Benefits of Community Gardening Activity in Obesity Intervention: Findings from F.E.A.T. Programme
Wirdah Mohamed
, Ruzita Abd Talib* Nutritional Science Programme, Centre for Community Health, Faculty of Health Sciences, Universiti Kebangsaan Malaysia, Kuala Lumpur, Malaysia
Corresponding Author Email: rzt@ukm.edu.my
DOI : http://dx.doi.org/10.12944/CRNFSJ.6.3.12
Download this article as:
![]()
This study determines the beneficial effect of community gardening activity in obesity intervention among overweight and obese adults in semi-urban area. The study was one of the activities in Arus Perdana Research Grant for obesity intervention, The Fit, Eat, Active and Training (F.E.A.T) programme. The study employs a pre-post quasi experimental design assigned into intervention (n=31) and control (n=30) group respectively. The intervention group followed a series of activities for 12 weeks of intervention. In one of the activities, subjects received a nutrition counselling session with nutritionist on daily vegetables intake, while agriculture officers demonstrated the procedure of producing fertilizers from household waste and vegetable gardening techniques. The subjects were divided into groups which planted their own vegetables at the space around community hall and in the pot during the intervention period. There was significant difference (p<0.05) for vegetable intake after 12-week intervention, when 1.8 ± 0.7 serving size for the intervention group is compared to 0.7 ± 0.5 serving size for the control group. The results reported noteworthy reductions (p<0.05) in body weight with -3.5% reduction for the intervention group which was involved in gardening as compared to -0.4% reduction for the control group. Moreover, BMI reductions were observed to be -4.1% and -0.9% and waist circumference reductions were -9.9% and -4.0% for intervention group and control group respectively. In conclusion, the community gardening program is fund to be a successful activity in improving daily vegetable intake, as well as reducing the BMI and waist circumference among obese adults in semi-urban community.
KEYWORDS:Adults; Gardening; Obesity Intervention; Vegetables Intakes
Introduction
Adult obesity and diabetes incidence were increased by 3.4% and 2.3% from 2011 until 2015 respectively in Malaysia.1 Although obesity is multifactorial and complex, most researchers concur that physical inactivity and poor eating behaviour, including inadequate of vegetables and fruits intake, are two behaviours that contribute to obesity and development of metabolic syndrome and lead to increased risk of chronic diseases.2,3,4,5
Consumption of at least two servings of fruits and three serving of vegetables on daily basis can reduce the risk of cardiovascular diseases (CVD), obesity and reduce weight gain among middle-aged women. Vegetables and fruits contain helpful blends of antioxidants, phytochemicals, and fibre which can reduce risk of CVD and other non-communicable diseases such as diabetes mellitus.6 Phytochemicals in fruits and vegetables have been found to be efficient anti-obesity agents suppressing increase of adipose tissue, which is related with biomarkers of oxidative stress. Eating a lot of vegetables and fruits can modify the adiposity related metabolic biomarkers in overweight women.7
The Malaysian Dietary Guideline recommends people to consume not less than five servings of vegetables and fruits daily.8, 9 Unfortunately, not more than half of adults meet the recommendation of five serving each of fruits and vegetables intake in a day, majority of them only consume at least 20% of recommended serving size.10 However, the National Health and Morbidity Survey V, revealed that 89% of Malaysian adults consumed inadequate vegetable (less than three servings per day). There were only 11.2% Malaysian adults which consumed adequate vegetables intake (more than three servings per day). While, a study in Canada reported that a burden of about 3.3 billion dollar per year for health care cost (30.5%) and indirect costs of productivity losses (69.5%) occur due to chronic diseases. This transpires because more than half of the population did not meet the recommendation of fruits and vegetables intake and physically inactive.11
Community gardening in urban areas has been studied by many countries to observe the impact on community development and to increase the availability of fresh fruits and vegetables.12 Results from previous studies proposed that community gardens helps people to get good food, stay physically active and enhanced mental health by promoting better social health and diminish stress.13,14 Previous research works have also found that if accessibility of fruits and vegetables at home increases, its consumption will increase as well.2 However, the studies regarding the association between involvement in community gardening and vegetables and fruits intake are limited.12 Moreover, there was only one study that reported the benefits of community gardening on health and body weight.14
To date, there has not been a single study carried out in Malaysia for the efficacy of gardening activities strategies in any obesity intervention. Therefore, the present study aims to evaluate the impact of community gardening on vegetables intake, physical activity and body weight among overweight and obese adults in semi-urban area. Community gardening is one of the activities in community based weight loss intervention: Fit, Eat, Active and Training . Finding from this study would be beneficial for developing community-based intervention programme and will help to improve the strategies in weight management among obese adults.
Materials and Methods
Study design, Subjects and Sampling
This is a quasi-experimental intervention study conducted within a 12-week period. Standard deviation (SD) for body mass index (BMI) from a previous study15 was used for sample size calculation of this study using the equation below:16
n = [2σ2 / ∆2] (Zα + Zβ )2
where n = estimated sample size, σ = standard deviation for BMI from previous study = 0.70, ∆ = detectable difference = 0.56, Zα = significance level for two-sided test = 1.96, Zβ = 80 % power of study = 0.84. While taking into account a non-response rate of 50 %, the required sample size was increased to 37 people for each group.
The purposive sampling method was used to determine the sample of the study. Sample selection was conducted in one of the districts with the highest prevalence of obesity in Malacca. While early screening was conducted to identify the following inclusion criterias: (1) aged between 25-59 years; (2) overweight or obese (BMI > 23 kg/ m2; (3) able to read, write and understand Malay and; (4) willing to join F.E.A.T programme. Exclusion criteria’s were subjects with diabetes, hypertension, cardiovascular diseases, pregnancy and physical disability.
The study protocol was reviewed and approved by the ethics committee of Research Ethics Committee of the University Kebangsaan Malaysia (UKM PPI/111/8/JEP-2016-392). A written informed consent was obtained from each subject prior to the intervention. Subjects were requested to complete a socio demographic questionnaire which included age, sex, educational level, household income, occupation and medical history at baseline data collection.
Anthropometry and Body Fat Measurements
Weight, BMI and percentage of body fat were measured using Tanita Body Composition Analyzer TBF-300 Model (Tanita Corporation, Japan). The classification of body fat percentage was referred to the guidelines by Wardlaw and Kessel,17 in which the magnitude percentage of body fat differ with different gender and age. While BMI was categorized as ‘normal’ (18.5 kg/m2 ≤BMI ≤22.9 kg/m2), ‘overweight’ (23.0 kg/m2 <BMI ≤24.9 kg/m2), ‘pre-obese’ (25.0 kg/m2 <BMI ≤ 29.9 kg/m2) or ‘obese’ (>30.0 kg/m2).18
Height was measured twice to the nearest 0.1 cm without shoes using SECA Body meter 217 (SECA GmbH & Co., Hamburg, Germany). Waist circumference (WC) was measured twice, to nearest 0.1 cm by using a Lufkin tape model W606PM (Apex Tool Group, Maryland, USA). Measurement was taken immediately above the right iliac crest at the mid-axillary line according to the method used in Centres for Disease Control and Prevention National Health and Nutrition Examination Survey, 2000. WC was classified as ‘normal’ for men (≤94 cm) and women (≤80 cm).19 All measurements were carried out by a trained researcher.
Vegetables Intake
Serving size of vegetable intake was obtained from the 24-hour diet recall. One serving size is equivalent of half cup of vegetables and Malaysian Dietary Guideline recommends to consume 3 servings (1 ½ cup) of vegetables daily.8 The 24-hour diet recall was done for three non-sequential days, which consisted of 2 weekdays and 1 weekend day in a week . Nutritionist ProTM software (Axxya Systems, United States), was used to analyse calorie and nutrients intake from the diet recalls. The under-reporting of calories intake estimation was determined by the ratio of reported total Energy Intake (EI) and Basal Metabolic Rate(BMR).20 The ratio of EI/BMR below 1.2 was classified as under-reporting.15 In this study, it was found that half (50.6%) of the participants were under-reporters, 45.3% were accurate and only 4% were over-reporters. However, this work took all the data and did not excluded the under or over-reported data.
Physical Activity Measurement
The of the subjects for pre and post intervention were measured using International Physical Activity Questionnaire (IPAQ).21 Three levels of physical activity are suggested from the categorical score; which are low, moderate and high. Moderate physical activity level was considered if the subjects were satisfied with these criteria: 1) at least three days of vigorous activity for 20 minutes or more each day; 2) at least five days of moderate activities or walking for 30 minutes or more each day or; 3) Achieving at least 600 Metabolic Equivalents of Task (MET)-minutes/week by doing of any combination of walking, moderate-intensity or vigorous-intensity activities for at least five day per week. While high physical activity was considered when the subjects had vigorous-intensity activity for three or more days achieving at least 1500 MET-minutes/week or spent every day on any combination of walking, moderate-intensity or vigorous-intensity activities and accumulated 3000 MET-minutes/week or more. Low physical activity level or inactive was considered for those who do not meet the standard either for moderate or high activity category.22
Fit, Eat, Active and Training (F.E.A.T) Programme
Fit, Eat, Active and Training (F.E.A.T) programme is a semi-urban community based weight loss program, focusing on dietary, physical activity and behaviour change strategies. F.E.A.T programme intervention consists of three main components; 1) nutritional education; 2) interactive and informative education sessions and; 3) participation in physical activity and exercise training. The intervention group received 12 weeks of the intervention while the control group did not receive any intervention activities. However health talk was conducted after the entire F.E.A.T programme was completed. Figure 1 shows 12- weeks of F.E.A.T intervention component.
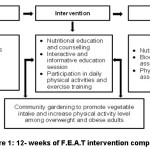 |
Figure 1: 12- weeks of F.E.A.T intervention component |
Education F.E.A.T Module was used during individual counselling, interactive and informative class room seminar, carnival and cooking demonstration. Subjects were received individual nutrition counselling session with nutritionist based on individual calorie requirement, as well as portion of vegetables intake and tips to increase vegetables intake. Growing their own vegetables is one of the tips to provide them with fresh vegetable and they can eat as salad or ulam (Malay language) at any time. Cooking demonstration based on F.E.A.T healthy recipe book (Mudah, Sihat, Sedap) was conducted by the professional chef and assisted by the nutritionist to encourage subjects increase vegetables intake with low fat cooking method and use less salt in cooking.
Community Gardening
Community gardening is one of the activities in F.E.A.T programme. Subjects were divided into five groups for community gardening activity. The agriculture officers were demonstrated the procedure for production of fertilizer from household wastes and vegetable gardening technique in one of the education sessions. Subjects were planted their own vegetables at the space around community hall and planting in pots. Community gardening session was held for at least 30 minutes three times per week during the intervention period. Brinjal, lady fingers, spinach, mustard and chili were the vegetables planted by the subjects around the community hall. They were also advised to plant vegetables around their backyard.
Statistical Analysis
SPSS (version 23) was used to analyse all the data. Kolmogorov–Smirnov test was used to examine the normality distribution of each variable. The frequency, percentage, mean and standard deviation were reported. Then the outcome was examined by comparing means using paired t-test and independent t-test. Nutritionist Pro™ software was used to analyse participant’s nutrient intake from three days of 24-hour diet recall. While daily serving size of vegetables and the frequency of vegetables intake were obtained through the interview.
Results
Study Participants
Among 74 subjects who were agreed to be involved in this study, only 61 subjects joined this programme until the end of 12- week intervention. There were 31 subjects for intervention group and 30 subjects for control group respectively. All of the subjects were Malay, consisted of 21% (n=13) males and 79% (n=48) females. Hence, the data was not representative for sex to make statistical comparisons as not many males’ subjects were consented to participate in the study. Mean age of the subjects was 46.4 ± 8.9 years old. The average monthly income was Malaysian Ringgit (MYR) 1716.40 ± 867.80 while their majority education level was at upper secondary school (68.8%) (Table 1). There was no significant difference for monthly income between intervention and control group but age was significantly different for the two groups (p<0.05).
Table 1: Demographic Characteristics of Participants
| Characteristics | Intervention Group (n=31) | Control Group (n=30) | Total(n=61) |
| Sex | |||
| Male | 6 (19.4%) | 7 (23.4%) | 21% (n=13) |
| Female | 25 (80.6%) | 23 (76.6%) | 79% (n=48) |
| Mean age (year) | 49.1 ± 6.1* | 43.7 ±10 | 46.4 ± 8.9 |
| Mean monthly income (MYR) | 1590.32 ± 751.15 | 1846.96 ± 969.44 | 1716.40 ± 867.80 |
| < 1500 | 15 (48.4%) | 14 (46.7%) | 47.5% (n=29) |
| 1501-3000 | 16 (51.6%) | 14 (46.7%) | 49.2% (n=30) |
| >3000 | – | 2 (6.7%) | 3.3% (n=2) |
| Education | |||
| No formal education | 2 (6.5%) | 1 (3.3%) | 5.0% (n=3) |
| Primary school | 2 (6.5%) | 4 (13.3%) | 9.8% (n=6) |
| Lower secondary school | 9 (29.0%) | 1 (3.3%) | 16.4% (n=10) |
| Upper secondary school | 18 (58.0%) | 24 (80.0%) | 68.8% (n=42) |
*Independent t-test: Significant difference (p<0.05) between intervention and control group
Vegetables Intake
The intervention resulted in increment of vegetables serving size intake, vegetables frequency intake and reduction in total calorie intake significantly after 12 week of intervention among intervention group compared to the control group (Table 2). Mean vegetables serving size intake for intervention group was significantly increased from 0.8 ± 0.7 serving size at pre intervention to 1.8 ± 0.7 serving size after intervention and there was no increment in vegetables serving size intake among the control group. While there was significant difference (p<0.05) for vegetables serving size intake at post- intervention between intervention and control group which were 1.8 ± 0.7 and 0.7 ± 0.5 serving size intakes respectively.
There was significantly increment (p<0.05) for frequency of vegetables intake among intervention group which was 0.9 ± 0.7 times/day at pre-intervention and 1.9 ± 0.7 times/day at post-intervention. Frequency of vegetables intake at post-intervention was also significantly different between the two groups. The frequency of vegetables intake was 1.8 ± 0.7 for intervention group and 0.7 ± 0.5 for control group.
Significant reduction (p<0.05) was also observed in total calorie intake after intervention from 1428 ± 638 at pre intervention to 1053 ± 418 (kcal/day) at post-intervention among intervention group. While there was significant difference (p<0.05) for total calorie intake between the two groups, where intervention group has a calorie intake of 1053 ± 418 (kcal/day) while the control group has a calorie intake of 1364 ± 715 (kcal/day) after 12 weeks of intervention.
Table 2: Vegetables Intake, Total Calorie Intake at pre- and Post-Intervention for Each Group (Mean ± SD)
| Variables | Intervention Group (n=31) | Control Group (n=30) | ||
| Pre-intervention | Post-intervention | Pre-intervention | Post-intervention | |
| Vegetables intake (serving size/day) | 0.8 ± 0.7 | 1.8 ± 0.7*1 | 0.7 ± 0.7 | 0.7 ± 0.5 |
| Frequency of vegetables intake(times/day) | 0.9 ± 0.7 | 1.9 ± 0.7*1 | 1.0 ± 0.8 | 1.1± 0.8 |
| Total calorie intake (kcal/day) | 1428 ± 638 | 1053 ± 418*1 | 1291 ± 794 | 1364 ± 715 |
*Paired t-test: Significant difference (p<0.05) for pre and post intervention within group
1Independent t-test: Significant difference (p<0.05) for post intervention between intervention and control group
Physical Activity Score
Mean total of physical activity score was observed to increase among intervention group from 2239 ±1303 at pre-intervention to 4605 ±1993 (MET-minutes/week) at post-intervention, while there was no increment among control group. There was significant difference (p<0.05) for total physical activity score after 12 weeks of intervention between intervention and control group which were 4605 ±1993 and 1800 ± 925 (MET-minutes/week) respectively (Table 3).
Table 3: Physical Activity Score at pre- and Post-Intervention for Each Group (Mean ± SD)
| Variables | Intervention Group (n=31) | Control Group (n=30) | ||
| Pre-intervention | Post-intervention | Pre-intervention | Post-intervention | |
| Total PA score(MET-minutes/week) | 2239 ±1303 | 4605 ±1993*1 | 1808 ± 1042 | 1800 ± 925 |
*Paired t-test: Significant difference (p<0.05) for pre and post intervention within group
1Independent t-test: Significant difference (p<0.05) for post intervention between intervention and control group
Anthropometry and Body Fat
Table 4 shows the significant reduction (p<0.05) in the body weight from 71.4 ± 10.6 to 68.9 ± 11.0 kg, BMI from 29.0 ± 4.5 to 27.8 ± 4.6 kg/m2 , WC from 91.9 ± 8.8 to 82.8 ± 9.4cm and for body fat percentage from 37.6 ± 9.0 to 36.0 ± 8.8% among intervention group. There were also significant difference (p<0.05) for body weight, BMI and WC reduction between the two groups after 12 weeks of intervention.
Table 4: Anthropometry Value and Body Fat at pre- and Post-Intervention for Each Group (Mean ± SD)
| Variables | Intervention Group (n=31) | Control Group (n=30) | ||
| Pre-intervention | Post-intervention | Pre-intervention | Post-intervention | |
| Body weight (kg) | 71.4 ± 10.6 | 68.9 ± 11.0*1 | 78.7 ± 14.3 | 78.4 ±13.8 |
| BMI (kg/m²) | 29.0 ± 4.5 | 27.8 ± 4.6*1 | 31.0 ± 5.2 | 31.3 ± 5.1 |
| WC (cm) | 91.9 ± 8.8 | 82.8 ± 9.4*1 | 97.3 ± 9.8 | 93.4 ± 9.3 |
| Body fat (%) | 37.6 ± 9.0 | 36.0 ± 8.8* | 40.7 ± 8.9 | 40.1 ± 9.4 |
Discussion
This study revealed that the majority of the subjects did not fulfil the recommendation of vegetables intake where they were only taking less than one serving of vegetable at one meal time per day. It was contrary to the recommendations to consume vegetables and fruits with every meal times for beneficial effect on health and reduction of chronic diseases.23 Vegetables and fruits intakes among adults are inadequate and below the recommendations in many countries despite of the fact that a lot of studies have been shown the beneficial effect on the health.7 Beside, study in Brazil showed that most of the population is most likely to choose sweetened food and food high in fat compared to the fruits and vegetables.24
The reasons for not eating vegetables and the barriers for eating fruits and vegetables are high cost, lack of time to prepare the food, limited fresh sources, unavailability at home, and limited knowledge of the subjects about the way to add more servings of vegetables in their diet.25,26,27,28 Vegetables are easily wilt and damaged, they have to be consumed quickly, which is one of the reason people do not take vegetables daily, especially for those who work and rarely go to markets or grocery stores. They tend to purchase other foods with a longer shelf life. The subjects also complained that they cannot do gardening in their house compound as their parent practiced before.26
Therefore, community gardening and growing our own vegetables at home in our intervention activity provided fresh vegetables with a minimum cost where the subjects can eat directly raw vegetable as a salad or ulam at any time and they can save time to cook vegetables. It was proven that the vegetables intake was increased from 0.8 to 1.8 serving size per day and the frequency of vegetables intake also increased from 0.9 to 1.9 times daily at post-intervention among intervention group compared to control group. The study suggests that those who are gardener can eat vegetables at any time they want it. They can take vegetables during breakfast, lunch and dinner as the vegetables are always available at home. This finding is consistent with the argument that adults who engage in the community gardening may eat more than 1.4 times of fruits and vegetables daily as compared to others who did not engage in that activity.29
Ulam or a type of Malay salad is one of vegetables planted in the F.E.A.T gardening activity. Ulam is one of the favourite dishes especially among Malay community. Ulam are not contaminated by chemicals or pesticides and contain important nutrients for human health, and are potential source for increasing vegetable consumption to meet recommendation by World Health Organization (WHO), which is 400 g per day.30 While Malaysian Dietary Guideline recommends to consume five portions or more of fruit and vegetables daily. The serving size recommendation will avoid intakes of high fat and energy food which contains less of nutrients.31 The recommendation was supported by Mohamed,32 whereby optimum consumption of fruit and vegetables benefits the human beings with good nutritional values.
Study by Nelson et al.,27 and Alaimo et al.,28 also reported that the subjects engaged on food planting activities and participated on community gardening increased their vegetables intakes per day than those who did not participate. Adults who participated in a community garden consumed 40% more fruits and vegetables daily than those who did not participate, and they were 3.5 times more likely to consume the recommendation of 5 portion daily of fruits and vegetables. Community gardening was a potential nutrition intervention because it addressed a primary barrier when trying to eat a healthful and fresh fruit and vegetables.28
Gardening is one of the F.E.A.T intervention activities to increase the physical activity among our overweight and obese subjects. They have to involve in the gardening task for at least 30 minutes, three times per week to increase their physical activity level which helps to reduce their weight. Overweight and obese people need to increase their energy expenditure by gradually increasing the physical activity up to 60-90 minutes daily to improve glycaemic control, weight maintenance and reduce the risk of CVD.33 Studies also showed that the effects of physical activity apart from weight loss are improved body compositions and reduced morbidity and mortality.34, 35
All weight management programmes whether initiated by individual or grouping for free or profit-oriented programme should recommend regular engagement in physical activity in daily life, to be more active.36 To improve physical activity they can do a lot of beneficial physical activities daily such as gardening activities, walking up stairs, washing the car, mopping the floor etc.33,36 Gardening is one of the enjoying leisure-time activity by many people which provides a good effect for physical and mental health. While vegetables gardening activity could increase vegetables intake among subjects and indirectly can increase physical activity which can help to reduce body weight and waist circumference.35,36
Subjects involved in our community gardening increased their physical activities level from moderate (2239 ±1303 MET-minutes/week) to high physical activity level (4605 ±1993 MET-minutes/week). Unfortunately, the control group which is not involved in community gardening still has a moderate physical activity level until the end of the intervention. Subjects performed a lot of digging, planting task and mixing soil during plantation of the vegetables. They also used a lot of upper body part when mixing soil and planting in pots. Gardening activity was categorised as moderate intensity physical activity using both upper and lower body part at the same time. Digging and planting task were categorised in moderate intensity activity and provided a good health effect as compared to the non-gardening form of physical activity. While gardening task that uses a lot of upper body part for harvesting, mixing soil were categorised as low-intensity activity.37,38
This study also shows a significant reduction in body weight for subjects who were involved in community gardening (-3.5%) as compared to the control group (-0.4%). While BMI reductions were -4.1% and -0.9% and waist circumference reductions were -9.9% and -4.0% for intervention and control group respectively. Consistent with a study by Zick et al., 14 who revealed that both women and men who involved in community gardening had significantly lowered their BMI’s compared to their neighbours who were not involved in that activity. The estimated BMI reductions were –1.84 for women and –2.36 for men and this study was conducted from relatively large numbers of community gardeners by using a post-test comparison group design to assess the impact of community gardening on BMI. However he proposed a randomized field experiment or quasi-experiment for conclusive assessment of community gardening impact on participants’ weight.
This study had several limitations. Data were limited by the estimation of vegetables consumption. The limitation of the accuracy estimation of vegetables consumed may happen, due to the difficulty in reporting their consumption as vegetables physical form are irregular and the vegetables are consumed generally with other ingredients which does not necessarily correspond to a serving size.23 In this study, the difficulty of vegetables estimation happened in determining the vegetable serving size when it prepared in noodles, fried rice and other Malaysian foods. Another factor that may affect the accuracy of dietary intake assessment is that the subjects might over report on vegetables consumption because high intake of vegetables can show a healthy eating. Furthermore, 24-hour recall used in this study is not the gold standard for the assessment of food consumption. None of the methods is extremely accurate for the assessment of fruits and vegetables consumption, whether it is isolated or combined method.23 However, to avoid the methodology errors, the interviews were carried out by the trained interviewers, with household measurement and pictures from Atlas of Food Exchanges and Portion Sizes.39
Second limitation was the physical activity assessment. The study did not report on MET-minutes/week for gardening task specifically. Physical activity was assessed using IPAQ in this study. The IPAQ is a set of four domains including leisure time physical activity, domestic and gardening (yard) activities, work-related physical activity and transport-related physical activity. The items in IPAQ form were structured to provide separate scores on walking activity, moderate-intensity activity and vigorous-intensity activity. The estimation of a specific domain cannot be estimated.22 Moreover, there are not enough data on exercise intensity of various common gardening tasks to be used in developing the gardening programme especially for improving health of adults.38
The strengths of our study is that we focused on assessing the benefits of community gardening with vegetables intake, body weight, BMI and waist circumference among overweight and obesity adults who are involved in community gardening. There were a few studies that assessed the association of participation in community gardening with BMI and obesity as a new potential of gardening on health.14 Secondly, we also used a quasi-experimental design that compared all the results of gardeners with those who did not participate in community gardening. There are only a few previous studies that have compared community gardeners to the nongardeners.12,14,40
In conclusion, the study showed that community vegetables gardening increased vegetables intake among subjects and made them physically active that drives to improved body weight, BMI and waist circumference.
Acknowledgements
This study is part of “Fit, Eat, Active and Training (F.E.A.T) Projects funded by Arus Perdana Grant (Code: AP 2014-025). Special thanks to all the subjects for their full cooperation. The efforts and dedications of the researchers, data collection team and all those involved in this project are also acknowledged.
Conflicts of Interest
None to declare
References
- Institute of Public Health (IPH). National Health and Morbidity Survey V (NHMS V). Ministry of Health Malaysia. 2015.
- Suresh V et al., Assess the Effectiveness of Structured Health Education Program Regarding Obesity among Adults Residing at Waghodia Taluka. Int. Journal of Advances Nursing Management. 2016;4(4):372-374.
- Spears-Lanoix E. C., McKyer E. L. J., Evans A., McIntosh W. A., Ory M, Whittlesey L., Kirk A. et al., Using Family-Focused Garden, Nutrition, and Physical Activity Program To Reduce Childhood Obesity: The Texas! Go! Eat! Grow! Pilot Study. Childhood Obesity. 2015;11(6):707–714.
CrossRef - Cavill N., Ells L. Treating adult obesity through lifestyle change interventions. A Briefing Paper for Commissioners. National Obesity Observatory; Oxford, UK. 2010.
- Vieira A. R et al., Fruits, vegetables, and bladder cancer risk: a systematic review and meta-analysis. Cancer Medicine. 2015;4(1):136–146.
CrossRef - He K., Hu F. B., Colditz G. A., Manson J. E., Willett W. C., Liu S. Changes in intake of fruits and vegetables in relation to risk of obesity and weight gain among middle-aged women. International Journal of Obesity. 2004;28(12):1569–1574.
CrossRef - Pem D., Jeewon R. Fruit and vegetable intake: Benefits and progress of nutrition education interventions- Narrative Review Article. Iranian journal of public health. 2015;44(10):1309–21.
- Malaysian Dietary Guideline. National Coordinating Committee on Food and Nutrition. Ministry of Health Malaysia. 2010.
- World Health Organization. Diet, nutrition and the prevention of chronic diseases. Report of a Joint WHO/FAO Expert Consultation. WHO Technical Report Series 916, Geneva. 2003.
- Nicklett E. J., Kadell A. R. Fruit and vegetable intake among older adults: a scoping review. NIH Public Access. 2014;75(4):305–312.
- Ekwaru J. P., Ohinmaa A., Loehr S., Setayeshgar S., Thanh N. X., Veugelers P. J. The economic burden of inadequate consumption of vegetables and fruit in Canada. Public Health Nutrition. 2017;20(3):515–523.
CrossRef - Alaimo K., Packnett E., Miles R. A., Kruger D. J. Fruit and Vegetable Intake among Urban Community Gardeners. Journal of Nutrition Education and Behavior. 2008;40(2):94- 101.
CrossRef - Schmutz U. et al., The benefits of gardening and food growing for health and wellbeing. Available from:URL:http://www.sustainweb.org/resources/files/reports/GrowingHealth_BenefitsReport/April 2014/ 27
- Zick C. D., Smith K. R., Kowaleski-Jones L., Uno C et al., Harvesting more than vegetables: The potential weight control benefits of community gardening. American Journal of Public Health. 2013;103(6):1110–1115.
CrossRef - Soon H. K., Saad H. A., Taib M. N. M., Rahman H. A., Mun C. Y. Effects of combined physical activity and dietary intervention on obesity and metabolic parameters in adults with abdominal obesity. The Southeast Asian journal of tropical medicine and public health. 2013;44(2):295–308.
- Naing N. N. Sample size determination in experimental studies. A practical guide on determination of sample size in health sciences research. Pustaka Aman Press Sdn. Bhd, Kelantan. 2009;66.
- Wardlaw G. M., Kessel M. Perspective in Nutrition. McGraw Hill, New York, USA; 5th ed: (2002).
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic. World Health Organization. 2000.
- World Health Organization. Waist Circumference and Waist-Hip Ratio: Report of a WHO Expert Consultation. Geneva. 2008.
- Macdiarmid J., Blundell J. Assessing dietary intake: Who, what and why of under-reporting. Nutrition research reviews. 1998;11(2):231–253.
CrossRef - Shamsuddin N., Koon P. B., Zulkifli S., Zakaria S., Noor M. I., Jamal R., Dato ’, P. Reliability and Validity of Malay Language Version of International Physical Activity Questionnaire (IPAQ-M) among the Malaysian Cohort Subjects. International Journal of Public Health Research. 2015;5(2).
- IPAQ I. P. A. Q. Guidelines for data processing and analysis of the International Physical Activity Questionnaire (IPAQ): short and long forms. Available from: URL: http:// www.Ipaq.Ki.Se /Scoring.Pdf/November 2005/1–15.
- Lopes M. S., Santos., L. C. dos., Lopes A. C. S., Abreu M. N. S. Comparison between two assessment tools for fruit and vegetable intake relative to the 24-h recall. Nutrition. 2017;38:34–40.
CrossRef - Figueiredo I. C. R., Jaime P. C., Monteiro C. A. Factors associated with fruit and vegetable intake among adults of the city of São Paulo. Rev Saude Publica. 2008;42(5).
- Richards J. E., McClure J. B., Alexander G. L. Why People Don’t Eat Fruit and Vegetables: Insight from Subjects Who Enrolled in MENU. Clinical Medicine & Research. 2010;8(1):32.
CrossRef - Yeh M. C., Ickes S. B., Lowenstein L. M., Shuval K et al., Understanding barriers and facilitators of fruit and vegetable consumption among a diverse multi-ethnic population in the USA. Health Promotion International. 2017;23(1):42-51.
CrossRef - Nelson J et al., Low income diet and nutrition survey. Volume 3 Nutritional status, physical activity, economic, social and other factors. London: Food Standards Agency The Stationary Office, UK. 2011.
- Alaimo K., Packnett E., Miles R. A., Kruger D. J. Fruit and Vegetable Intake among Urban Community Gardeners. Journal of Nutrition Education and Behavior. 2008;40(2):94- 101.
CrossRef - John J. H., Ziebland S. Reported barriers to eating more fruit and vegetables before and after participation in a randomized controlled trial: A qualitative study. Health Education Research. 2004;19(2):165–174.
CrossRef - Ahmad N. I., Abdullah A., Abdullah M. F., Heng L.Y et al., Tabiat pengambilan ulam-ulaman di kalangan orang dewasa pelbagai etnik di Selangor. Jurnal Sains Kesihatan Malaysia. 2010;8(2):27–35.
- National Institute for Health and Care Execellence. Obesity: guidance on the prevention, identification, assessment and management of overweight and obesity in adults and children. NICE clinical guideline. 2006;43:1-84.
- Mohamed S. Functional foods against metabolic syndrome (obesity, diabetes, hypertension and dyslipidemia) and cardiovascular disease. Trends in Food Science & Technology. 2014;35(2):114-128.
CrossRef - Kruegle E. Factors that motivate obese and overweight patients to adhere to lifestyle change. Degree Thesis, University of Applied Sciences. 2012.
- Baillot A., Romain A. J., Boisvert-Vigneault K., Audet M., Baillargeon J. P., Dionne I. J., Valiquette L. et al., Effects of Lifestyle Interventions That Include a Physical Activity Component in Class II and III Obese Individuals: A Systematic Review and Meta-Analysis. Plos One; 10(4): e0119017. 2015.
- Jepsen R., Aadland E., Robertson L., Kolotkin R. L., Andersen J. R., Natvig G. K. Physical activity and quality of life in severely obese adults during a two-year lifestyle intervention programmeme. Journal of obesity. 2015;314194.
- Cavill N., Ells L. Treating adult obesity through lifestyle change interventions. A briefing paper for commissioners. Oxford: National Obesity Observatory. 2010;1-18.
- Park S., Lee A., Lee K., Son K. Gardening tasks performed by adults are moderate- to high-intensity Physical activities. Hort Technology. 2014;24(1):3–8.
CrossRef - Park S., Lee K., Son K. Determining exercise intensities of gardening task as a physical activity using metabolic equivalents in older adults. Hort Science. 2014;46(12):1706-1710.
- Suzana S., Noor Aini M. Y., Shanita S. N. Atlas of food exchanges and portion sizes. MDC Publisher, Kuala Lumpur. 2nd ed. 2009.
- Blair D., Sherman S., Giesecke C. C. A dietary, social and economic evaluation of the Philadelphia Urban Gardening Project. J Nutr Educ. 1991;23(4):161-167.
CrossRef
Accepted on: 06-12-2018
Second Review by: Yashvee Dunneram (U.K)
Final Approval by: Prof. Min-Hsiung Pan





Web of Science Coverage
Emerging Sources Citation Index (ESCI)
2024 Journal Impact Factor: 1.1
Scopus Journal Metrics
CiteScore 2025: 2.6
CiteScore Details
Sustainable Nutrition: Food Systems, Nutrient Retention, and Public Health Impact
![]()
This journal is a member of, and subscribes to the principles of, the Committee on Publication Ethics (COPE)








