disease. Clin Oral Investig. 2017;21(5): 1553-1558.
CrossRef - Adegboye A.R., Boucher B.J., Kongstad J., Fiehn N.E., Christensen L.B., Heitmann B.L. Calcium, vitamin D, casein and whey protein intakes and periodontitis among Danish adults. Public Health Nutr.2016;19(3): 503-510.
CrossRef - Liu K., Meng H., Tang X., Xu L., Zhang L., Chen Z., Shi D., Feng X., Lu R. Elevated plasma calcifediol is associated with aggressive periodontitis. J Periodontol. 2009;80(7): 1114-1120.
CrossRef - Liu K., Meng H., Lu R., Xu L., Zhang L., Chen Z., Shi D., Feng X., Tang X. Initial periodontal therapy reduced systemic and local 25-hydroxyvitamin D(3) and interleukin-1beta in patients with aggressive periodontitis. J Periodontol. 2010;81(2): 260-266.
CrossRef - Lee D.E., Kim J.H., Choi S.H., Cha J.H., Bak E.J., Yoo Y.J. Periodontitis mainly increases osteoclast formation via enhancing the differentiation of quiescent osteoclast precursors into osteoclasts. J Periodontal Res. 2015;50(2): 256-264.
CrossRef - Highfield J. Diagnosis and classification of periodontal disease.Aust Dent J. 2009;54 Supple 1: S11-26.
CrossRef - Teles F.R., Teles R.P., Martin L., Socransky S.S., Haffajee AD. Relationships among interleukin-6, tumour necrosis factor-α, adipokines, vitamin D, and chronic periodontitis.J Periodontol.2012;83(9): 1183-1191.
CrossRef - Socransky S.S., Haffajee A.D., Cugini M.A., Smith C., Kent RL Jr. Microbial complexes in subgingival plaque.J Clin Periodontol.1998;25(2): 134-144.
CrossRef - Cheng J.B., Motola D.L., Mangelsdorf D.J., Russell DW. De-orphanization of cytochrome P450 2R1: a microsomal vitamin D 25-hydroxylase. J Biol Chem.2003;278(39), 38084-38093.
CrossRef - Liu K., Meng H., Hou J. Activity of 25-hydroxylase in human gingival fibroblasts and periodontal ligament cells. PLoS One.2012;7(12): e52053.
CrossRef - Liu K, Meng H, Hou J.Characterization of the autocrine/paracrine function of vitamin D in human gingival fibroblasts and periodontal ligament cells. PLoS One.2012;7(6): e39878.
CrossRef - Tang X., Pan Y., Zhao Y. Vitamin D inhibits the expression of interleukin-8 in human periodontal ligament cells stimulated with Porphyromonasgingivalis. Arch Oral Biol. 2013;58(4): 397-407.
CrossRef - Andrukhov O., Andrukhova O., Hulan U., Tang Y., Bantleon H.P., Rausch-Fan X. Both 25-hydroxyvitamin-D3 and 1,25-dihydroxy vitamin-D3 reduces the inflammatory response in human periodontal ligament cells. PLoS One.2014;9(2): e90301.
CrossRef - De Filippis A., Fiorentino M., Guida L., Annunziata M., Nastri L., Rizzo A. Vitamin D reduces the inflammatory response by Porphyromonasgingivalis infection by modulating human β-defensin-3 in human gingival epithelium and periodontal ligament cells.IntImmunopharmacol. 2017;47: 106-117.
CrossRef - Hildebolt CF. Effect of vitamin D and calcium on periodontitis.J Periodontol.2005;76(9): 1576-1587.
CrossRef
Accepted on: 15-04- 2019
Second Review by: Dr. Dragana Gabrić Croatia
Final Approval by: Prof. Suhad Maatoug Bahijri





Web of Science Coverage
Emerging Sources Citation Index (ESCI)
2024 Journal Impact Factor: 1.1
Scopus Journal Metrics
CiteScore 2025: 2.6
CiteScore Details
Sustainable Nutrition: Food Systems, Nutrient Retention, and Public Health Impact
![]()
This journal is a member of, and subscribes to the principles of, the Committee on Publication Ethics (COPE)








