Eating Disorders Among Saudi Dietitians: Prevalence and Analysis
 and Renad Ahmad Tarawah1
and Renad Ahmad Tarawah1 1Department of Clinical Nutrition, Umm Al-Qura University, Makkah, Saudi Arabia.
2Department of Nutrition and Food Science, Menofia University, Shebein El-Kom, Egypt.
Corresponding Author E-mail: ehbakr@uqu.edu.sa
DOI : http://dx.doi.org/10.12944/CRNFSJ.12.1.19
Download this article as:
![]()
Eating disorders (EDs) involve persistently disturbed eating and related behaviors that result in altered consumption or absorption of food with potential physical or psychological function impairment. There are four major types of EDs: anorexia nervosa, bulimia nervosa, binge eating disorder, and eating disorders not otherwise specified. This investigation aimed to study the prevalence of EDs by assessing the nutritional status of nutrition students and dietitians from multiple provinces in Saudi Arabia. A cross-sectional study included 175 male and female nutrition students and dietitians. EDs were diagnosed using the Eating Attitudes Test – 26 item (EAT-26) and Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Dietary intake was estimated using repeated 24-hour recall records. Diets were analyzed using food processor nutrition and fitness software. The intakes were compared with the recommended dietary allowances (RDA). The mean participant age was 24.62 ± 4 years. According to EAT-26 diagnostic criteria, the prevalence of EDs was 15.4%. The ED participants had normal body mass index values of 23.6 ± 3.47kg/m2. The diet analysis showed that these subjects had a lower intake of energy, macronutrients, and micronutrients but higher intakes of other micronutrients than the RDA. Nine (33.3%) of the subjects were students and 18 (66.7%) were dietitians. l EDs were more prevalent among dietitians than students. The EDs included a high number of other specified feeding or eating disorders and unspecified eating disorder cases. Subjects with ED had an unbalanced diet and poor nutrition. Our investigation concluded that the prevalence of EDs in Saudi Arabia was 15.4% among nutrition students and dietitians. Moreover, EDs were more prevalent in some provinces of Saudi Arabia. Intakes of energy, macronutrients, and some micronutrients were low, while those of other micronutrients were higher than the RDA.
KEYWORDS:DSM-5; Dietitians; Eating disorder; EAT-26; Nutrition Students
Introduction
Eating disorders (EDs) are defined as persistent disturbed eating patterns and eating-related behaviors that result in altered food consumption or absorption and potential physical or psychological function disruptions. According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), there are eight major types of EDs: anorexia nervosa (AN), bulimia nervosa (BN), binge eating disorder (BED), pica, rumination disorder, avoidant/restrictive food intake disorder (ARFID), eating disorder not otherwise specified (EDNOS), and unspecified feeding or eating disorder (UFED) 1. AN is defined as a psychological illness or syndrome characterized by an intense fear of fatness or seeking a low body weight. The body mass index (BMI) of patients with AN is reportedly very low at less than 17.5 kg\m2. Affected individuals restrict their high-fat food intake and exercise excessively 2. BN is a life-threatening psychiatric illness characterized by the overeating of high-calorie food in a short time paired with self-induced vomiting, laxative and diuretic use, fasting, or over-exercising to avoid weight gain 3.
BED is characterized by the eating of a large amount of food in a short time compared to normal individuals. Sufferers also feel guilty or depressed after eating, consume food alone to avoid embarrassment, and eat food even when not hungry. To diagnose BED, binge episodes must occur once per week for 3 months or more, and the syndrome must not be influenced by any normal compensatory behavior 4. Pica is defined as eating items that are not typically thought of as food and do not contain significant nutritional value, such as hair, dirt, or paint chips 5. Rumination disorder is characterized by the repeated and unintentional regurgitation of food, usually during or immediately after eating 6. ARFID is similar to anorexia in that both involve limiting the amount and/or types of food consumed; however, unlike anorexia, ARFID does not involve any distress about body shape or size or fears of fatness 7. EDNOS is defined by the DSM-5 as those who have an ED but do not satisfy the diagnostic criteria for any of the previous ED types. The most recent DSM-5 update renamed this type as other specified feeding or eating disorders (OSFED), which include several illnesses such as purging disorder, atypical AN, subthreshold BN, and subthreshold BED 8.
UFED is applied to those who have an ED but do not meet the diagnostic criteria for any of the previous types of OSFED. Another type of EDs that is not described by the DSM-5 is orthorexia nervosa (ON), which is characterized by an unhealthy obsession with healthy eating that emphasizes following extreme rules for “clean and pure” nutrition and unreasonable specifications for food selection and/or preparation 9.
The nutritional status of eating disorders and nutrition plays a major role among individuals with ED. Malnutrition is common because of the low consumption of macro- and micronutrients in AN and BN. Moreover, this restriction can affect micronutrient availability, resulting in compromised immunity; loss of lean body mass; fatigue; altered brain function; and deficiencies in vitamin D, calcium, folate, cobalamin, zinc, magnesium, thiamine, riboflavin, niacin, pyridoxine, C, E, K, and Fe, leading to anemia. Replacing these nutrients is an important part of nutritional therapy to enhance patient recovery 10,11. EDs can affect multiple organ systems and be potentially life-threatening. These disorders can lead to changes in the gastrointestinal system. Food restriction and vomiting can cause digestion and interrupt normal stomach functions, leading to nausea, blotting, gastroparesis, constipation, anemia, and blood sugar fluctuations. EDs can also affect the cardiovascular system 12. AN has specific health consequences due to the extreme caloric restriction. Symptoms include hypokalemia, hypoglycemia, abdominal discomfort, and loss of bone mineral density 13. BN is associated with xerosis, an electrolyte imbalance leading to arrhythmias, early satiety, gastroparesis, constipation related to laxative abuse, gastroesophageal reflux, and malnutrition 14. BED also features complications, such as diabetes, dysphagia, diarrhea, blotting, nutrient deficiencies, and increased risk of cancer, hypertension, and obstructive sleep apnea 15. The epidemiological incidence of EDs reported in the United Kingdom is AN, 7.4%; BN, 0.8%; BED, 3.6%; and OSFED, 2.4%. In Finland, the prevalence of AN among females is 3.6%, while that of OSFED is 0.6%. In Holland, the rate of EDs among females is 3.7%, while that of AN is 1.2%, BN is 0.6%, BED is 1.6%, and OSFED is 0.3%. The rate of Eds among males is 0.5%, that of AN and BN is 0.1%, and that of BED is 0.3%. In Switzerland, among females, the rate of AN is 1.9%, while that among males is 0.2%. In Germany, the rate of AN is 0.3%, BN is 0.4%, and BED is 0.5%. In Sweden, for females, the rate of BN is 1.6% and that of BED is 0.4%. In Australia, the rate of ED is 16.3%, AN is 0.46%, BN is 0.66%, and BED is 5.58%. In the United States, the rate of AN among females is 1.37% and that of BED is 1.7%; the rate of BED among males is 0.8%. In Canada, the rate of EDs among females is 4.46%, AN is 0.06%, BN is 2.01%, and BED is 0.68%; among males, the rate of EDs is 2.21%, BN is 1.31%, and BED is 0.16% 16.
The prevalence of EDs in the Middle East and North Africa region is 16.9% in the United Arab Emirates (specifically for BED). Egypt has a 65.0% prevalence of EDs. In Saudi Arabia (Dammam), 29.4% of females have ED; these rates are 35% and 23.3% for Taif and Arar cities, respectively 17-20. Another study aimed to determine the frequencies of ON and EDs among dietitians 21. Moreover, a study assessed ED behavior and addiction to food among 967 nutrition and non-nutrition students 22, and another determined the number of risky behaviors of EDs and body image satisfaction among 743 female nutrition students and dietitians 23.
Accordingly, this investigation aimed to study the prevalence of EDs by assessing the nutritional status of nutrition students and dietitians from multiple provinces in Saudi Arabia.
Materials and Methods
Study type and duration
This epidemiological descriptive cross-sectional study was conducted in Saudi Arabia between October 2020 and March 2021.
Study setting and sampling
Nutrition students and dietitians aged 18–55 years from different nutrition colleges and hospitals in the 13 provinces of Saudi Arabia were the target group. Subjects with chronic diseases, such as diabetes, hypertension, and hypo/hyperthyroidism, as well as pregnant and lactating women, were excluded from the study. Only dietitians and students of a dietetic school at any academic level were eligible for inclusion.
The participants were either studying at Taibah University, King Saud University, King Abdulaziz University, King Faisal University, Umm Al-Qura University, Imam Mohammad Ibn Saud Islamic University, Princess Nourah Bint Abdul Rahman University, University of Hail, Northern Border University, Taif University, Jazan University, or Albaha University or working at MOH or a private hospital in Saudi Arabia.
The sample size was calculated using the Raosoft online calculator with a 95% confidence level and a 5% margin of error.
Data collection
Participants were screened using an EAT-26 translated into Arabic. The EAT-26 is a widely used questionnaire tool for screening EDs that uses a 6-point Likert scale (always, usually, often, sometimes, rarely, never). The original version of the EAT-26 was published in 1982. A score above 20 indicates possible ED, 20–24 indicates mild ED, 25–30 indicates moderate to severe ED, and > 31 indicates very severe ED 24.
An electronic online questionnaire was distributed to the participants using Google Forms via different social media apps and consisted of three parts:1) consent form; 2) personal information (name, age, sex, province, college, academic level, weight, and height for a total of 14 questions); and 3) the translated EAT-26 (total of 32 questions). All questions in the surveys were mandatory, and subjects could not submit the questionnaire if any were left blank. The subjects were allowed to go back to a previous question, this survey has 3 screens 1 for each part . The participants could submit the completed questionnaire only once. The questionnaire was designed to take approximately 7 min to complete. Participation was voluntary and uncompensated.
All participants whose scores indicated EDs were included and diagnosed according to DSM-5 criteria.
Diagnostic criteria
The first screening tool, for indicating subjects with EDs was EAT-26 which is not a diagnostic tool it has been used to determine whether the subject had ED; however, this criterion only determines whether the person has an eating disorder but does not identify the type. The second diagnostic criterion is the DSM-5 diagnosis, which was used to identify the ED type (pica, rumination disorder, AFRID, AN, BN, BED, OSFED, and UFED) by calling the participants with ED and asking whether they had symptoms recorded in the DSM-5 to identify the type 25. Telephone calls were used because some participants had a time limit for the interview or were located in a different province.
Anthropometric measurements
Weight and height were self-measured and reported in the electronic questionnaire. The BMI of each participant was calculated using the Quetelet equation: BMI=(weight (kg))/(height (m²)) .
Dietary assessment
Dietary intake was estimated using twice-repeated 24-hour recall records collected by calling the participants with ED and asking them what they ate and drank the day before. The same procedure was performed a week later with a focus on energy. In addition, the following nutrients and macronutrients were recorded: [carbohydrates (g), protein (g), fat (g)] and micronutrients: [carbohydrates (g), protein (g), fat (g)] and micronutrients: [vitamin A (μg), thiamin (mg), riboflavin (mg), niacin (mg), pantothenic acid (mg), pyridoxine (mg), biotin (μg), folate (μg), cobalamin (μg), vitamin C (mg), vitamin D (μg), vitamin E (mg), vitamin K (μg), Ca (mg), Cr (μg), Cu (mg), F (mg), I (μg), Fe (mg), Mg (mg), Mn (mg), P (mg), K (mg), Na (mg), Se
(μg), and Zn (mg)]
Ethical considerations
Permission to conduct the current study was obtained from the local committee for biomedical ethics to conduct scientific research at Umm Al-Qura University. Participants provided their consent before the beginning of the project, and they were assured that all of their information would be kept private and that they had the right to withdraw from the study at any time.
Pretesting of questionnaires
The data collection tools were pretested electronically in 5 subjects who were not included in the study to confirm the clarity of the questions and any necessary changes before the main project was conducted.
Data analysis
Microsoft Excel was used to initially enter and analyze the data. The 24 recall records were analyzed using the food processor nutrition and fitness software ESHA Research version 11.9.13. The intake values were compared with the recommended dietary allowance (RDA) for energy, macronutrients, and micronutrients and obtained from the National Institutes of Health 26. Descriptive and inferential data were analyzed using (SPSS Statistics for Windows version 26; IBM ) used the frequencies descriptive to identify mean, and descriptive statistics, the significance of independent sample T-test, Pearson’s correlation and chi-square were used. The significance level was set at P ≤ 0.05.
Results
A total of 186 participants (14 men, and 172 women) were recruited from different provinces in Saudi Arabia. Two participants were excluded because they were not nutrition students or dietitians, while contact information was lost for nine participants. The final total number of participants included in the study was 175 (12 men, 163 women); thus, the completion rate was 94%. The mean participant age was 24.62 ± 4.7 years, the minimum age was 19 years, and the maximum age was 53 years, 24 participants were between 19–30 years of age and 3 participants were between 31–50 years old. Of the participants, 3.4% (n=6) were previously treated for an ED, while 96.6% had never been treated for an ED (n=169).
EAT-26 and DSM-5
According to the EAT-26, participants scoring ≥ 20 points were classified as having an ED. Accordingly, 27 participants (15.4%), including two men and 25 women, had ED, with a present age of 6.9% and 93.1% for men and women, respectively (Figure 1). Of all patients, 29.6% (n=8) had mild ED, 29.6% (n=8) had moderate to severe ED, and 40.7% (n=11) had very severe ED. The mean age of patients with ED was 24.96 ± 4 years.
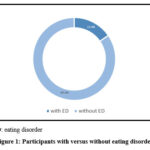 |
Figure 1: Participants with versus without eating disorders. |
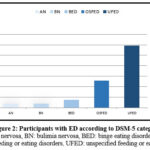 |
Figure 2: Participants with ED according to DSM-5 category |
One participant (3.7%) had AN, one (3.7%) had BN, two (7.4%) had BED, seven (25.9%) had OSFED, and 16 (59.3%) had UFED (Figure 2).
Regarding those with an ED, according to place of residence, 6 (22.2%) were from Eastern Province, 1 (3.7%) was from Hail province, 1 (3.7%) was from Jizan province, 5 (18.5%) were from Mecca province, 11 (40.7%) were from Medina province, and 3 (11.1) were from Riyadh province (Figure 3).
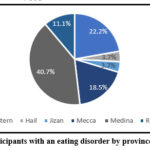 |
Figure 3: Participants with an eating disorder by province of residence |
Regarding participants’ academic level, five (18.5%) were in the fifth academic level, one (3.7%) in the seventh, two (7.4%) in the eighth, one (3.7%) was an intern, and 18 (66.7%) had graduated.
Anthropometric measurements
The anthropometric measurements of the subjects with versus without ED are shown in Table 1. The mean height was 159 ± 6.8 cm, mean weight was 59.6 ± 8.7 kg, and mean BMI was 23.6 ± 3.47 for participants with an ED. The mean height was 157 ±7.3 cm, the mean weight was 56.3 ± 17 kg, and the mean BMI was 22.8 ± 10 for participants without an ED. Hence, there were insignificant differences in weight, height, and BMI; the P values were 0.328, 0,388, and 0.696, respectively, for those with ED versus those without ED.
Moreover, the reference data of BMI categories indicated a higher prevalence of normal body weight among all participants with versus without ED than of underweight, overweight, and obese. There were significant differences the P values were 0.012 compared to those with and without ED (Tables 2).
Table 1: Anthropometric measurements of subjects with versus without an eating disorder (ED).
|
Variable |
Subjects with an ED |
Subjects without an ED |
P value |
|
Height (cm) |
159 ± 6.8 |
157 ± 7.3 |
0.388 |
|
Weight (kg) |
59.6 ± 8.7 |
56.3 ± 17 |
0.328 |
|
Body mass index (kg/m²) |
23.6 ± 3.47 |
22.8 ± 10 |
0.696 |
Values are shown as mean ± standard deviation.
Table 2: Body mass index (BMI) categories of subjects with and without eating disorders
|
|
subjects with eating disorders |
subjects without eating disorders |
P value |
||
|
BMI category |
No. |
% |
No. |
% |
|
|
Underweight Normal weight Overweight Obesity I Obesity II Obesity III |
1 19 5 2 0 0 |
3.7 70.4 18.5 7.4 0 |
30 83 22 11 1 1 |
20.3 56.1 14.9 7.4 0.7 0.7 |
0.012 |
Dietary assessment
Participants with an ED declared either a high or low intake of macro- and/or micronutrients based on their twice-repeated 24-hour dietary recall records. The consumption was less than the RDA for energy, carbohydrate, protein, fat, vitamins including A, D, E, C, B1, B2, B3, B5, B7, B9, and B12 and minerals including Ca, Cr, Cu, F, I, K, Mg, P, and Zn, and there was a slight reduction in the RDA for vitamin B6, K, and Se. However, the consumptions of Fe, Mn, and Na exceeded the RDA. There were insignificant and significant differences in macro- and micronutrients among those with ED (Tables 3 and 4).
Table 3: Macronutrient and vitamin intakes of participants with eating disorders
|
Nutrient |
Mean ± SD |
RDA |
% of RDA |
P value |
|
Energy (kcal) |
1358.2 ±661.6 |
2044 |
66.4 |
0.000 |
|
Carbohydrate (g) |
169.2 ±85.6 |
280.48 |
60.67 |
0.000 |
|
Protein (g) |
59.25 ±21.4 |
76.7 |
77.5 |
0.086 |
|
Fat (g) |
55.62 ±36.5 |
68.48 |
80.5 |
0.005 |
|
Vitamin A (μg) |
245.24 ±182.5 |
714.81 |
34.2 |
0.075 |
|
Vitamin B1 (mg) |
0.68 ±0.39 |
1.1 |
62.12 |
0.468 |
|
Vitamin B2 (mg) |
0.86 ±0.44 |
1.1 |
78 |
0.000 |
|
Vitamin B3 (mg) |
12.54 ±6.15 |
14.15 |
88.8 |
0.328 |
|
Vitamin B5 (mg) |
1.19 ±0.93 |
5 |
23.9 |
0.821 |
|
Vitamin B6 (mg) |
1.17 ±0.87 |
1.3 |
90.14 |
0.523 |
|
Vitamin B7 (μg) |
2.9 ±2.57 |
30 |
9.67 |
0.869 |
|
Vitamin B9 (μg) |
178.5 ±111.8 |
400 |
44.63 |
0.967 |
|
Vitamin B12 (μg) |
1.72 ±1.31 |
2.4 |
71.68 |
0.017 |
|
Vitamin C (mg) |
57.5 ±72.3 |
76.1 |
75.5 |
0.000 |
|
Vitamin D (μg) |
1.8 ±2.3 |
15 |
12 |
0.000 |
|
Vitamin E (mg) |
3.8 ±3.1 |
15 |
25.33 |
0.525 |
|
Vitamin K (μg) |
83 ±192.6 |
92.2 |
91.7 |
0.734 |
Results were taken from 24-hour recall records.
Table 4: Mineral intakes of participants with eating disorders
|
Nutrient |
Mean ± SD |
RDA |
% of RDA |
P value |
|
Ca (mg) |
683.9 ± 475 |
1000 |
68.4 |
0.011 |
|
Cr (μg) |
0.78 ± 0.82 |
25.74 |
3 |
0.456 |
|
Cu (mg) |
0.53 ± 0.28 |
900 |
59 |
0.142 |
|
F (mg) |
0.04 ± 0.08 |
3.07 |
1.36 |
0.543 |
|
I (μg) |
1.8 ± 1.6 |
150 |
0.8 |
0.509 |
|
Fe (mg) |
38 ± 154 |
17.26 |
216 |
0.000 |
|
Mg (mg) |
137.37 ± 74.3 |
317.78 |
43.56 |
0.000 |
|
Mn (mg) |
4.42 ± 17.4 |
1.8 |
244.9 |
0.971 |
|
P (mg) |
617.4 ± 323.4 |
700 |
88.2 |
0.000 |
|
K (mg) |
1543 ± 620.6 |
2659.26 |
58.2 |
0.113 |
|
Na (mg) |
2421.3 ± 995.6 |
1500 |
161.4 |
0.685 |
|
Se (μg) |
52 ± 21.8 |
55 |
94.5 |
0.212 |
|
Zn (mg) |
4.6 ± 2.2 |
8.22 |
56.5 |
0.001 |
Results were taken from the 24-hour recall records.
Correlations between EAT-26 scores and nutrient intakes.
The obtained data showed significant correlations for ED parameters according to EAT-26 scores. There was a significant correlation between EAT-26 score and energy (P = 0.005), carbohydrate (P = 0.009), vitamin B2 (P = 0.025), vitamin B12 (P = 0.001), vitamin D (P = 0.003), Ca (P = 0.032), Fe (P = 0.000), Mg (P = 0.005), P (P = 0.001), and Zn (P = 0.001) consumption (Table 6). Meanwhile, there was no significant correlation between EAT-26 scores and protein (P = 0.268), fat (P = 0.052), vitamin B9 (P = 0.396), and vitamin C (P = 0.368) consumption (Table 5).
Table 5: Significant and insignificant correlations between Eating Attitudes Test – 26 item (EAT-26) score and nutrient intake
|
Parameter |
Nutrient intake |
P value |
Pearson correlation |
|
EAT-26 score |
Energy |
0.005 |
.527 |
|
Carbohydrate |
0.009 |
.494 |
|
|
Protein |
0.268 |
0.221 |
|
|
Fat |
0.052 |
0.379 |
|
|
Vitamin B2 |
0.025 |
.431 |
|
|
Vitamin B9 |
0.396 |
0.170 |
|
|
Vitamin B12 |
0.001 |
.584 |
|
|
Vitamin C |
0.368 |
0.181 |
|
|
Vitamin D |
0.003 |
.557 |
|
|
Ca |
0.032 |
.414 |
|
|
Fe |
0.000 |
.737 |
|
|
Mg |
0.005 |
.527 |
|
|
P |
0.001 |
.596 |
|
|
Zn |
0.003 |
.544 |
Discussion
The investigation aimed to study the prevalence of EDs by assessing the nutritional status of nutrition students and dietitians among multiple provinces in Saudi Arabia.
Prevalence of eating disorders
Our results showed that more females than males had EDs, partially because there are fewer male dietitians than female dieticians in Saudi Arabia, which agreed with a previous study reporting that 15.6% versus 84.4% of male versus female nutrition students (N = 147), respectively, had an ED 22. In the present study, EDs were more prevalent among individuals 19–30 years of age and less prevalent in 31–50-year-olds, among whom only three participants were affected by an ED, whereas no individuals aged >50 years old had an ED. The mean age of individuals with an ED was 24.96 years, similar to that of a previous study reporting a mean age of 22.5 years for students versus 31.2 years for dietitians 23. Meanwhile, 3.4% were previously treated for an ED versus 8.2% of the 636 participants of a previous study 21.
In our study, the prevalence was higher for OSFED and UFED than for other EDs. A similar study conducted in Brazil of 745 female participants showed an ED prevalence of 9.10%; it included only females because more than 90% of dietitians in Brazil are female 23. A previous study of 147 students in the United States reported an ED prevalence of 9.5% 22. Meanwhile, another study of 97 nutrition students in Australia reported an ED prevalence of 14.5% 27. Another study in Australia of 137 nutrition students and dietitians reported an ED prevalence of 13.25% 28. A study in Wisconsin, USA, of 35 participants reported an ED prevalence of 22.2% for nutrition students and dietitians 29. Furthermore, the ED rate variance among studies reflected the difference in ED prevalence among nutrition students and dietitians concerning geographic regions worldwide, which might have been due to differences in socioeconomic status and knowledge about EDs that could affect and lead to EDs. Notably, all studies used the EAT-26 to assess subjects for EDs.
According to our data, EDs were more prevalent (40.7%) in Medina province despite the equal percentage of participants from Medina and Mecca provinces. Moreover, the ED rate was high (22.2%) in the Eastern province compared to the number of participants included. Some provinces did not declare EDs because the number of participants was small compared with the total population in other provinces. Two of the provinces (Al-Jowf and Najran) were not included in the study because no participants within them completed the questionnaire, and only one participant was included from Asser Province. In other provinces, the study did not detect any cases of EDs, and slightly fewer participants completed the questionnaire. Further research is required to include more participants from provinces with lower sample numbers.
A study in Brazil disagreed with our findings; it reported a total of 43 students and 25 dieticians with an ED versus our 9 students and 18 dietitians 23. In the present study, among those students with an ED, five were in their third academic year, four were in their fourth year, and none were reported in their first or second academic year. In another study, four participants were in their first or second academic year while 10 were in their third or fourth academic year 22 . However, with the study’s small sample size, it is difficult to draw definitive conclusions.
Our data demonstrated a BN rate of 3.7% and a BED rate of 7.4%. In Australia, a 23% BN prevalence was reported 27; and in Brazil, among 179 nutrition students, the BN rate was reportedly 6.1%, while that of BED was 2.8% 30. Unfortunately, no study cited rates of AN, OSFED, or UFED among nutrition students and dietitians.
Anthropometric measurements
Our study demonstrated that participants with EDs had a normal BMI (mean, 23.6 kg/m2). Only one patient was underweight, 19 were normal weight, five were overweight, and two were obese (Table 2). A study in the United States revealed that the mean BMI was within the underweight/normal classification in 11 cases versus overweight or obese in two cases 18. According to a study in Australia, the average BMI of individuals with EDs was normal (22.7 kg/m2) 28.
Dietary assessment
Patients with EDs were more susceptible to nutrient deficiencies. The present study revealed that most participants had an inadequate diet, and the average intakes of energy, macronutrients (carbohydrate, protein, and fat), energy, and macronutrients were below the RDA (energy, 1358.2 kcal; carbohydrate, 169.2 g; protein, 59.25 g; and fat, 55.62 g). A previous study 31 reported the following intakes for ON (Orthorexia Nervosa) respondents: energy, 25.5 kcal/kg; carbohydrate, 195.3 g; protein, 66.8 g; and fat, 69.7 g. These values are below the RDA for energy, carbohydrate, and protein and within the RDA for fat. They also included one micronutrient – Na – at a mean intake of 2260.4 mg (i.e., higher than the RDA). In our study, the Na intake was 2421.3 mg (i.e., higher than the RDA). Unfortunately, no study investigated other nutrients, and research has yet to include all types of EDs and macro plus micronutrient intakes among nutrition students and dietitians. Here we found significant differences between EAT-26 scores and energy and carbohydrate intakes and insignificant differences between EAT-26 scores and protein and fat intakes.
Strength and Limitations
This study has some limitations. It used an online self-report questionnaire and had a low number of participants. However, owing to limited time and resources, it was not possible to include larger numbers of nutrition students and dietitians. Biomarkers may have enabled strong inferences regarding the results of the current study. Thus, further studies are necessary that include biochemical analyses. This is a descriptive cross-sectional study. The strength of our study is that it is the first in Saudi Arabia to investigate the prevalence of EDs among nutrition students and dietitians.
Conclusion
Our investigation concluded that the prevalence of EDs in Saudi Arabia is 15.4% among nutrition students and dietitians. The documented EDs included high numbers of OSFED and UFED cases. Moreover, EDs are more prevalent in some provinces of Saudi Arabia. Intakes of energy, macronutrients, and some micronutrients were low, while those of other micronutrients were higher than the RDA.
Acknowledgment
The authors would like to thank the Deanship of Scientific Research at Umm Al-Qura University for supporting this work by Grant Code: (22UQU4330031DSR01). Moreover, the authors offer many thanks to the current study’s participants, without whom this work would not have been possible. We would like to thank Editage (www.editage.com) for English language editing.
Conflict of Interest
The author(s) declares no conflict of interest.
Funding Sources
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
- Gaines, Stacey A and Burnett, Taylor Beth S. 2014 Perceptions of Eating Behaviors, Body Image, and Social Pressures in Female Division II College Athletes and Non-Athletes. Journal of Sport Behavior; 37 (4): 351-369
- Dell’Osso, L., Abelli, M., Carpita, B., Pini, S., Castellini, G., Carmassi, C., & Ricca, V. (2016). Historical evolution of the concept of anorexia nervosa and relationships with orthorexia nervosa, autism, and obsessive-compulsive spectrum. Neuropsychiatric disease and treatment, 12, 1651–1660. https://doi.org/10.2147/NDT.S108912.
CrossRef - Harrington BC, Jimerson M, Haxton C, Jimerson DC. Initial evaluation, diagnosis, and treatment of anorexia nervosa and bulimia nervosa. Am Fam Physician. 2015 Jan 01;91(1):46-52. [PubMed]
- McCuen-Wurst, C., Ruggieri, M. and Allison, K. 2018. Disordered eating and obesity: associations between binge-eating disorder, night-eating syndrome, and weight-related comorbidities. Annals of the New York Academy of Sciences,. 1411(1):.96-105.
CrossRef - NEDA Team. PICA. 2021. nationaleatingdisorders.org. Available at: https://www.nationaleatingdisorders.org/learn/by-eating-disorder/other/pica.
- Peckham, A. 2021. Rumination disorder: Definition, symptoms, treatment, and more.. Medicalnewstoday.com. Available at: https://www.medicalnewstoday.com/articles/rumination-disorder.
- NEDA Team. 2021. AVOIDANT RESTRICTIVE FOOD INTAKE DISORDER (ARFID).. nationaleatingdisorders.org. Available at: https://www.nationaleatingdisorders.org/learn/by-eating-disorder/arfid.
- Riesco, N., Agüera, Z., Granero, R., Jiménez-Murcia, S., Menchón, J. and Fernández-Aranda, F. 2018. Other Specified Feeding or eating disorders (OSFED): Clinical heterogeneity and cognitive-behavioral therapy outcome. European Psychiatry,. 54, pp.109-116. Available at: https://pubmed.ncbi.nlm.nih.gov/30193141/.
CrossRef - Gkiouleka, M., Stavraki, C., Sergentanis, T. and Vassilakou, T. 2022. Orthorexia Nervosa in Adolescents and Young Adults: A Literature Review. Children,. 9(3), p.365. Available at: https://www.mdpi.com/2227-9067/9/3/365/htm.
CrossRef - Barnard, Neal D. 2018. “Eating Disorders.” Nutrition Guide for Clinicians. 3rd ed., Physicians Committee for Responsible Medicine, nutritionguide.pcrm.org/nutritionguide/view/Nutrition_Guide_for_Clinicians/1342074/all/Eating_Disorders.
- Scribner, C. 2016. Understanding Nutritional Needs of Patients with Eating Disorders: Implications for Psychiatrists.. Psychiatric Times. Volume 33 , No, 4. Available at: https://www.psychiatrictimes.com/ view/understanding-nutritional-needs-patients-eating-disorders-implications-psychiatrists.
- Kaye, W. 2018. Health Consequences. National Eating Disorders Association.. Available at: https://www.nationaleatingdisorders.org/ health-consequences.
- Chidiac, C. 2019. An update on the medical consequences of anorexia nervosa. Current Opinion in Pediatrics,. 31(4), pp.448-453.
CrossRef - Gibson, D., Workman, C. and Mehler, P. 2019. Medical Complications of Anorexia Nervosa and Bulimia Nervosa. Psychiatric Clinics of North America,. 42(2), pp.263-274. Available at: https://pubmed.ncbi.nlm.nih. gov/ 31046928/.
CrossRef - Wassenaar, E., Friedman, J. and Mehler, P. 2019. Medical Complications of Binge Eating Disorder. Psychiatric Clinics of North America,. 42(2), pp.275-286. Available at: https://linkinghub.elsevier.com/retrieve/ pii/S0193953X19300152.
CrossRef - Lindvall Dahlgren, C., Wisting, L. and Rø, Ø. 2017. Feeding and eating disorders in the DSM-5 era: a systematic review of prevalence rates in non-clinical male and female samples. Journal of Eating Disorders,. 5(1), pp.5-7. Available at: https://jeatdisord.biomedcentral.com/ articles/10.1186/s40337-017-0186-7.
CrossRef - Melisse, B., de Beurs, E. and van Furth, E. 2020. Eating disorders in the Arab world: a literature review. Journal of Eating Disorders, 8(1), pp.1-19. Available at: https://jeatdisord.biomedcentral.com/ articles/10.1186/s40337-020-00336-x.
CrossRef - Fatima, W., Fatima, R. and Anwar, N. 2018. Prevalence of Eating Disorders among Female College Students of Northern Broader University, Arar, Kingdom of Saudi Arabia. International Journal of Child Health and Nutrition,. 7(3), pp.115-121. Available at: https://www.researchgate.net/publication/339617424_Kingdom_of_Saudi_Arabia.
CrossRef - El-Azeem Taha, A., Abu-Zaid, H. and El-Sayed Desouky, D. 2018. Eating Disorders Among Female Students of Taif University, Saudi Arabia. Archives of Iranian medicine,. 21(3), pp.111-117. Available at: https://pubmed.ncbi.nlm.nih.gov/29688736/.
- Alwosaifer, A., Alawadh, S., Abdel Wahab, M., Boubshait, L. and Almutairi, B.. 2018. Eating disorders and associated risk factors among Imam Abdulrahman bin Faisal university preparatory year female students in Kingdom of Saudi Arabia. Saudi Medical Journal,. 39(9), pp.910-921. Available at: https://www.ncbi.nlm.nih.gov/pmc/ articles/PMC6201000/.
CrossRef - Tremelling, K., Sandon, L., Vega, G. and McAdams, C. 2017. Orthorexia Nervosa and Eating Disorder Symptoms in Registered Dietitian Nutritionists in the United States. Journal of the Academy of Nutrition and Dietetics,. 117(10), pp.1612-1617. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5623148/.
CrossRef - Yu, Z. and Tan, M.. 2016. Disordered Eating Behaviors and Food Addiction among Nutrition Major College Students. Nutrients,. 8(11), p.673. Available at: https://pubmed.ncbi.nlm.nih.gov/27792162/.
CrossRef - Toral, N., Gubert, M., Spaniol, A. and Monteiro, R.. 2016. Eating disorders and body image satisfaction among Brazilian undergraduate nutrition students and dietitians. Archivos latinoamericanos de nutricion. 66(2), pp.129-134. Available at: https://pubmed.ncbi. nlm.nih.gov/29737669/.
- Garner, D., Olmsted, M., Bohr, Y. and Garfinkel, P. 1982. The Eating Attitudes Test: psychometric features and clinical correlates. Psychological Medicine. 12(4), pp.871-878.
CrossRef - Benson, S., Young, S., Akaka, J., Bernstein, C., Crowley, B., Everett, A. 2013. Diagnostic and statistical manual of mental disorders. 5th ed. Arlington: American Psychiatric Publishing. pp.329-354.
- Stallings, V., Harrison, M. and Oria, M. 2019. Dietary Reference Intakes for Sodium and Potassium. Washington, DC: National Academies Press,. pp.565-577.
CrossRef - Rocks, T., Pelly, F., Slater, G. and Martin, L. 2017. Prevalence of Exercise Addiction Symptomology and Disordered Eating in Australian Students Studying Nutrition and Dietetics. Journal of the Academy of Nutrition and Dietetics. 117(10), pp.1628-1636.
CrossRef - Rocks, T., Pelly, F., Slater, G. and Martin, L. 2017. Eating attitudes and behaviours of students enrolled in undergraduate nutrition and dietetics degrees. Nutrition & Dietetics. 74(4), pp.381-387.
CrossRef - Woehrer, K. 2018. Prevalence of Eating Disorders Tendencies, Disordered Eating, and Orthorexia Nervosa Behaviors in Dietetic-Nutrition Students Compared to Biology Students. University of Wisconsin–Stout,. pp.1-42.
- de Moraes, C., Appolinário, J., Mourilhe, C., de Freitas, S. and da Veiga, G. 2021. Reliability of the Brazilian version of the questionnaire on eating and weight patterns-5 (QEWP-5). Eating and Weight Disorders – Studies on Anorexia, Bulimia and Obesity,. 26(3), pp.1-8. Available at: https://link.springer.com/article/10.1007%2Fs40519-020-01072-6.
CrossRef - Grammatikopoulou, M., Gkiouras, K., Markaki, A., Theodoridis, X., Tsakiri, V., Mavridis. 2018. Food addiction, orthorexia, and food-related stress among dietetics students. Eating and Weight Disorders – Studies on Anorexia, Bulimia and Obesity. 23(4), pp.459-467. Available at: https://link.springer.com/article/10.1007/s40519-018-0514-1.
CrossRef
List of Abbreviations
AN, anorexia nervosa
ARFID, avoidant/restrictive food intake disorder
BED, binge eating disorder
BMI, body mass index
BN, bulimia nervosa
DSM-5, Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition
EAT-26, Eating Attitudes Test – 26 item
EDNOS, eating disorder not otherwise specified
EDs, eating disorders
OR, orthorexia nervosa
OSFED, other specified feeding or eating disorders
RDA, Recommended Dietary Allowance
UFED, unspecified feeding or eating disorder
Accepted on: 01 Feb 2024
Second Review by: L.I. Krasnova
Final Approval by: Dr. Neha Sanwalka





Web of Science Coverage
Emerging Sources Citation Index (ESCI)
2024 Journal Impact Factor: 1.1
Scopus Journal Metrics
CiteScore 2025: 2.6
CiteScore Details
Sustainable Nutrition: Food Systems, Nutrient Retention, and Public Health Impact
![]()
This journal is a member of, and subscribes to the principles of, the Committee on Publication Ethics (COPE)








