Diabetes Knowledge, Practices, and Risk Perception among Saudi University Students: Insights from a Cross-Sectional Study
 , Sumia Mohammed Enani2, Albandari Abdullah Bin Ammar3, Howeida Hassan Abusalih1, Amal Hamdi Kenanah4, Alaa Jameel Almiman5, Abdulrahman Ahmed Alsayegh6 and Abeer Salman Alzaben1
, Sumia Mohammed Enani2, Albandari Abdullah Bin Ammar3, Howeida Hassan Abusalih1, Amal Hamdi Kenanah4, Alaa Jameel Almiman5, Abdulrahman Ahmed Alsayegh6 and Abeer Salman Alzaben1 1Department of Health Sciences, College of Health and Rehabilitation Sciences, Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
2Faculty of Human Sciences and Design, Department of Food and Nutrition, King Abdulaziz University, Jeddah, Saudi Arabia.
3Department of Clinical Nutrition, College of Applied Medical Sciences, Ha’il University, Ha’il, Saudi Arabia.
4Department of General Studies, College of Humanities and Sciences, Prince Sultan University, Riyadh, Saudi Arabia.
5Department of Community Health Science, College of Applied Science, King Saud University, Riyadh, Saudi Arabia.
6Department of Clinical Nutrition, College of Nursing and Health Sciences, Jazan University, Jazan, Saudi Arabia.
Corresponding Author E-mail:NMBawazeer@pnu.edu.sa
DOI : http://dx.doi.org/10.12944/CRNFSJ.13.2.12
Download this article as:
![]()
Type 2 diabetes is an escalating concern among youth. This research aimed to evaluate university students' knowledge about diabetes, their health-related practices, and perceived risks of developing the disease in Saudi Arabia. An online cross-sectional survey was carried out between February 2021 and December 2022, targeting students from all academic levels. Sociodemographic data, diabetes history, and lifestyle factors were collected using a validated questionnaire assessing diabetes knowledge, practices, and perceived risk. Among 1,312 participants, 66% were female, 42% were in their first year, and 60% had a family history of diabetes. Dietary knowledge received the lowest scores, and there were gaps in seeking information from healthcare professionals and following diabetes-related news. Overall, 83% of students had low to moderate diabetes knowledge, 54% exhibited neutral health practices, and 44.6% perceived themselves as high risk of developing diabetes. Factors significantly associated with diabetes knowledge and practices included age, education, family history, and workshop participation (p < 0.05). Regression analysis revealed that education level and knowledge explained 10.3% of the variance in diabetes-related practices (p < 0.001). In conclusion, University students demonstrated low to moderate diabetes knowledge and neutral health practices, particularly regarding diet and information-seeking behaviors. Public education initiatives tailored for university students are critical to improving diabetes prevention behaviors and promoting healthy lifestyles.
KEYWORDS:Diabetes awareness; Health behavior; Preventive practices; Risk factors; Saudi Arabia; Type 2 diabetes; University students
Introduction
Type 2 diabetes (T2D) is defined as the inability of the body to metabolize blood glucose for energy.1 It is the most prevalent type of diabetes worldwide and is widely considered a disease of the older population. However, it is now more commonly diagnosed in younger populations, including adolescents.2 According to the Centers for Disease Control and Prevention in the United States, T2D is an increasing threat among the young, with one in four individuals aged 19–34 years having prediabetes, a key risk factor for developing T2D.3 Furthermore, 0.46 cases per 1,000 have been reported among those under 20 years of age.4 This prevalence of T2D has been linked to the global incidence of childhood obesity.5 An inverse association has been observed between body mass index and age at onset of T2D, with severe weight gain in those aged < 40 years presenting a higher risk of T2D.6 The disease progresses more rapidly in youth compared to adults, with higher risks of morbidity and mortality observed in this highly productive age group.7
The major predisposing risk factors for T2D are a family history of diabetes, sedentary lifestyle, obesity or overweight, and ethnicity.2
Saudi Arabia (SA) is among the top 10 countries with the highest prevalence of T2D.2 A study reported that 25% of the total population of SA has diabetes.8 The prevalence of diabetes and impaired fasting glucose is higher in children and adolescents in SA compared to the international figures, with > 90% of individuals being unaware of their disease.9 A healthy lifestyle and eating habits, as well as regular physical activity within the entire family, should be considered to reduce obesity rates, improve quality of life, and control disease-related secondary morbidity.10, 11
Public awareness of diabetes and its risk factors is crucial for decreasing disease incidence, yet only a few studies have assessed the level of knowledge of diabetes and its risk factors among young adults. Two national studies identified a significant lack of public awareness regarding diabetes and its associated complications.12, 13 As of 2019, only 27 out of 60 Saudi citizens reported adhering to the Saudi Dietary Guidelines, which the Saudi Ministry of Health developed to promote balanced nutrition and prevent chronic diseases, such as cardiovascular diseases. These guidelines emphasize the importance of consuming a variety of food groups in appropriate portions and limiting saturated fats, added sugars, and salt.14 Furthermore, salt intake in SA exceeds the recommended level,15 and the consumption of sugar-sweetened canned beverages by overweight Saudi women has been found to be associated with insulin resistance.16
Therefore, given the rising prevalence of diabetes among the young population, this study aimed to evaluate university students’ knowledge of diabetes, their health-related practices, and their perceptions of personal risk for developing the condition. Such an assessment has the potential to reduce disease morbidity and mortality by informing the development of targeted programs that enhance awareness of diabetes and its risk factors. Additionally, the associations between diabetes knowledge, perceived risk, and health practices were explored, considering sociodemographic variables, diabetes history, and lifestyle factors among university students.
Materials and Methods
Study design and methods
An online cross-sectional survey was carried out between February 2021 and December 2022 using an online survey. The inclusion criteria were male and female students registered at Saudi Arabian universities at all academic levels who were available during the data collection period. The exclusion criteria were students who could not read Arabic or who had other medical conditions, such as celiac disease or liver disease. Participants were recruited from different universities in SA based on communication with faculty members who expressed their desire to participate in data collection. The students included in this study were from the following institutions: King Saud University and Prince Sultan University in Riyadh, King Faisal University in Hofuf, Jazan University in Jazan, King Abdulaziz University in Jeddah, and Hail University in Hail.
Ethical approval was granted by the Institutional Review Board (IRB) of Princess Nourah bint Abdulrahman University (21-0013, dated 10 January 2021). Permission for data collection was obtained from the deans of the participating institutions. Students who agreed to participate were asked to complete the questionnaire. Participation was voluntary, and the participants had the option to decline to take part in the survey. Consent was provided by participants clicking on the ‘I agree’ button on the digital questionnaire.
Convenience sampling was employed, and the study sample was obtained by assisting a researcher in reaching out to students at the universities. This strategy involved using university email systems to communicate with students and, when necessary, engaging in personal communication with select individuals to facilitate their participation. There were no restrictions based on demographic factors, such as age, sex, religion, field of study, or specialization. The minimum sample size was justified based on a previous study,17 which recommended an ideal ratio of 10 participants per item for adequate statistical analysis. Accordingly, a minimum 320 participants were required to correspond with 32 items of the study instrument. The final sample size of 1312 participants significantly exceeded this minimum, thereby enhancing statistical power, improving the precision of estimates, and increasing the generalizability of the findings. This larger sample allows for more robust analyses, facilitates the detection of subtle effects, and provides a more representative understanding of the target population, ultimately strengthening the reliability and validity of the study’s conclusions. The response rate was 100%, with no incomplete responses.
Data Collection Tool
An online, self-administered questionnaire was designed using Google Forms to collect information from the participants. The questionnaire included various sections to capture relevant data and was distributed via email to students at the participating universities. Participants accessed the survey through a secure link provided in the email, ensuring anonymity and confidentiality. First, the requested sociodemographic information included age, sex, and educational level (academic year). The diabetes history included questions related to the students’ family history of diabetes and their diagnosis of diabetes. Regarding lifestyle history, questions about the students’ levels of physical activity, smoking status, and specific nutrition regimens were asked. Other questions probed whether the students had attended or actively participated in any educational sessions about diabetes (e.g., lectures, workshops, or receipt of educational materials), whether their blood glucose levels had ever been checked, and whether the students knew how an individual develops diabetes.
A previously developed questionnaire, used among university students in Saudi Arabia who met the same inclusion criteria as those in the current study, was identified and utilized to assess diabetes knowledge, health practices, and risk perceptions as part of a diabetes awareness program.18 This questionnaire, validated by Khlaifat et al. (2020), consists of three sections, each focusing on different aspects of diabetes knowledge and awareness.19 To further ensure the content validity, relevance, and appropriateness of the questionnaire for the study’s target population and objectives, a content validation process was undertaken. A panel of three experts—comprising registered dietitians, nutritionists, and public health researchers—independently evaluated the relevance of each of the 32 items. The Item Content Validity Index (I-CVI) was calculated, yielding an overall score of 0.88, indicating a high degree of content validity. The first section assessed the participants’ knowledge of diabetes using 22 questions about diet, physical activity, overweight, the definition of diabetes, commonly used medications, signs and symptoms, and diabetes complications. These questions included 14 questions to which the participants could respond with ‘true’, ‘false,’ or ‘do not know,’ as well as 8 multiple-choice questions for which the participants could choose only one answer. The questions in this section were scored as follows: ‘true’ responses were given one point, and ‘false’ and ‘do not know’ responses received a zero. The potential sum of the scores ranged from 0–22. A high score reflected the highest level of knowledge about diabetes. Knowledge was categorized into three groups: 0–49% (0 to < 11 correct answers) indicated a low level of knowledge about diabetes, 50–74% (11 to < 17 correct answers) indicated a moderate level of knowledge, and 75–100% (17–22 correct answers) indicated a high level of knowledge.
The second section of the questionnaire assessed students’ health practices using seven multiple-choice questions. The participants were asked to rank their responses according to a four-point Likert scale (4 = always, 3 = sometimes, 2 = rarely, and 1 = never). The total practice scores ranged from 7–28, with specific score ranges indicating levels of diabetes practices: scores between 7–14 were categorized as indicating poor practice, scores from 15–21 were considered neutral practice, and scores between 22–28 represented good practice. The specific behaviors assessed included exercising, maintaining a balanced diet, consulting health practitioners, adopting healthy lifestyle changes, considering lifestyle changes to reduce the possibility of diabetes, monitoring weight, and staying informed about diabetes. These items aimed to evaluate participants’ awareness of and proactive measures regarding diabetes prevention.
Finally, the third section of the questionnaire assessed students’ perceptions of their own risk of developing diabetes through three statements: “My assessment of the possible risk that I will develop diabetes,” “My assessment of diabetes and its impact on health,” and “My assessment of the impact of diabetes on people of my age.” Participants evaluated their perceptions based on their understanding of diabetes risk factors and selected one of the following response options: high risk, moderate risk, low risk, or not influential. For the analysis, the moderate and high-risk responses were combined and categorized into a single ‘high-risk’ category.20
Statistical analysis
Data analysis was performed using the Statistical Package for the Social Sciences version 21 (IBM Corp., New York, United States). A p-value of less than 0.05 was considered statistically significance. Descriptive statistics were reported as frequencies, percentages, means, and standard deviations (SD), as applicable. The association between the students’ knowledge of diabetes and their health practices, in relation to sociodemographic characteristics, diabetes history, and lifestyle factors, as well as the association between the students’ diabetes knowledge, health-related practices, and risk perception, were assessed using a chi-square test. A simple linear regression model was used to investigate the association between knowledge scores, education levels, and health-related practices. The model summary and ANOVA table provide an overview of the overall model fit. The correlation coefficient (R) reflects the strength of the association between the independent variables (knowledge score and education) and the dependent variable (health-related practices). The coefficient of determination (R²) quantifies the proportion of variance in health-related practices accounted for by the combined influence of knowledge scores and education. The F-statistic assesses the joint impact of knowledge scores and education on health-related practices, with significance determined at a p-value of 0.05.
Results
Sociodemographic variables, diabetes history, and lifestyle characteristics
Table 1 shows the sociodemographic characteristics, diabetes history, and lifestyle practices of the study population (n = 1,312 students). Most students were female and in their first year of study. A majority reported being physically active and nonsmokers, with over half having a family history of diabetes. While many were aware of how diabetes develops, fewer had attended educational events on the topic. Social media was the most common source of diabetes information, followed by informal and healthcare-related sources.
Table 1: Sociodemographic variables, diabetes history, and lifestyle characteristics of the study participants (n = 1,312).
|
Characteristics |
n (%) |
|
Age (years) |
|
|
18–22 |
1,039 (79.3%) |
| > 23 |
270 (20.7%) |
|
Gender |
|
|
Male |
445 (34%) |
| Female |
867 (66%) |
|
Education (academic year) |
|
|
First |
546 (41.6%) |
| Second |
225 (17.1%) |
|
Third |
172 (13.1%) |
| Fourth |
204 (15.5%) |
|
Fifth |
165 (12.6%) |
|
Follow a specific nutrition regimen |
|
|
Yes |
229 (17.5%) |
| No |
1,083 (82.5%) |
|
Frequency of physical activity |
|
| 1–2 times/week |
547 (42%) |
|
3–4 times/week |
261 (20%) |
| 5+ times/week |
158 (12%) |
|
I do not exercise |
346 (26%) |
|
Multivitamins supplements |
|
| Yes |
238 (18%) |
|
No |
1,074 (82%) |
|
Smoking status |
|
| Smoker |
140 (11%) |
|
Nonsmoker |
1,119 (85%) |
| Previous smoker |
53 (4%) |
|
Have diabetes |
|
|
Yes, T2D |
17 (1.3%) |
| Yes, T1D |
44 (3.4%) |
|
No |
1,147 (87.4%) |
| Not sure |
104 (7.9%) |
|
History of diabetes |
|
|
First-degree relatives |
418 (32%) |
| Second-degree relatives
No history of diabetes |
365 (28%) 529 (40%) |
|
Ever check your blood sugar |
|
|
Yes |
715 (54.5%) |
| No |
597 (45.5%) |
|
Attend a diabetes workshop or lecture, or read about diabetes |
|
|
Yes |
450 (34%) |
| No |
862 (66%) |
|
Have information on how a person gets diabetes |
|
|
Yes |
910 (69%) |
| No |
402 (31%) |
|
If the answer is yes, what is the source of this information? |
|
|
Television |
16 (1.8%) |
| Physicians |
158 (17.7%) |
|
Friends/relatives |
259 (29%) |
| Nurses/specialists |
164 (18.3%) |
|
Social media |
297 (33.2%) |
Knowledge, practices, and risk perceptions related to diabetes
Figure 1 illustrates the distribution of the study participants’ diabetes knowledge scores, health-related practices, and self-perception of their risk for developing diabetes. Among the university students, 41.1%, 41.8%, and 17.1% demonstrated low, moderate, and high levels of diabetes-related knowledge, respectively. The majority of students exhibited neutral practices toward diabetes (53.9%), while only 22.2% reported engaging in behaviors aimed at preventing diabetes. Additionally, 44.6% of students perceived themselves to be at high risk of developing diabetes.
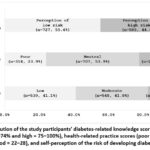 |
Figure 1: Distribution of the study participants’ diabetes-related knowledge scores (low = 0–49%, moderate = 50–74% and high = 75–100%), health-related practice scores (poor = 7–14, neutral = 15–21 and good = 22–28), and self-perception of the risk of developing diabetes (n = 1,312). |
The participants’ responses to the questions regarding their diabetes knowledge and lifestyle practices are presented in Table 2 and Figure 2. The diabetes-related knowledge questions were categorized into diet, physical activity, overweight, medication, general diabetes knowledge, and diabetes complications. The table reports the number and percentage of correct answers. Among the assessed categories, diet received the lowest score, suggesting a potential gap in knowledge in this area. Furthermore, the mean and standard deviation of the health practice items indicated insufficient practices, particularly in obtaining information about diabetes from healthcare practitioners (1.93 ± 1.0) and following diabetes-related news (2.21 ± 1.06).
Table 2: The participants’ responses to the questions related to diabetes-related knowledge item scores.
|
Diabetes-related |
Correct
answers, n (%) |
Incorrect answers, n (%) |
Don’t know answers, n (%) |
| Diet |
|
||
|
No need to organize the (wrong statement) |
972 (74.1) | 78 (5.9) | 262 (20.0) |
| Spread the food intake across multiple meals in DM |
557(42.5) | 775 (57.5) |
– |
|
Reason for recommending |
327 (24.9) | 985 (75.1) | – |
| Foods can be eaten without limitations in DM |
566 (43.1) | 746 (56.9) |
– |
|
Highest amount of energy foods |
285 (21.7) | 1,027 (78.3) | – |
| Reason for preferred using olive oil over ghee and butter in DM |
558 (42.5) | 335 (25.5) |
419 (32.0) |
|
Medication |
|||
| Oral diabetes medications are insulin tablets form (wrong statement) |
398 (30.3) | 406 (30.9) |
508 (38.7) |
|
Insulin dose must be adjusted |
942 (71.8) | 42 (3.2) | 328 (25.0) |
| Diabetics on medication do not need to engage in physical activity (wrong statement) |
897 (68.4) | 77 (5.9) |
338 (25.8) |
|
Diabetes complications |
|||
| Increase blood sugar level may harm body organs e.g. eyes and kidneys (correct statement) |
850 (64.8) | 70 (5.3) |
392 (29.9) |
|
Increase the level of blood |
343 (26.1) | 304 (23.2) | 665 (50.7) |
| Cause of reduced pain sensitivity in diabetic foot injuries. |
932 (71.0) | 305 (23.2) |
305 (23.2) |
|
Physical activity |
|||
|
Physical inactivity contributes |
966 (73.6) | 115 (8.8) |
231 (17.6) |
| Daily walking increases the level of blood sugar in DM (wrong statement) |
895 (68.2) | 99 (7.5) |
318 (24.2) |
|
Daily walking increases |
664 (50.6) | 126 (9.6) | 522 (38.9) |
| Overweight |
|
||
|
weight loss helps manage DM |
1,101 (83.9) | 35 (2.7) | 176 (13.4) |
| General diabetes knowledge |
|
||
|
Blood sugar levels are |
326 (24.9) | 508 (38.7) | 478 (36.4) |
| DM involves the body’s inability to respond to insulin (correct statement) |
668 (50.9) | 270 (20.6) |
374 (28.5) |
|
DM is a non-infectious |
1,158 (88.3) | 56 (4.3) | 98 (7.5) |
| DM is incurable (correct statement) |
581 (44.3) | 471 (35.9) |
260 (19.8) |
|
Healthy eating and regular |
821 (62.6) | 89 (6.8) | 402 (30.6) |
| Normal levels of fasting blood sugar in DM. |
678 (51.7) | 203 (15.5) |
431 (32.8) |
Abbreviations: DM, Diabetes Mellitus
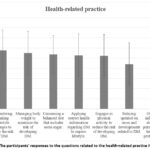 |
Figure 2: The participants’ responses to the questions related to the health-related practice item scores. |
Comparison of knowledge, practices, and risk perceptions related to diabetes across sociodemographic variables, diabetes history, and lifestyle variables
Tables 3 and 4 present comparisons of diabetes-related knowledge and practices across sociodemographic variables, diabetes history, and lifestyle characteristics. Statistically significant associations (p < 0.05) were observed for age, education level, family history of diabetes, blood sugar monitoring, diabetes status, adherence to a specific nutrition regimen, knowledge about diabetes acquisition, and participation in diabetes-related workshops or lectures. A more detailed analysis revealed that younger participants (18–22 years) predominantly demonstrated moderate knowledge, while those aged 23–27 years more frequently exhibited high knowledge. Higher academic standing was positively associated with knowledge levels, with fifth-year students showing greater proportions of moderate and high knowledge. Gender differences were also evident: males were more likely to have low knowledge, whereas females more often reported moderate or high levels. Engagement in health-related behaviors and information sources played a critical role. Participants who followed a nutrition regimen, monitored their blood sugar, attended diabetes workshops or lectures, or read about diabetes were more likely to exhibit moderate to high knowledge. Additionally, receiving information from healthcare professionals (doctors, nurses, or specialists) was associated with higher knowledge levels. Diabetes status and family history were also strongly linked to knowledge. Individuals with diabetes, especially those with Type 1 diabetes and those with a family history (first- or second-degree relatives), demonstrated higher levels of moderate and high knowledge compared to those without such histories. In contrast, no statistically significant associations were found between knowledge levels and either physical activity frequency or smoking status.
The relationship between diabetes-related knowledge, practices, and risk perception
The relationship among diabetes-related knowledge, risk perception, and practices was investigated. Diabetes-related knowledge was found to be statistically significant in relation to both the risk perception and health-related practices (Table 5) (p < 0.001).
Table 3: Comparison of diabetes-related knowledge across sociodemographic variables, diabetes history, and lifestyle characteristics
|
|
Knowledge | |||
| Low | Moderate | High |
p value* |
|
|
Age (years) |
||||
| 18–22
23–27 |
390 (38.2%)
63 (21.5%) |
532 (52.2%)
134 (45.7%) |
98 (9.6%)
72 (24.6%) |
0.000 |
|
Gender |
||||
| Male
Female |
180 (40.4%)
284 (29.2%) |
213 (47.8%)
464 (47.7%) |
52 (11.7%)
119 (12.2%) |
0.002 |
|
Education (academic year) |
||||
| First
Second Third Fourth Fifth |
262 (49.1%)
60 (28.3%) 58 (37.2%) 46 (24.7%) 38 (29.7%) |
256 (48.0%)
148 (69.8%) 85 (54.5%) 112 (60.2%) 76 (59.4%) |
28 (5.2%) 17 (8%) 29 (60.2%) 46 (24.7%) 51 (39.8%) |
0.000 |
|
Follow a specific nutrition regimen |
||||
|
Yes No |
62 (25.1%)
402 (37.1%) |
127 (51.4%)
550 (50.7%) |
40 (16.2%)
131 (12.1%) |
0.006 |
|
Frequency of physical activity |
||||
| 1–2 times /week
3–4 times/week 5+ times/week I do not exercise |
183 (33.5%)
101 (38.7%) 49 (31%) 131 (37.9%) |
295 (53.9%)
121 (46.6%) 88 (55.7%) 173 (50%) |
69 (12.6%)
39 (14.9%) 21 (13.3%) 42 (12.1%) |
0.368 |
|
Smoking status |
||||
| Smoker
Nonsmoker Previous smoker |
61 (43.6%)
38 (5.3%) 20 (37.0%) |
67 (47.9%)
584 (81.6%) 26 (48.1%) |
12 (8.6%)
152 (21.2%) 7 (13%) |
0.193 |
|
Have diabetes |
||||
| Yes, T2D
Yes, T1D No Not sure |
3 (20.0%)
1 (2.5%) 415 (34.0%) 45 (41.7%) |
8 (53.3%)
22 (55%) 596 (48.8%) 51 (47.2 %) |
6 (40.0%)
21 (52.5%) 136 (11.1%) 8 (7.4%) |
0.000 |
|
History of diabetes |
||||
| 1st-degree relatives
2nd-degree relatives No relatives |
93 (22.2%)
121 (33.2%) 250 (47.3%) |
241 (57.7%)
199 (54.5%) 273 (44.8%) |
84 (20.1%)
45 (12.3%) 42 (7.9%) |
0.000 |
|
Ever check your blood sugar |
||||
| Yes
No |
280 (46.9%)
184 (25.7%) |
271 (45.4%)
406 (56.8%) |
46 (7.7%)
125 (17.5%) |
0.000 |
|
Attend a diabetes workshop or lecture, or read about diabetes |
||||
| Yes
No |
85 (18.9%)
379 (44.0%) |
269 (59.8%)
408 (47.3%) |
96 (21.3%)
75 (8.7%) |
0.000 |
|
Have information on how a person gets diabetes |
||||
| Yes
No |
236 (58.7%)
228 (25.1%) |
157 (39.1)
520 (57.1%) |
9 (2.2%)
162 (17.8%) |
0.000 |
|
If the answer is yes, what is the source of this information? |
||||
| Television
Doctor Relative/friend Nurses/specialists Social media |
7 (35.0%)
22 (12.8% 109 (37.2%) 18 (10.8%) 128 (38.6%) |
12 (60.0%)
89 (51.7%) 170 (58.0%) 100 (59.9%) 171 (51.7%) |
1 (5.0%)
61 (35.5%) 14 (4.8% 49 (29.3%) 32 (9.6%) |
0.000 |
*Chi-square, Abbreviations: T2D; Type 2 diabetes, T1D; Type 1 diabetes
Table 4: Comparison of diabetes-related practices across sociodemographic variables, diabetes history, and lifestyle characteristics
|
|
Practice | ||||
| Poor | Neutral | Good |
p value* |
||
|
Age (years) |
|||||
| 18–22
23–27 |
263 (25.8%)
47 (17.5%) |
544 (53.3%)
147 (54.6%) |
213 (20.9%)
75 (27.9%) |
0.004 |
|
|
Gender |
|||||
| Male
Female |
115 (25.8%)
199 (23.0%) |
245 (55.1%)
462 (53.3%) |
85 (19.1%)
206 (23.8%) |
0.130 |
|
|
Education (academic year) |
|||||
| First
Second Third Fourth Fifth |
164 (30.0%)
51 (22.7%) 38 (22.1%) 36 (17.6%) 25 (15.2%) |
284 (52.0%)
127 (56.4%) 94 (54.7%) 113 (55.4%) 89 (53.9%) |
98 (17.9%)
47 (20.9%) 40 (23.3%) 55 (27.0%) 51 (30.9%) |
0.000 |
|
|
Follow a specific nutrition regimen |
|||||
| Yes
No |
290 (26.8%)
24 (10.5%) |
611 (56.4%)
96 (41.9%) |
182 (16.8%)
109 (47.6%) |
0.000 |
|
|
Frequency of physical activity |
|||||
| 1–2 times /week
3–4 times/week 5+ times/week I do not exercise |
102 (18.6%)
49 (18.8%) 26 (16.5%) 137 (39.6%) |
321 (58.7%)
131 (50.2% 69 (43.7%) 186 (53.8%) |
124 (22.7%)
81 (31.0%) 63 (39.9%) 23 (6.6%) |
0.000 |
|
|
Smoking status |
|||||
| Smoker
Nonsmoker Previous smoker |
10 (18.9%)
253 (22.6%) 51 (36.4%) |
30 (56.6%)
609 (54.4%) 68 (48.6%) |
13 (24.5%)
257 (23.0%) 21 (15%) |
0.005 |
|
|
Have diabetes |
|||||
| Yes, T2D
Yes, T1D No Not sure |
4 (9.1%)
4 (23.5%) 265 (23.1%) 41 (39.4%) |
21 (47.7%)
6 (35.3%) 626 (22.3%) 53 (51.0%) |
19 (43.2%)
6 (35.3%) 256 (22.3%) 10 (9.6%) |
0.000 |
|
|
History of diabetes |
|||||
| 1st-degree relatives
2nd-degree relatives No relatives |
70 (16.7%)
94 (25.8%) 150 (28.4%) |
220 (52.6%)
198 (54.2%) 289 (54.6%) |
128 (30.6%)
73 (20.0%) 90 (17.0%) |
0.000 |
|
|
Ever check your blood sugar |
|||||
| Yes
No |
192 (23.2%)
122 (17.1%) |
327 (54.8%)
380 (53.1%) |
78 (13.1%)
213 (29.8%) |
0.000 |
|
|
Attend a diabetes workshop or lecture, or read about diabetes |
|||||
| Yes
No |
255 (29.6%)
59 (13.1%) |
468 (54.3%)
239 (53.1%) |
139 (16.1%)
152 (33.8%) |
0.000 |
|
|
Have information on how a person gets diabetes |
|||||
| Yes
No |
149 (37.1%)
165 (18.1%) |
226 (56.2%)
481 (52.9% |
27 (6.7%)
264 (29.0%) |
0.000 |
|
|
If the answer is yes, what is the source of this information? |
|||||
| Television
Doctor Relative/friend Nurses/specialists Social media |
5 (25.0%)
20 (11.6%) 65 (22.2%) 22 (13.2%) 18 (25.9%) |
11 (55.0%)
90 (52.3%) 164 (56.0%) 76 (45.5%) 183 (55.1%) |
4 (20.0%)
62 (36.0%) 64 (21.8%) 69 (41.3%) 63 (19.0%) |
0.000 |
|
*Chi-square, Abbreviations: T2D; Type 2 diabetes, T1D; Type 1 diabetes
Table 5. Association between diabetes-related knowledge, risk perception, and health-related practices.
|
|
Knowledge | |||
| Low | Moderate | High |
P value |
|
|
Risk perception |
||||
|
My assessment of diabetes and its impact on health |
||||
| Not influential
Weak risk Moderate risk High risk |
15 (1.2%)
33 (2.7%) 265 (21.8%) 151 (12.4%) |
4 (0.3%)
37 (3.1%) 361 ( 29.8 275 (22.7%) |
0 (0%)
8 (0.7%) 70 (5.8%) 93 (7.7%) |
0.000 |
|
My assessment of the impact of diabetes on people of my age |
||||
| Not influential
Weak risk Moderate risk High risk |
23 (1.8%)
61 (5.5%) 247 (20.3%) 133 (10.9%) |
7 (0.5%)
76 (6.2%) 365 (30.0%) 229 (24.6%) |
0 (0%)
14 (1.5%) 100 (8.2%) 57 (4.6%) |
0.000 |
|
My assessment of the possibility that I might have diabetes |
||||
| Not influential
Weak risk Moderate risk High risk |
33 (2.7%)
140 (11.5%) 214 (17.9%) 77 (6.3%) |
79 (6.5%)
242 (19.9%) 290 (23.9%) 66 (5.4%) |
36 (2.9%)
55 (4.5%) 68 (5.6%) 12 (0.9%) |
0.000 |
|
Health-related practices |
||||
| Poor practices | 163 (51.9%) | 139 (44.3%) |
12 (3.8%) |
0.000 |
|
Neutral practices |
248 (35.1%) | 382 (54.0%) | 77 (10.9% | |
| Good practices | 53 (18.2%) | 156 (53.6%) |
82 (28.2%) |
|
The results of the regression analysis exploring the relationship between knowledge, education, and health-related practices are presented in Table 6 (a). The correlation coefficient (R) of 0.321 suggests a moderate positive correlation between these variables. The R² value of 0.103 suggests that 10.3% of the variation in health-related practices can be explained by knowledge and education. The F-statistic of 47.991, with a p-value of less than 0.001, confirms that the model is statistically significant.
According to the coefficient behavior Table 6 (b), a one-unit increase in knowledge score is associated with a 2.084-unit increase in health-related practices, while a one-unit increase in education corresponds to a 0.247-unit increase in health-related practices; both effects are statistically significant. Despite these significant relationships, the model explains only a small proportion of the variance in health-related practices, suggesting that other factors not included in the model may also influence these behaviors.
Table 6: Simple linear regression between health-related practices, knowledge score, and education model summary and ANOVA.
|
a. Predictors: (Constant), education, knowledge score (independent variables) |
|||||||||
| Model | R | R square | Adjusted R square | Standard error of the estimate | Mean square | Sum of squares | df | F | Sig. |
| 1 | 0.321 | 0.103 | 0.103 | 4.48426 | 1507.972 | 3015.945 | 2 | 47.991 | 0.000 |
|
b. Coefficients: Behavior (dependent variable) |
|||||||||
|
Model |
Unstandardized coefficients | Standardized coefficients | t | Sig. | |||||
| B | Std. error |
Beta |
|||||||
|
1
|
(Constant) |
13.422 | 0.373 | 35.946 | 0.000 | ||||
| Knowledge | 2.084 | 0.196 | 0.290 | 10.625 |
0.000 |
||||
|
Education |
0.247 | 0.088 | 0.076 | 2.791 |
0.005 |
||||
df: degrees of freedom (df), F: F statistics, Sig.: significance
Discussion
A lack of knowledge about the risk factors related to diseases, including diabetes, can make it challenging to take preventive measures, such as adopting healthy lifestyle habits. Therefore, a knowledge-based understanding of one’s personal risk of diabetes is essential for successful preventive health behaviors.21, 22 Communities and educational institutions have studied knowledge, attitudes, and practices related to diabetes.19, 23-25 The current study examined the level of knowledge about diabetes, health-related practices, and the perceived risk of diabetes among university students in SA and investigated the associated sociodemographic variables, diabetes history, and lifestyle factors of 1,312 students.
The current study found a low level of diabetes knowledge among university students. Similarly, a nationwide cross-sectional study in Poland reported insufficient public awareness of diabetes among adults.26 Previous studies on diabetes knowledge among Saudi university students have shown varying results; however, the majority consistently reported low or moderate levels of knowledge, which aligns with the findings of our study.25, 27, 28 Reviews have concluded that diabetes knowledge and awareness are poor among non-diabetic students and patients with diabetes in SA.29, 30 These findings highlight the need for increased knowledge and awareness of diabetes among the Saudi population. Strategies for improving diabetes awareness should be integrated into existing healthcare systems.
Individuals with poor diabetes knowledge may engage in unhealthy lifestyle behaviors, such as poor dietary choices and physical inactivity, both known risk factors for T2D. However, a substantial body of research has demonstrated that up to 60% of T2D cases can be prevented through lifestyle modifications, such as adopting a healthy diet and increasing physical activity.31 Community-based diabetes education interventions have been shown to improve diabetes knowledge and health beliefs, leading to positive changes in self-reported behaviors.32
Moreover, individuals with limited knowledge of diabetes are less likely to recognize its symptoms or seek medical advice when they occur, potentially leading to delays in diagnosis and treatment, which increases the risk of complications.26 A low level of diabetes knowledge has also been significantly associated with a higher likelihood of undiagnosed diabetes and impaired fasting glucose levels.33 The prevalence of undiagnosed diabetes in Saudi adults has been reported to be as high as 23%, which points to the importance of targeted diabetes education programs. 34
Only 34% of the students in this study attended a diabetes education program, and of those who received information about diabetes, only 36% obtained it from healthcare professionals. More than 60% of the students reported that their primary sources of diabetes information were friends, relatives, or social media. Similarly, a previous cross-sectional survey in China, which assessed self-reported knowledge of diabetes among college students, found that newspapers, books, television, and the internet were the major sources of knowledge about T2D.35 Another study suggested that sources of information play a key role in diabetes knowledge, with those who had better knowledge of the Hispanic population receiving their information primarily from healthcare providers.36
The most significant knowledge gap identified was in the area of diabetes-related dietary choices, with the majority of diet-related questions receiving insufficient scores in this study. Suboptimal diabetes-related nutritional knowledge has been reported to be associated with a higher glycemic index in patients with diabetes.37 This evidence suggests that educational programs should focus on nutrition to prevent diabetes, which could improve dietary self-management practices.
The current study examined diabetes-related knowledge, health practices, and perceptions of diabetes risk across various sociodemographic predictors, lifestyle factors, and diabetes history. Age, education, family history of diabetes, and engaging in behaviors such as regularly monitoring blood sugar levels or adhering to a specific diet were all significantly associated with better health-seeking behaviors and greater diabetes knowledge (p < 0.05). These findings are consistent with previous research that identified education level as a key determinant of diabetes risk perception and family history as a significant predictor of diabetes awareness.38, 39 A positive correlation has been reported between education and knowledge in areas such as health promotion and disease management, as individuals with higher education are more likely to be exposed to health-related messages.40 Furthermore, we found diabetes knowledge to be significantly different between genders, which is inconsistent with the literature. A cross-sectional study found that diabetes knowledge among females was lower than among males in SA.41 Another study in Poland found that female gender, higher education, and a family history of diabetes were associated with a higher level of diabetes awareness.26
In this study, participants who regularly monitored their blood sugar levels and followed a specific nutrition regimen demonstrated greater diabetes knowledge and better health-related practices, suggesting that these practices may reinforce diabetes awareness, as seen in a previous study.18 Outcomes such as increased attendance at diabetes educational sessions have been previously associated with higher levels of knowledge, attitudes, and improved practices, highlighting the importance of targeted education.18, 42, 43 Previous research has confirmed that educational programs can significantly enhance the understanding of diabetes risks and management. 42, 43
Notably, higher levels of knowledge among participants were associated with a better understanding of diabetes risks and their consequences, which in turn influenced health-related behaviors. These results are consistent with other research that suggests that a lack of awareness of diabetes risk factors may contribute to students’ inaccurate assessments of their future risk for the disease.44, 45 College students frequently have a moderate understanding of diabetes, along with inaccurate risk perceptions that are influenced by their self-reported good health.46 This emphasizes the necessity of focused educational initiatives to increase understanding, dispel myths, and raise the precision of risk assessments.
A major strength of this study is its large sample size, which includes participants from multiple universities and regions across SA. In addition, the survey tool employed has been previously used among young populations in Arab countries, including Saudi Arabia and Jordan. 18, 19 However, several limitations should be acknowledged. First, the cross-sectional design of the study restricts the ability to draw causal inferences between the examined variables. Second, reliance on self-reported data may introduce biases related to recall and social desirability. Third, the use of an online self-administered questionnaire may have led to self-selection bias. Although this method ensured participant anonymity and convenience, the findings are likely to reflect the characteristics of individuals who chose to participate. Unobservable factors influencing participation—such as greater health awareness or personal relevance to the topic—may have influenced the results, thereby limiting the external validity and generalizability of the findings to the broader university student population.
Conclusion
The current study determined the students’ levels of knowledge about diabetes as well as their scores related to health practices for different aspects of diabetes, highlighting areas of insufficient knowledge and practice among the surveyed students. The findings of this study underscore the need for targeted educational programs that enhance understanding of diabetes, particularly among students without a medical background or a family history of the disease. Emphasizing diabetes-related nutrition and lifestyle practices could help strengthen prevention efforts and empower students to make informed health decisions. Future studies are needed to assess the impact of tailored public diabetes education programs on decreasing the risk of developing T2D in the Saudi population.
Acknowledgement
The authors express their gratitude to the study participants for their valuable contributions.
Funding Sources
This research was funded by Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2025R207), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
Conflicts of Interest
The authors declare no potential conflicts of interest.
Data Availability Statement
All data are available in the paper and can be provided upon request.
Ethics Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of Princess Nourah bint Abdulrahman University (PNU IRB number 21-0013, dated 10 January 2021).
Informed Consent Statement
Informed consent was obtained from all participants, in accordance with the ethical standards applicable in the country of origin. Participants indicated their consent by clicking the “I agree” button on the digital questionnaire. The privacy rights of all participants were respected throughout the study.
Clinical Trial Registration
This research does not involve any clinical trials.
Permission to Reproduce Material from Other Sources
Not Applicable
Author Contributions
- Nahla Mohammed Bawazeer – Conceptualization, Methodology, Project Administration, Writing, and Final Approval of the Manuscript.
- Abeer Salman Alzaben – Conceptualization, Methodology, Funding Acquisition, Writing, and Final Approval of the Manuscript.
- Sumia Mohammed Enani – Collection and Analysis and Drafting the Original Manuscript.
- Albandari Abdullah Bin Ammar – Data Collection and Drafting the Original Manuscript.
- Howeida Hassan Abusalih – Formal Analysis
- Amal Hamdi Kenank – Data Collection.
- Alaa Jameel Almiman – Data Collection.
- Abdulrahman Ahmed Alsayegh – Data Collection.
References
- Galicia-Garcia U., Benito-Vicente A., Jebari S., et al. Pathophysiology of Type 2 Diabetes Mellitus. Int J Mol Sci. 2020; 21(17):6275. https://doi.org/10.3390/ijms21176275
CrossRef - International Diabetes Federation. IDF Diabetes Atlas 2021. https://diabetesatlas.org/idfawp/resource-files/2021/07/IDF_Atlas_10th_Edition_2021.pdf. Accessed June 25, 2023.
- Centers for Diabetes Control and Prevention. Type 2 Diabetes is a Rising Threat in Youth 2023. https://www.cdc.gov/diabetes/library/socialmedia/infographics/diabetes-youth-threat.html. Accessed June 25, 2023.
- Zhang C., Zhang H., Zhang Bo. Prevalence trends and racial-ethnic disparities of diabetes and prediabetes among children and adolescents in the United States from 2019 to 2021. Prev Med Rep. 2024; 41:102688. https://doi.org/10.1016/j.pmedr.2024.102688
CrossRef - Buttermore E., Campanella V., Priefer R. The increasing trend of Type 2 diabetes in youth: An overview. Diabetes Metab Syndr. 2021; 15(5):102253. https://doi.org/10.1016/j.dsx.2021.102253
CrossRef - Wilmot E., Idris I. Early onset type 2 diabetes: risk factors, clinical impact and management. Ther Adv Chronic Dis. 2014; 5(6):234-44. https://doi.org/10.1177/2040622314548
CrossRef - D’Adamo E., Caprio S. Type 2 diabetes in youth: epidemiology and pathophysiology. Diabetes Care. 2011; 34 Suppl 2(Suppl 2):S161-5. https://doi.org/10.2337/dc11-s212
CrossRef - Al-Rubeaan K., Al-Manaa H.A., Khoja T.A., et al. Epidemiology of abnormal glucose metabolism in a country facing its epidemic: SAUDI-DM study. J Diabetes. 2015; 7(5):622-32. https://doi.org/10.1111/1753-0407.12224
CrossRef - Al-Rubeaan K. National surveillance for type 1, type 2 diabetes and prediabetes among children and adolescents: a population-based study (SAUDI-DM). J Epidemiol Commun Health. 2015; 69(11):1045-51. https://doi.org/10.1136/jech-2015-205710
CrossRef - Cha E., Akazawa M.K., Kim K.H., et al. Lifestyle habits and obesity progression in overweight and obese American young adults: Lessons for promoting cardiometabolic health. Nurs Health Sci. 2015;.17(4):467-75. https://doi.org/10.1111/nhs.12218
CrossRef - Shilbayeh S. Type 2 diabetes mellitus and its effect on quality of life in adolescents: A retrospective cohort study in Saudi Arabia. Pediatr Endocrinol Diabetes Metab. 2022; 28(1):54-63. https://doi.org/10.5114/pedm.2022.113988
CrossRef - Aljoudi A.S., Taha A.Z. Knowledge of diabetes risk factors and preventive measures among attendees of a primary care center in eastern Saudi Arabia. Ann Saudi Med. 2009; 29(1):15-9. https://doi.org/10.4103/0256-4947.51813
CrossRef - Mohieldein A.H., Alzohairy M.A., Hasan M. Awareness of diabetes mellitus among Saudi nondiabetic population in Al-Qassim region, Saudi Arabia. J Diabetes Endocrinol. 2011; 2(2):14-9. https://doi.org/10.18203/2319-2003.ijbcp20171678
CrossRef - Alkhaldy A.A., Alamri R.S., Magadmi R.K., et al. Dietary Adherence of Saudi Males to the Saudi Dietary Guidelines and Its Relation to Cardiovascular Diseases: A Preliminary Cross-Sectional Study. J Cardiovasc Dev Dis. 2019; 6(2):17. https://doi.org/10.3390/jcdd6020017
CrossRef - Hanbazaza M.A., Mumena W.A. Knowledge and Practices Related to Salt Intake among Saudi Adults. Int J Environ Res Public Health. 2020; 17(16):5749. https://doi.org/10.3390/ijerph17165749
CrossRef - Alkhaldy A.A., Rizq N.K., Del Jaylan S.A., et al. Dietary Intake and Physical Activity in Relation to Insulin Resistance in Young Overweight Saudi Females: An Exploratory Pilot Study. Prev Nutr Food Sci. 2019; 24(4):373-80. https://doi.org/10.3746/pnf.2019.24.4.373
CrossRef - Andy Field. Discovering Statistics Using IBM SPSS Statistics. FIFTH EDITION. University of Sussex, UK: Sage edge; 2017.
- Alzaben A.S., Bakry H.M., Alnashwan N.I., et al. The influence of a diabetes awareness program on diabetes knowledge, risk perception,
and practices among university students. Primary care diabetes. 2023; 17(4):327-33. https://doi.org/10.1016/j.pcd.2023.04.011
CrossRef - Khlaifat A.M., Al-Hadid L.A., Dabbour R.S., et al. Cross-sectional survey on the diabetes knowledge, risk perceptions and practices among university students in South Jordan. J Diabetes Metab Disord. 2020; 19(2):849-58. https://doi.org/10.1007/s40200-020-00571-8
CrossRef - Mainous A.G., Mansoor H., Rahmanian K.P., et al. Perception of Risk of Developing Diabetes Among Patients With Undiagnosed Prediabetes: The Impact of Health Care Provider Advice. Clin Diabetes. 2019; 37(3):221-6. https://doi.org/10.2337/cd18-0050
CrossRef - Harrison J.A., Mullen P.D., Green L.W. A meta-analysis of studies of the Health Belief Model with adults. Health Educ Res. 1992;7(1):107-16. https://doi.org/10.1093/her/7.1.107
CrossRef - Janz N.K., Becker M.H. The Health Belief Model: a decade later. Health Educ Q. 1984; 11(1):1-47. https://doi.org/10.1177/109019818401100101
CrossRef - Alqahtani M., Almutairi F.E., Albasseet A.O., et al. Knowledge, Attitude, and Practice of Diabetes Mellitus Among the Saudi Population in Riyadh, Saudi Arabia: A Quantitative Study. Cureus. 2020; 12(1):e6601. https://doi.org/10.7759/cureus.6601.
CrossRef - Alsous M., Abdel Jalil M., Odeh M., et al. Public knowledge, attitudes and practices toward diabetes mellitus: A cross-sectional study from Jordan. PLoS One. 2019; 14(3):e0214479. https://doi.org/10.1371/journal.pone.0214479.
CrossRef - Gazzaz Z.J. Knowledge, Attitudes, and Practices Regarding Diabetes Mellitus Among University Students in Jeddah, Saudi Arabia. Diabetes Metab Syndr Obes. 2020; 13:5071-8. https://doi.org/10.2147/DMSO.S287459.
CrossRef - Sekowski K., Grudziaz-Sekowska J., Pinkas J., et al. Public knowledge and awareness of diabetes mellitus, its risk factors, complications, and prevention methods among adults in Poland-A 2022 nationwide cross-sectional survey. Front Public Health. 2022; 10:1029358. https://doi.org/10.3389/fpubh.2022.1029358.
CrossRef - Alamri O. Knowledge of Diabetes Characteristics by Students at University of Tabuk, Saudi Arabia. Health. 2021; 13(4):393-404. https://doi.org/10.4236/health.2021.134032.
CrossRef - Khamaiseh A.M., Alshloul M.N. Diabetes Knowledge among Health Sciences Students in Saudi Arabia and Jordan. Jordan Med J. 2019; 53(1):37-48. https://doi.org/10.55544/jrasb.2.5.8
CrossRef - Robert A.A., Al Awad A.D., Al Dawish M.A. Current Status of Knowledge and Awareness of Diabetes Mellitus in Saudi Arabia. Curr Diabetes Rev. 2021; 17(5):e101220186818. https://doi.org/10.2174/1573399816999201012200841.
CrossRef - Alanazi F.K., Alotaibi J.S., Paliadelis P., et al. Knowledge and awareness of diabetes mellitus and its risk factors in Saudi Arabia. Saudi Med J. 2018; 39(10):981-9. https://doi.org/10.15537/smj.2018.10.22938.
CrossRef - Galaviz K.I., Narayan K.M.V., Lobelo F., et al. Lifestyle and the Prevention of Type 2 Diabetes: A Status Report. Am J Lifestyle Med. 2018; 12(1):420. https://doi.org/10.1177/1559827615619159.
CrossRef - Chapman-Novakofski K., Karduck J. Improvement in knowledge, social cognitive theory variables, and movement through stages of change after a community-based diabetes education program. J Am Diet Assoc. 2005; 105(10):1613-6. https://doi.org/10.1016/j.jada.2005.07.010.
CrossRef - Hallit S., Saade S., Zeidan R.K., et al. Factors associated with undiagnosed type II diabetes mellitus, undiagnosed impaired fasting glucose and these patients’ quality of life in Lebanon. J public health. 2020 ;42(3):550-60. https://doi.org/10.1093/pubmed/fdz051.
CrossRef - Jambi H., Enani S., Malibary M., et al. The Association Between Dietary Habits and Other Lifestyle Indicators and Dysglycemia in Saudi Adults Free of Previous Diagnosis of Diabetes. Nutr Metab Insights. 2020; 13:1178638820965258. https://doi.org/10.1177/1178638820965258.
CrossRef - Xu Y., Zhang D., Liu K., et al. Self-reported knowledge on diabetes and its related factors among Chinese college students: a cross-sectional study. BMJ Open. 2016; 6(9):e011963. https://doi.org/10.1136/bmjopen-2016-011963.
CrossRef - Zhao X. Relationships between sources of health information and diabetes knowledge in the U.S. Hispanic population. Health Commun. 2014; 29(6):574-85. https://doi.org/10.1080/10410236.2013.784937.
CrossRef - Breen C., Ryan M., Gibney M.J., et al. Diabetes-related nutrition knowledge and dietary intake among adults with type 2 diabetes. Br J Nutr. 2015; 114(3):439-47. https://doi.org/10.1017/S0007114515002068.
CrossRef - Whitaker S.M., Bowie J.V., McCleary R., et al. The Association Between Educational Attainment and Diabetes Among Men in the United States. Am J Mens Health. 2014; 8(4):349-56. https://doi.org/10.1177/1557988313520034.
CrossRef - Baptiste-Roberts K., Gary T.L., Beckles G.L., et al. Family history of diabetes, awareness of risk factors, and health behaviors among African Americans. Am J Public Health. 2007; 97(5):907-12. https://doi.org/10.2105/AJPH.2005.077032
CrossRef - Veerasetty N.K., Venkatachalam J., Subbaiah M., et al. Determinants of health literacy and its impact on glycemic control among women with gestational diabetes mellitus in a tertiary care hospital, Puducherry – A cross-sectional analytical study. J Educ Health Promot. 2024; 13:119. https://doi.org/10.4103/jehp.jehp_762_23.
CrossRef - Abdulghani H.M., Ahmed M.M., Al-Rezqi A.M., et al. Knowledge and awareness levels of diabetes mellitus risk factors among nondiabetic visitors of primary health care centers: a multicenter study. Eur Rev Med Pharmacol Sci. 2021; 25(22):7066-77. https://doi.org/10.26355/eurrev_202111_27259.
- Alsous M.M., Odeh M., Abdel Jalil M. Effect of an educational intervention on public knowledge, attitudes, and intended practices towards diabetes mellitus: A quasi-experimental study. Int J Clin Pract. 2020; 74(9):e13565. https://doi.org/10.1111/ijcp.13565.
CrossRef - Shiferaw W.S., Akalu T.Y., Desta M., et al. Effect of educational interventions on knowledge of the disease and glycaemic control in patients with type 2 diabetes mellitus: a systematic review and meta-analysis of randomised controlled trials. BMJ Open. 2021 ;11(12):e049806. doi: 10.1136/bmjopen-2021-049806.
CrossRef - Collins K.M., Dantico M., Shearer N.B., et al. Heart disease awareness among college students. J Commun Health. 2004; 29(5):405-20. https://doi.org/10.1023/b:johe.0000038655.19448.b2.
CrossRef - Mongiello L.L., Freudenberg N., Jones H. Diabetes Risk Factor Knowledge Varies Among Multiracial College Students. J Immigr Minor Health. 2016; 18(5):971-8. https://doi.org/10.1007/s10903-015-0250-9.
CrossRef - Khan R.K., Misra R., Shawley-Brzoska S., et al. Predictors of diabetes risk perception among college students. J Am Coll Health. 2022; 70(6):1803-9. https://doi.org/10.1080/07448481.2020.1825222.
CrossRef
Abbreviations List
DM – Diabetes Mellitus
T1D – Type 1 Diabetes
T2D – Type 2 Diabetes
R – Correlation Coefficient
SA – Saudi Arabia
Accepted on: 19 July 2025
Second Review by: Matt Kasman
Final Approval by: Dr. Suhad Bahijr





Web of Science Coverage
Emerging Sources Citation Index (ESCI)
2024 Journal Impact Factor: 1.1
Scopus Journal Metrics
CiteScore 2025: 2.6
CiteScore Details
Sustainable Nutrition: Food Systems, Nutrient Retention, and Public Health Impact
![]()
This journal is a member of, and subscribes to the principles of, the Committee on Publication Ethics (COPE)








