Pre-Post Assessment of Serum Zinc and Copper Status in Uncomplicated Pulmonary Tuberculosis Patients Receiving Directly Observed Treatment Short Course
 , Rukmini M S, Durga Rao Yalla and Sowndarya K
, Rukmini M S, Durga Rao Yalla and Sowndarya K Department of Biochemistry, Kasturba Medical College, Mangalore, Manipal Academy of Higher Education, Manipal, Karnataka, India.
Corresponding Author E-mail: poornima.manjrekar@manipal.edu
DOI : http://dx.doi.org/10.12944/CRNFSJ.11.2.31
Download this article as:
![]()
Mycobacterium tuberculosis causing the infectious disease tuberculosis has a predilection for the lungs although it is common to see other organs involved. India has adopted the TB-DOTS program for the treatment of the same. Undernutrition and tuberculosis are mutually inclusive. Micronutrients like zinc and copper play a key role in cytokine kinetics and immunity and thus are important in an individual’s response to infectious disease. Serum copper and zinc levels in patients with pulmonary tuberculosis (pTB) before and after two months of directly observed treatment short course (DOTS) were assessed in this study. The serum samples of 39 pTB patients were collected before the commencement of anti-tubercular therapy (ATT) and tested for copper and zinc levels. At the end of the intensive phase of treatment, blood samples of 31 out of the 39 pTB patients were again collected and tested for the same trace elements. In the pre-post comparison of 31 patients who could be followed up, an increase in serum zinc levels [101 (74.9) μg/dl vs 112(155.5) μg/dl)] after the treatment was not statistically significant (p=0.15). The serum copper levels [184(105.7) μg/dl vs 247(80.8) μg/dl)] were significantly increased after two months of DOTS therapy. Sputum negativity was close to 81%.Serum copper, as well as zinc levels, were increased after DOTS therapy for two months. Since the response to therapy was 69%, supplementation of copper and zinc may benefit the pTB patients in achieving sputum negativity sooner and completely.
KEYWORDS:Copper; DOTS; Inflammation; Tuberculosis; Zinc
Introduction
Mycobacterium tuberculosis, primarily affecting the lungs and causing pTB is listed by World Health Organization (WHO) as the ninth leading cause of death globally. In 2019, there were 10.0 million (8.9–11.0 million) Tuberculosis (TB) cases and 1.2 million TB deaths among the HIV-negative subjects, and an additional 208000 deaths (177 000–242 000) among HIV-positive subjects. 1Drug-resistant TB endures being a threat to community health. In 2019, about half a million individuals developed rifampicin-resistant TB (RR-TB), amongst which 78% had multidrug-resistant TB (MDR-TB) globally. The three nations with the major share of the worldwide burden included India (27%), China (14%), and Russian Federation (8%).1
The risk of developing TB is high in people with HIV (41.4%), overcrowding (57.3%), poverty (39.5%), smoking (26.37%), close contacts (11.5%), diabetes (5.4%), family history (17.5%) and alcohol use (50.7%).2-4. Undernutrition leads to secondary immunodeficiency which in turn upsurges the susceptibility of the host to infection. Protein-energy malnutrition and deficiencies of micronutrients increase the risk of TB.5
Several micronutrients have a role in immune modulation. Among these, the trace elements zinc and copper have played a key role in the proliferation and differentiation of the cells involved in acquired and innate immunity and thus they are essential in providing resistance to infectious diseases like tuberculosis.6 The adversities of zinc deficiency on antibody and cytokine production, cell signaling, chemotaxis, proliferation, and functioning of natural killer, B lymphocytes, and T helper cells have been well established.7 Zinc plays a vital role in the catalysis and structural stabilization of over 300 enzymes and is a part of metalloproteins, many of which are present in immune cells.8
Zinc influences both acquired and innate immune functions.9 It is extremely critical for the regular growth and functioning of the cells that mediate innate immunity, neutrophils, and NK cells. Phagocytosis, intracellular killing, and the production of cytokines are affected by the deficiency of zinc. Zinc deficiency can also affect the growth and functioning of T and B cells. Due to the ability of zinc to act as an anti-oxidant and stabilize membranes, its role in preventing free radical-induced injury during the inflammatory processes is well understood.10 Zinc deficiency causes alteration in the number and function of monocytes, natural killer cells, neutrophils, B cells, and T cells.5, 9 It decreases the synthesis of TNF, IFN-γ, and IL-1.11
Zinc availability is regulated by transporter proteins, ZnT and ZnP, and storage proteins metallothionein.12,13 Zinc is essential for Mycobacterium tuberculosis in small amounts but turns out to be toxic in excess.14 Certain bacteria such as Mycobacterium tuberculosis thrive inside their host by effluxing transition metals, predominantly zinc and copper.15
Copper is a vital component of the enzyme Superoxide Dismutase of the respiratory burst pathway which is required for the production of hydrogen peroxide in monocytes and neutrophils.9. 16 Copper deficiency leads to neutropenia and thus it has been proposed that copper has a role in leukocyte proliferation and differentiation.17The innate immune mechanism causes accumulation of copper in macrophage phagosomes infected with mycobacteria. To overcome this, the bacteria have developed copper resistance mechanisms.18Copper is imperative for the viability of Mycobacterium tuberculosis but the copper supplied by the host has been reported to suppress the growth of the bacteria.17 Copper is transported into the phagosome thus destroying the bacilli. To thrive, the mycobacteria express metal efflux pumps.15 Like Zinc, Copper is necessary for the growth and development of Mycobacterium tuberculosis, but is toxic, when consumed in higher amounts.18Remarkably high levels of copper have been observed in primary granulomas in the lungs of guinea pigs infected with mycobacteria.14
There are conflicting reports as regards the role of micronutrients in tuberculosis. Also, there is not sufficient evidence for the supplementation or otherwise of these elements during tuberculosis treatment. The current study was planned to evaluate the micronutrient status in patients with TB before and after DOTS and note the recovery status.
Materials and methods
The current prospective observational study was conducted after obtaining the institutional ethical clearance (IEC KMC MLR 02-18/36 dated 21.02.2018). Freshly diagnosed TB patients without any other known immunological disease were included during their first visit to the District Tuberculosis Centre. Sputum smear-positive cases with treatment failure or receiving treatment after the treatment interruption, patients with relapse of TB, HIV positive, and known cases of extrapulmonary TB were excluded. All participants voluntarily consented to participate in the study.
Patient demographics (Age, gender, height, and weight) and clinical (sputum positivity) details were documented using a proforma. Height and weight were noted following standard procedures and equipment and calculation of BMI was done using the formula: weight (kg) /height (m)2 at baseline and after 2 months of the DOTS regime. DOTS regime for the first two months consists of Isoniazid, Rifampicin, Pyrazinamide, and Ethambutol. Treatment adherence was meticulously ensured through telephonic calls by the primary author and the field workers of the National TB eradication program of India. Blood samples from study patients were collected in sterile plain blood collection tubes under aseptic conditions before the initiation of therapy and after the follow-up period of 2 months. Centrifugation of serum was done at 3000 rpm for 5 minutes and was stored in 2mL aliquots at -20oC for further analysis. Only 31 of the 39 baseline cases could be followed up. The rest were either lost or refused to be part of the study. For the pre-post comparison, data from the 31 patients who could be followed up was used.
At the end of the baseline and follow-up period, serum Copper and Zinc levels were estimated.
The Nitro-PAPS method and (3, 5-Di-Bromo-2-pyridylazo)-N-ethyl-N-(3-sulphopropyl) aniline method were adopted for the spectrophotometric estimation of zinc and copper respectively using commercially available kits procured from Coral Clinical Systems using semi-auto analyzer Star 21 Plus. Zinc reacts with Nitro-PAPS in an alkaline medium to form a purple-coloured compound. The intensity of the compound formed is directly proportionate to the concentration of zinc in the sample. In an acidic medium, copper released from ceruloplasmin reacts with Di-Br-PAESA to form a colored compound. The intensity of the compound formed is directly proportional to the concentration of copper present in the sample.
Analysis of data was done using SPSS (Statistical Package for the Social Sciences) version 20.0. Depending on the data distribution, continuous variables were analyzed by paired t test or Wilcoxon sign rank test (before and after comparison). Chi square test was used to analyze the categorical variables. p<0.05 was considered statistically significant.
Results
At Baseline – Prior to the Initiation of DOTS Treatment
The mean age of 39 pTB sputum smear-positive patients was found to be 41.56 ±15.67 years. The Body Mass Index (BMI) of the patients was 17.45±2.45 Kg/m2. The median serum Zinc and Copper levels before treatment were 105 μg/dl (71 μg/dl) and 193 μg/dl (170 μg/dl) respectively. [Table 1]
Table 1: Baseline Characteristics of Pulmonary Tuberculosis patients prior treatment (n=39) and after two months of DOTS treatment (n=31)
| Parameters | Pre-treatment (n=39)Mean ± SD | Post-treatment(n=31)Mean ± SD |
| Age (years) | 41.56±15.67 | 41.88±17.08 |
| Height(cm) | 161.92±9.14 | 163.51±6.52 |
| Weight(Kg) | 45.92±8.45 | 47.07±8.15 |
| BMI(Kg/m2) | 17.45±2.45 | 17.56±2.86 |
| Sputum Positivity (Male: Female) | 27: 12 | 23:8 |
| Zinc# μg/dl | 105 (71) | 122 (92) |
| Copper# μg/dl | 193 (170) | 252.5 (99.5) |
All results were expressed as Mean ± SD
#Expressed as Median and (interquartile range)
After Two Months of Follow up – Post DOTS Treatment
After DOTS treatment, among 31 pulmonary tuberculosis patients, BMI was found to be 17.56±2.86 Kg/m2. The serum Zinc and copper levels increased to 122(92) μg/dl and 252.5 (99.5)μg/dl) respectively. [Table 1]
For pre-post comparison, the data of the 31 cases available during the follow-up period was used. The increase in serum zinc levels of these 31 cases from their baseline median of 101(74.9) μg/dl to 112(155.5) μg/dl after the treatment was not statistically significant (p=0.15). The serum copper levels significantly increased from 184(105.7) μg/dl to 247(80.8) μg/dl) (p<0.01) after two months of DOTS therapy for the patients. [Table 2]
Table 2: Comparison of demographic, clinical characteristics, and serum Concentrations of micronutrients of tuberculosis patients before and after Two months of DOTS
| Variables | Baseline (n=31) | Follow up (n=31) | p-value |
| Height (Cms) | 162.8 ± 6.46 | 162.8 ± 46 | – |
| Weight (Kg) | 45.57 ± 8.01 | 46.52 ± 8.07 | 0.17 |
| BMI (Kg/M2) | 17.16 ± 2.84 | 17.53 ± 3.06 | 0.17 |
| Zinc# μg/dl | 101(74.9) | 112 (155.5) | 0.15 |
| Copper# μg/dl | 184 (105.7) | 247(80.8) | <0.01* |
All results are expressed as Mean ± SD (Standard Deviation)
Paired t-test, #Expressed as Median and (interquartile range)
*p <0.05 is considered significant, Wilcoxon signed-rank test.
Sputum Conversion after Follow up
At the end of intensive phase treatment, 31 pTB patients were followed up; 19% of patients remained sputum positive, 12% showed scanty acid-fast bacilli and 69% were sputum negative. [Figure 1]
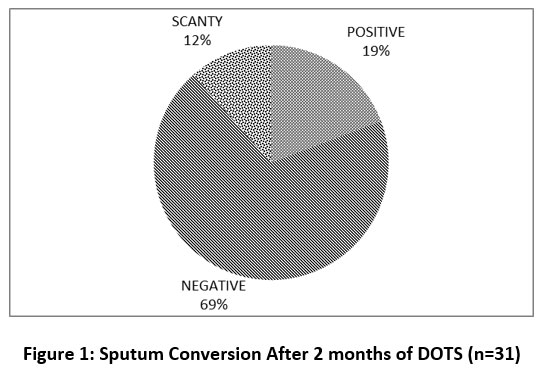 |
Figure 1: Sputum Conversion After 2 months of DOTS (n=31) |
Discussion
Nutritional status largely determines acquiring pTB infection and the course of the disease. In this study, we assessed the BMI, sputum negative conversion, and serum levels of copper (Cu) and Zinc (Zn) before and after two months of the Directly Observed Treatment Short course (DOTS) regime and compared them. Being underweight is identified both as a cause and a result of anorexia and weight loss in pTB. The Tuberculosis patients included in the current study followed a mixed diet, majorly consuming sea foods. BMI of the patients didn’t show any improvement post-treatment. TB patients were 11 and 7 times had a BMI <18.5 and mid-arm circumference < 24 cm respectively in a study conducted in India.19 Patients in the present study also had BMI categorizing them as underweight and malnourished. Reduced appetite and malabsorption of proteins and micronutrients leads to muscle wasting20 in TB. Deficiency of micronutrients playing diverse metabolic functions in the body is the commonest cause of secondary immunodeficiency leading to morbidity and mortality in tuberculosis. It has been reported that there is a linear increase in weight soon after the initiation of therapy, 21 this however was not observed in our study. There was no significant improvement in the BMI post-treatment despite education on the need for a balanced and nutritious diet.
According to the kit insert, the normal reference range of zinc is 60-120 µg/dl and that of copper is 80-155 µg/dl. All the patients included in the study consumed a mixed diet (data not presented) and Mangalore being a coastal region has predominant seafood eaters. Consumption of zinc and copper-rich fish and shellfish possibly explains their adequate serum concentrations.22 Contrary to this finding, different studies23 conducted in Indonesia, England, other parts of India, and Japan reported low levels of micronutrients in active pTB patients. Poor nutritional status, malabsorption, and increased metabolism of several micronutrients lead to their deficiency.24 The disease-induced production of cytokines and acute phase protein synthesis will inhibit the synthesis of serum albumin and cause intense shifts in the concentration of some indispensable micronutrients in plasma.20
Lower baseline levels of zinc have been explained by the preferential movement of zinc to affected tissues from plasma, reduced synthesis of the zinc carrier protein in the liver, or raised metallothionein synthesis.25Anti-tubercular therapy (ATT) for two months, resulting in a slight elevation of Zn levels, indicating that plasma zinc levels may serve as a marker for assessing the disease severity and the patient’s response to therapy.23, 26, 27 Furthermore, it was reported that supplementation of zinc and vitamin A to adult TB patients would hasten the elimination of Mycobacterium, thus leading to quick cure in them.28 Consistent with these reports, we found an insignificant elevation in the serum zinc concentration post-treatment. Zinc is an antioxidant and anti-inflammatory agent. It acts as a molecular signal for the immune cells and the transcription factors involved in the gene expression of inflammatory cytokines.11 Zinc helps in the modulation of cytokine release and induction of proliferation by acting as a cofactor for thymulin and adequate intake of Zinc helps in TH1 response.9 Supplementation of zinc in the elderly has shown the reduced occurrence of infections and reduced both the generation of inflammatory cytokines and oxidative stress.11 Zinc supplementation also increases components of innate immunity like phagocytosis by neutrophils and macrophages, the activity of natural killer cells and oxidative burst generation, antibody response, and cytotoxic T cells.9
Copper is a vital component of several structural enzymes such as cytochrome oxidase, lysyl oxidase, superoxide dismutase, ceruloplasmin, and metallothioneins that act in redox reactions.29 Surplus amounts are toxic to microbes and could inhibit the growth of M. tuberculosis.30 TB in pigs was controlled by the elevation of copper levels in lung lesions.31 The role of copper in pTB has been justified both as an oxidant and as part of antioxidant systems and hence its functions are complex.32 Consensus regarding the levels and mechanism of action needs further elucidation. The ratio of copper/zinc and the absolute copper values were significantly elevated in the tuberculosis patients as compared to controls. 33 We found a statistically significant elevation in the copper levels after 2 months of DOTS treatment. Growth of Mycobacterium tuberculosis necessitates the requirement of two of the copper-containing enzymes such as cytochrome -c oxidase and Cu/Zn-superoxide dismutase. Among hosts, copper acts as a poison in macrophages by damaging the bacterial iron-sulfur clusters of enzymes and displacing cofactor ions like zinc and manganese.34
Post DOTS therapy for two months, serum Zn levels as well as copper levels increased in this study. The difference in the observed findings from previous reports could be attributed to the diverse food habits of different patients and their varied socioeconomic backgrounds. The increase could also be a result of stress on nutrition, adherence to treatment, and surveillance and monitoring at various levels by the government-implemented Revised National Tuberculosis Control Programme. Some patients were taken from a TB Sanatorium where they were institutionalized. We ensured adherence to treatment by frequently calling the patients and educating them about the nutritional requirements.
The sputum negativity in the patients who were followed up was 69% and another 12% of the patients showed scanty acid-fast bacilli. It can be safely assumed that the response to treatment was 81% which exerts the importance of the raised copper and zinc levels in these patients. The response to therapy is similar to other studies.35, 36 Supplementation of copper and zinc may be beneficial to patients with pTB in achieving sputum negativity at the earliest.
However, it would be worthwhile to study the impact of these minerals in those patients who remained sputum positive even after intensive phase therapy for 2 months.
Despite the small number of participants, the strength of the study lies in its prospective follow-up design. Although the role of adequate nutrition is emphasized, the contribution of micronutrients in the development, progression, and prognosis of the disease has not been well established. This study points to the importance of maintaining serum copper and zinc levels during the intensive two months anti-tubercular therapy phase in pulmonary tuberculosis patients.
Since it was a time-bound study and only the freshly diagnosed uncomplicated tuberculosis patients were chosen, we could include 39 cases and follow up only 31 cases. Based on the results, the authors aim to take up a follow-up study where the patient’s treatment will be augmented with zinc and copper to better understand their efficacy.
Conclusion
Despite the habitual consumption of seafood and other non-vegetarian food, there was no significant improvement in the nutritional status as evidenced by BMI. Copper and zinc are known to play important roles in immunity and infection control. Supplementation with these may be beneficial in enhancing the response to treatment and ensuring early sputum negativity in tuberculosis patients. Optimization of the levels to bring on a favorable response from the host is required.
Acknowledgement
We would like to thank ICMR-STS for funding this research work.
Conflicts of Interest
The authors declare no conflicts of interest.
Funding Sources
ICMR-STS funded this research work. Refernce ID: 2018-01601.
References
- World Health Organisation. Global tuberculosis report 2020. http://www.who.int/tb/publications/global_report/en/.
- Kirenga B.J., Ssengooba W., Muwong C., Nakiyingi L., Kyaligonza S., Kasozi S. Tuberculosis risk factors among tuberculosis patients in Kampala, Uganda: implications for tuberculosis control. BMCPublic Health. 2015;15:13. doi: 10.1186/s12889-015-1376-3. doi: 10.1186/s12889-015-1376-3.
CrossRef - Restrepo B.I. Diabetes and Tuberculosis. Microbiol Spectr.2016;4(6):10.1128/microbiolspec.TNMI7-0023-2016. doi: 10.1128/microbiolspec.TNMI7-0023-2016.
CrossRef - Silva D.R., Muñoz-Torrico M., Duarte R., Galvão T., Bonini E.H., Arbex F.F. Risk factors for tuberculosis: diabetes, smoking, alcohol use, and the use of other drugs. J Bras Pneumol. 2018; 44:145-152. doi: 10.1590/s1806-37562017000000443.
CrossRef - Gupta K.B., Gupta R., Atreja A., Verma M., Vishvkarma S. Tuberculosis and nutrition. Lung India. 2009 ; 26:9-16. doi: 10.4103/0970-2113.45198.
CrossRef - Bahi G.A., Boyvin L., Meite S., M’Boh G.M., Yeo K., N’Guessan K.R. Assessment of serum copper and zinc concentration,and the Cu/Zn ratio determination in patients with multidrug resistant pulmonary tuberculosis(MDR-TB) in Cote d’lvoire. BMC Infect dis.2017; 17:257. doi: 10.1186/s12879-017-2343-7.
CrossRef - Vignesh K.S., Deepe S.G. Metallothioneins: Emerging Modulators in Immunity and Infection. Int J Mol Sci. 2017; 18: 2197. doi: 10.3390/ijms18102197.
CrossRef - Wessels I., Maywald M., Rink L. Zinc as a Gatekeeper of Immune Function. Nutrients.2017; 9:1286. doi: 10.3390/nu9121286.
CrossRef - Prasad R., Ahmad I., Kushwaha R.A.S., Gupta M.K., Saleem M.Vitamin A and Zinc Alter the Immune Function in Tuberculosis. Kuwait Medical Journal. 2012; 44:183-189.
- Edem V.F., Ige O., Arinola O.G. Plasma vitamins and essential trace elements in newly diagnosed pulmonary tuberculosis patients and at different durations of anti-tuberculosis chemotherapy. Egyptian Journal of Chest Diseases and Tuberculosis. 2015; 64:675-679. org/10.1016/j.ejcdt.2016.02.001
CrossRef - Prasad A.S. Zinc: An antioxidant and anti-inflammatory agent: Role of zinc in degenerative disorders of aging. J Trace Elem Med Bio. 2014; 28:364-371. doi: 10.1016/j.jtemb.2014.07.019.
CrossRef - Bonaventura P., Benedetti G., Albarede F., Miossec P. Zinc and its role in immunity and inflammation. Autoimmun Rev. 2015; 14:277-85. doi: 10.1016/j.autrev.2014.11.008
CrossRef - Hojyo S., Fukada T. Roles of Zinc Signaling in the Immune System. J Immunol Res. 2016; 2016:6762343. doi: 10.1155/2016/6762343.
CrossRef - Niederweis M., Wolschendorf F., Mitra A., Neyrolles O. Mycobacteria, Metals, and the Macrophage. Immunol rev. 2015; 264:249-263. doi: 10.1111/imr.12265.
CrossRef - Neyrolles O., Mintz E., Catty P. Zinc and copper toxicity in host defense against pathogens: Mycobacterium tuberculosis as a model example of an emerging paradigm. Front Cell Infect Microbiol. 2013; 3:89. doi: 10.3389/fcimb.2013.00089.
CrossRef - Nguyen G.T., Green E.R., Mecsas J. Neutrophils to the ROScue: Mechanisms of NADPH Oxidase Activation and Bacterial Resistance. Front Cell Infect Microbiol. 2017;7:373. doi: 10.3389/fcimb.2017.00373.
CrossRef - Djoko K.Y., Ong C.Y., Walker M.J., McEwan A.G. The Role of Copper and Zinc Toxicity in Innate Immune Defense against Bacterial Pathogens. J BiolChem.2017;290 (31):18954-18961. doi: 10.1074/jbc.R115.647099.
CrossRef - Shi X., Darwin K.H. Copper homeostasis in Mycobacterium tuberculosis. Metallomics. 2015; 7:929-34. doi: 10.1039/c4mt00305e.
CrossRef - Shetty N., Shemko M., Vaz M., D’Souza G. An epidemiological evaluation of risk factors for tuberculosis in South India: A matched case control study. Int J Tuberc Lung Dis.2006;10:80-6. PMID: 16466042.
- Gupta K.B., Gupta R., Atreja A., Verma M., Vishvkarma S.Tuberculosis and nutrition. Lung India. 2009; 26:9-16. doi: 10.4103/0970-2113.45198.
CrossRef - Vasantha M., Gopi P.G., Subramani R. Weight gain in patients with tuberculosis treated under directly observed treatment short-course (DOTS). Indian J Tuberc. 2009; 56:5-9. PMID: 19402266.
- Gombart A.F., Pierre A., Maggini S. A Review of Micronutrients and the Immune System-Working in Harmony to Reduce the Risk of Infection. Nutrients. 2020; 12:236. doi: 10.3390/nu12010236.
CrossRef - Venugopal V., Gopakumar K. Shellfish: Nutritive Value, Health Benefits, and Consumer Safety. Compr Rev Food Sci Food Saf. 2017; 16:1219-1242. doi: 10.1111/1541-4337.12312.
CrossRef - Hennigar S.R., Kelley A.M., McClung J.P. Metallothionein and Zinc Transporter Expression in Circulating Human Blood Cells as Biomarkers of Zinc Status: a Systematic Review. Adv Nutr. 2016; 7:735-46. doi: 10.3945/an.116.012518.
CrossRef - Beisel W.R. Metabolic responses of the host to infection. In: Textbook of Pediatric Diseases (Feigin R.D. & Cherry J.D., eds.). Saunders, Philadelphia, pp. 54-69,1998.
- Rockwood N., du Bruyn E., Morris T., Wilkinson R.J. Assessment of treatment response in tuberculosis. Expert Rev Respir Med. 2016; 10:643-54. doi: 10.1586/17476348.2016.1166960.
CrossRef - King J.C., Brown K.H., Gibson R.S., Krebs N.F., Lowe N.M., Siekmann J.H. Biomarkers of Nutrition for Development (BOND)-Zinc Review. J Nutr. 2015; 146:858S-885S. doi: 10.3945/jn.115.220079.
CrossRef - Keflie T.S., Samuel A., Woldegiorgis A.Z., Mihret A., Abebe M., Biesalski H.K. Vitamin A and zinc deficiencies among tuberculosis patients in Ethiopia. J Clin Tuberc Other Mycobact Dis. 2018; 12:27-33. doi: 10.1016/j.jctube.2018.05.002.
CrossRef - Grammer T.B., Kleber M.E., Silbernagel G., Pilz S., Scharnagl H., Lerchbaum E. Copper, ceruloplasmin, and long-term cardiovascular and total mortal- ity (the Ludwigshafen Risk and Cardiovascular Health Study). Free Radic Res. 2014; 48:706–15. doi: 10.3109/10715762.2014.901510.
CrossRef - Neyrolles O., Wolschendorf F., Mitra A., Niederweis M. Mycobacteria, metals, and the macrophage. Immunol Rev. 2015; 264:249-63. doi: 10.1111/imr.12265.
CrossRef - Shah S., Dalecki A.G., Malalasekera A.P., Crawford C.L., Michalek S.M., Kutsch O. 8-Hydroxyquinolines are boosting agents of copper-related toxicity in mycobacterium tuberculosis. Antimicrob Agents Chemother. 2016;60:5765–76. doi: 10.1128/AAC.00325-16.
CrossRef - Qi C., Wang H., Liu Z., Yang H. Oxidative Stress and Trace Elements in Pulmonary Tuberculosis Patients During 6 Months Anti-tuberculosis Treatment. Biol Trace Elem Res. 2021; 199:1259-1267. doi: 10.1007/s12011-020-02254-0.
CrossRef - Kassu A., Yabutani T., Mahmud Z.H., Mohammad A., Nguyen N., Huong B.T. Alteration in serum levels of trace elements in tuberculosis and HIV infection. Eur J Clin Nutr. 2006; 60:580–6. doi: 10.1038/sj.ejcn.1602352.
CrossRef - Rowland J.L., Niederweis M. Resistance mechanisms of Mycobacterium tuberculosis against phagosomal copper overload. Tuberculosis (Edinb). 2012; 92(3):202-10. doi: 10.1016/j.tube.2011.12.006.
CrossRef - Kayigamba F.R., Bakker M.I., Mugisha V., Gasana M., Schim van der Loeff M.F. Sputum completion and conversion rates after intensive phase of tuberculosis treatment: an assessment of the Rwandan control program. BMC Res Notes. 2012; 16;5:357. doi: 10.1186/1756-0500-5-357.
CrossRef - Bawri S., Ali S., Phukan C., Tayal B., Baruwa P. A study of sputum conversion in new smear positive pulmonary tuberculosis cases at the monthly intervals of 1, 2 & 3 month under directly observed treatment, short course (dots) regimen. Lung India. 2008;25:118-23. doi: 10.4103/0970-2113.44122.
CrossRef
Accepted on: 31 Oct 2022
Second Review by: Rafaella de Paula Paseto Fernandes
Final Approval by: Dr. Jiwan S. Sidhu





Web of Science Coverage
Emerging Sources Citation Index (ESCI)
2024 Journal Impact Factor: 1.1
Scopus Journal Metrics
CiteScore 2025: 2.6
CiteScore Details
Sustainable Nutrition: Food Systems, Nutrient Retention, and Public Health Impact
![]()
This journal is a member of, and subscribes to the principles of, the Committee on Publication Ethics (COPE)








