Oral Carbohydrate Administration was Suitable for Cesarean Section–A Systematic Review and Meta-Analysis of Randomized Trials
 , , Li Bo Wang3, Zhi Qin Wang4, Zhen Feng Zhou5, , Meng Yan Xu6 and Gui Juan He1
, , Li Bo Wang3, Zhi Qin Wang4, Zhen Feng Zhou5, , Meng Yan Xu6 and Gui Juan He1 1School of Nursing, Zhejiang Chinese Medical University, Hangzhou, China.
2Department of Surgery, Hangzhou Women’s Hospital (Hospital Maternity and Child Health Care Hospital), Hangzhou, China.
3Department of Obstetrics and Gynecology, Hangzhou Women’s Hospital, Hangzhou, China
4Department of Pharmacy, Zhejiang Provincial Xinhua Hospital, Hangzhou, China.
5Department of Anesthesiology, Hangzhou Women’s Hospital, Hangzhou, China,
6Department of Nursing Hangzhou Women’s Hospital, Hangzhou, China.
Corresponding Author E-mail: songxh8866@163.com
DOI : http://dx.doi.org/10.12944/CRNFSJ.11.2.01
Download this article as:
![]()
The use of carbohydrate (CHO) drinks prior to elective cesarean section has gained momentum, but its effect on maternal and neonatal outcomes remains controversial. The aim of this meta-analysis was to assess the effect of an oral CHO load prior to cesarean delivery on insulin sensitivity, insulin resistance, maternal glycemia, neonatal glycemia, and breastfeeding. As of May 21, 2023, we searched through five databases for English-language experimental studies on pre-cesarean oral CHO. A total of 3,940 citations were received, of which seven were selected. The concentrations of CHO used in these studies ranged from 5.9% to 14.2%, and the amounts used were 300-400 ml. We found that pre-cesarean CHO loading reduced maternal insulin resistance and increased maternal glucose levels. CHO loading activates the insulin pathway of critical en-zymes to some extent, increasing glucose utilization by peripheral tissues and ultimately reducing postop-erative insulin resistance. Of course, this is also beneficial in improving maternal blood sugar. We did not find that CHO increased maternal insulin sensitivity or neonatal blood glucose levels. Future prospective randomized controlled trials can use nutritional load to increase colostrum production after Caesarean sec-tion to enhance the confidence of these mothers in breastfeeding. In addition, our preoperative beverage could be more individualized to accommodate diabetic women.
KEYWORDS:Breastfeeding neonatal immunity; Cesarean section; Carbohydrate loading; Insulin resistance
Introduction
Since the 1980s, clinical trials have been challenging the traditional practice of requiring all patients to have scheduled surgery from midnight. 1 During abdominal surgery, the Enhanced Recovery After Surgery (ERAS®) Society recommends using clear fluids for at least 2 hours and solid fluids for 6 hours. 2 The rationale for preoperative oral carbohydrate (CHO) loading is to prevent harmful catabolic alterations associated with fasting, for example, glycogenolysis, decreased insulin sensitivity, and proteolytic metabolism.3 Insulin resistance can lead to hyperglycemia and reduced tissue responsiveness to insulin bioactivity. This metabolic problem leads to a status of catabolism and can contribute to increased morbidity and prolonged hospitalization. 4-7 Women undergoing elective cesarean delivery require prolonged fasting, which is thought to be a factor in the development of neonatal hypoglycemia. 8 In addition, women who underwent elective cesarean delivery lactated significantly less in the early postpartum period than women with spontaneous vaginal delivery. 9 Therefore, the incidence of hypoglycemia is higher in newborns delivered by cesarean section than in newborns delivered spontaneously. Hypoglycemia directly affects the metabolism of neonatal brain tissue, which in turn severely affects its related physiological activities, causing irreversible and permanent damage, and the symptoms of hypoglycemia lasting 30 minutes can lead to brain cell death. 10 One way to improve maternal and neonatal prognosis after cesarean delivery is to optimize patient nutrition prior to elective surgery through preoperative oral CHO loading therapy as part of the Enhanced Recovery After Cesarean (ERAC) pathway. 11-14
The American Society of Anesthesiologists recommends “Drinking transparent liquids 2 hours before the induction of anesthesia for those undergoing elective cesarean section without complications”. 15 Gastric emptying tests 16 have shown that less than 400 ml of oral CHOs 2 hours before cesarean section is permissible. Types of carbohydrates used in the current study, 17-23 including different concentrations of sugar water and Gatorade, among other options.
Numerous studies have been conducted on CHO loading, with a variety of outcomes, but their quality is not satisfactory. Moreover, it is controversial whether oral CHO loading before cesarean delivery improves maternal insulin sensitivity and reduces insulin resistance, maternal glycemia, neonatal glycemia, and breastfeeding. As a result, a meta-analysis of studies focused on the effects of pre-operative treatment of carbohydrates on clinical and metabolic parameters in cesarean section is required. Meanwhile, this is the first meta-analysis related to oral carbohydrate administration during cesarean section.
Specific Aims
This review evaluated the available evidence to determine whether oral CHO beverages should be consumed before cesarean delivery. Our evaluation was based on evidence, including the stability of maternal blood sugar levels and the strength of neonatal blood sugar levels, postoperative insulin sensitivity increases, postoperative breastfeeding rate increases, and hospital stays were shortened.
Information and methodology
A systematic evaluation and meta-analysis of randomized controlled trials (RCTs) were conducted in accordance with the Preferred Reporting Elements for Systematic Evaluation and Meta-analysis (PRISMA) guidelines.24 The notice was recorded at https://www.crd.york.ac.uk /PROSPERO/ and bears ID CRD42022323953.
Search strategies and inclusion criteria
Up to 21/05/2023, a systematic and comprehensive literature search was conducted using the Pub-Med/EMBASE/Cochrane Library/Clinical Trials /Web of Science databases. Two authors separately searched for English articles. In addition, terms such as alternative words, carbohydrate acronym (CHO), British or American alternative spellings, keywords, free text, and Medical Subject Headings (MeSH) were used to enhance the search further (see Appendix 1). Duplicate studies, studies with incomplete experimental data, animal studies, abstracts only, and reviews were excluded. The following inclusion criteria were applied:
RCTs;
Women who were over 18 years of age and were undergoing elective cesarean section;
Populations containing >30 patients;
Experiments that did not encourage drinking at midnight;
Interventions include taking more than 50ml of carbohydrates 2 to 3 hours before cesarean section;
Randomly assigned carbohydrate load and fasting/placebo (e.g., water), used for short periods and with clear usage.
The primary outcome measures were maternal glucose levels, neonatal glucose levels, insulin resistance, insulin sensitivity, and postoperative breastfeeding.
The secondary outcome measures were as follows: Length of hospitalization, the incidence of postoperative nausea and vomiting (PONV), preoperative gastric emptying time, grip strength, urinary ketone levels, body temperature, preoperative maternal hunger and thirst anxiety, and postoperative complications. Studies that were not included were duplicate publications, studies without full text, studies with incomplete experimental data, animal studies, trial registries, and studies that used different methods to evaluate the same outcomes.
Data Extraction
Two of us (Hu Y, Song xih) independently classified the interventions, and discrepancies were resolved by a third reviewer (Wang zq). When further information was needed to determine eligibility, we contacted the trial authors. The procedure of literature screening is given in Figure 1. Table T1 (in supplementary materials) displays the risk of bias assessment for each study (listed in Table 1) , and Table 1 displays the maternal characteristics.
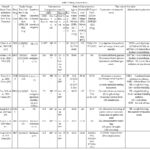 |
Table 1: Study characteristics. |
Outcomes
Primary outcomes: Maternal glucose levels, neonatal glucose levels, insulin resistance, insulin sensitivity, and postoperative breastfeeding.
Secondary outcomes: Length of stay, rate of PONV, preoperative gastric emptying time, grip strength, urinary ketone levels, body temperature, preoperative maternal hunger and thirst anxiety, and postoperative complications.
Data Synthesis and Statistic Analyzing
Review Manager 5.3 software was utilized in this meta-analysis. All analyses were two-tailed and had an alpha of 0.05. Categorical data were pooled as risk ratios (RRs) with 95% confidence intervals. The results for continuous data are summarized as the mean differences (MD, with units) or standardized mean differences (SMDs, denoted as standard deviations) with 95% confidence intervals, when appropriate. Categorical data were pooled as RRs with 95% confidence intervals. Heterogeneity was assessed using the I2 statistic, with an I2 greater than 50% indicating significant heterogeneity. When I2 was more excellent than 50%, random effects meta-analysis was used first. The SMD was used when studies assessing the same outcome used different measures or when the results differed significantly due to differences in the study population. When the SMD was not appropriate, the raw results were reported as descriptive expressions.
Risk of Bias
The Cochrane Risk of Bias Instrument guidelines were used to assess each study, which included randomization, allocation order, participant blinding, outcome assessment blinding, reporting of incomplete data, selective reporting, and other biases. Our assumption for risk of bias assessment was that the study’s quality increases with the number of evaluations that indicate a low risk of bias.
GRADE (Recommendation Grading, Assessment, Establishment, and Estimation)
The quality of evidence was assessed using the GRADEpro GDT software (https://gdt.gradepro.org/app/). The evaluation results were categorized by the quality of the evidence, which was categorized as high, medium, low, and deficient quality. The results of the evidence evaluation have been expressed in Table T2 (in supplementary materials) Figures 2 and 3 show the results of all other meta-analyses. The results of the other non-meta-analyses extracted by the authors are described in Tables 2 and 3.
The evaluation of evidence quality (GRADE)
As all studies were RCTs, the results were first considered to be of high quality. Comparing the CHO and placebo groups, the evidence was increased in one and low in the other. The smaller sample size was the large confidence interval and significant heterogeneity.
Results
Search Results
The database searched 3,940 articles; 3,919 articles were retained after removing duplicates and screening them by title and abstract. A total of 21 full-text articles were assessed as eligible, of which 14 were substantially removed after comparison with the inclusion and exclusion criteria. Seven full-text articles were included for analysis (Figure 1).
Table 2. Qualitative clinical outcomes were excluded from the meta-analysis. The counts are the number of patients.
|
Outcomes |
Experimental Group |
Placebo Group |
Fasting Group |
References/Country |
|||
|
Case (%) |
n |
Case |
n |
Case (%) |
n |
||
|
Infant blood glucose |
63% |
15 |
50% |
17 |
65% |
15 |
Wendling et al., 2020 USA [25] |
|
Hypotension |
5 |
39 |
6 |
40 |
7 |
39 |
Yang et al., 2021 China [26] |
|
Shivering |
10 |
39 |
11 |
40 |
21 |
39 |
Yang et al., 2021 China [26] |
|
Urinary ketone level |
18% |
91 |
– |
– |
61% |
93 |
Clark et al., 2019 UK [27] |
|
Grasp strength |
Only image date range |
Clark et al., 2019 UK [27] |
|||||
|
Intraoperative vomiting |
Total: 4 |
Total: 47 |
Wendling et al., 2020 USA [25] |
||||
|
Only image date range |
Shi et al., 2020 China [31] |
||||||
|
Only image date range |
Shi et al., 2020 China [31] |
||||||
|
Anxiety |
Only image date range |
Shi et al., 2020 China [31] |
|||||
Table 3: Quantitative clinical outcomes were not part of the meta-analysis. The definition of values was either the standard deviation (SD) or median (interquartile range (IQR).
|
Outcomes |
Experimental Group (CHO) |
Placebo Group |
Fasting Group |
References/Country |
|||
|
Mean (SD); Median (IQR) |
n |
Mean (SD); Median (IQR) |
n |
Mean (SD); Median (IQR) |
n |
||
|
Hospital length of stay; Days (hours) |
39 h [27-47, 11-116] |
91 |
– |
– |
43 h [27-48, 12-240] |
93 |
Clark et al., 2019 UK [27] |
|
4 (4–4) |
39 |
4 (4–4) |
40 |
4 (4–4) |
39 |
Yang et al., 2021 China [26] |
|
|
Thirst |
5 [3-6, 0-8] |
91 |
– |
5 [4-6, 0-10] |
93 |
Clark et al., 2019 UK [27] |
|
|
OR = 5.5, 95% CI 1.2–24.8 |
15 |
NS |
NS |
Wendling et al., 2020 USA [25] |
|||
|
2 (1) |
43 |
2 (2) |
42 |
Liu et al., 2021 China [29] |
|||
|
0 (0–0) |
39 |
0 (0–0) |
40 |
3 (0–3) |
39 |
Yang et al., 2021 China [26] |
|
|
Hunger |
5 [3-7, 0-10] |
91 |
– |
6 [4.25-8.0-10] |
93 |
Clark et al., 2019 UK [27] |
|
|
NS |
OR = 3.1, 95% CI 0.7-12.6 |
17 |
OR = 5.5, 95% CI 1.1-28.4 |
15 |
Wendling et al., 2020 USA [25] |
||
|
2 (2) |
43 |
5 (2) |
42 |
Liu et al., 2021 China [29] |
|||
|
0 (0–0) |
39 |
0 (0–3) |
40 |
1 (0–3) |
40 |
Yang et al., 2021 China [26] |
|
|
Anxiety |
3 (3.57) |
91 |
4 (4.71) |
93 |
Clark et al., 2019 UK [27] |
||
|
1 (3.3) |
39 |
3 (10.3) |
40 |
1 (3.5) |
39 |
Yang et al., 2021 China [26] |
|
|
Body temperature (core temperature) |
36.78 (0.31) |
39 |
36.63 (0.41) |
40 |
36.68 (0.46) |
39 |
Yang et al., 2021 China [26] |
|
Early neonatal feeding indicators |
|||||||
|
First breastfeeding (min) |
27.47 (11.51) |
45 |
51.96 (20.20) |
46 |
Fard et al., 2017 Iran [30] |
||
|
Feeding frequency |
6.14 (0.55) |
45 |
4.82 (0.46) |
46 |
Fard et al., 2017 Iran [30] |
||
|
The mean duration of breastfeeding (min) |
116.48 (19.68) |
45 |
82.13 (12,40) |
46 |
Fard et al., 2017 Iran [30] |
||
|
Ultrasonic recording of gastric antrum cross-section area or gastric volume (2 h after feeding) |
159.36 ± 15.59 mm2 |
25 |
150.88 ± 19.01 mm2 |
25 |
– |
– |
Shi et al., 2020 China [31] |
|
Maternal blood glucose |
4.2 (3.6–4.7) |
30 |
4.3 (3.9–4.7) |
29 |
4.4 (3.9–4.8) |
29 |
He et al., 2021 China [28] |
|
Insulin resistance |
3.802±0.346 |
25 |
5.107±0.371 |
25 |
4.92±0.52 |
25 |
Shi et al., 2020 China [31] |
|
Infant blood glucose (umbilical cord blood glucose) |
3.2 (2.9–3.7) * |
30 |
3.0 (2.8–3.3) |
29 |
3.0 (2.8–3.2) |
29 |
He et al., 2021 China [28] |
|
HOMA-IR |
|||||||
|
Pre-operation |
2.1 (1.6-2.9) |
30 |
2.2 (1.6-2.9) |
29 |
2.2 (1.6-2.9) |
29 |
He et al., 2021 China [28] |
|
Post-operation |
0.9(0.5-1.5) |
30 |
1.6 (0.8-2.6) |
29 |
1.6 (0.9-2.3) |
29 |
He et al., 2021 China [28] |
|
Insulin |
|||||||
|
Pre-operation |
11.3 (8.9-14.8) |
30 |
11.5 (9.0-14.6) |
29 |
11.6 (9.0-14.6) |
29 |
He et al., 2021 China [28] |
|
Post-operation |
4.6 (2.8-7.6) |
8.0 (4.5-13.3) |
8.6 (5.0-11.5) |
||||
The study, Patient, and Treatment Characteristics
The sample RCTs involved 688 women. These experiments were all double-blinded 25,29 and triple-blinded trials; 28,31 one of them, 27 was a single-blinded trial, and the others were not described. Women received 200 to 400 mL of a beverage with a CHO concentration of 5% to 14.2% at one or different times prior to cesarean delivery. The risk of bias assessment scores ranged from a maximum of 7 to a minimum of 3.
CHO Effects on Clinical and Biochemical Parameters
The primary data of the meta-analysis included insulin sensitivity, insulin resistance, maternal glucose levels, and neonatal glucose levels—none of the secondary outcomes needed more lysis.
The evaluation metrics showed that CHO loading reduced insulin resistance (n = 100, SMD = -1.23, 95% confidence interval (CI) = -1.39 to-1.08, p<0.00001). However, there was no statistical significance regarding increased insulin sensitivity (p=0.18).
In terms of maternal and neonatal glucose levels, the results showed improved maternal glucose levels (n = 135, SMD =0.71, 95% confidence interval (CI) = 0.05 to 1.38, p = 0.04), with no significant difference in neonatal glucose outcomes (p = 0.45). Since I2 =71%, the sensitivity analysis performed in Liu Ning’s study had a substantial effect on the results, which may be because the study population in the 29 groups included diabetic women.
Figures 2-3 show the results of all other meta-analyses. The results of other non-meta-analyses extracted by the authors are described in Tables 2 and 3.
Quality Assessment of Evidence (GRADE)
As all studies were investigational clinical trials (RCTs), the findings were initially considered to be high quality evidence. However, the evidence was high in one study and low in another. The reason was due to smaller sample sizes with large confidence intervals and significant heterogeneity.
 |
Figure 1: The flowchart depicting the search strategy and study selection for Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) study. |
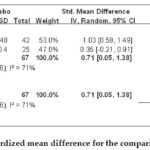 |
Figure 2: One effect size standardized mean difference for the comparison of maternal glucose levels. |
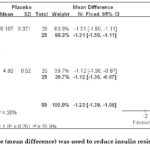 |
Figure 3: An effect size (mean difference) was used to reduce insulin resistance for comparison. |
Discussion
Our study suggests that preoperative CHO loading benefits women undergoing cesarean delivery. To our knowledge, this study is the first to observe oral CHO loading prior to cesarean delivery. This meta-analysis included RCTs involving 688 women.
The results suggest that CHO in women undergoing cesarean section may not shorten the length of hospital stay compared to patients undergoing abdominal or cardiac surgery, 32,33 as the length of stay after cesarean section is not long and does not fit as a primary indicator. This has led to insufficient evidence and support in this area. However, there is inadequate evidence about whether CHO loading improves neonatal blood glucose levels or increases maternal insulin sensitivity. However, the addition of CHOs in this study was beneficial in enhancing maternal blood glucose levels and reducing insulin resistance. The reduction in insulin resistance is in keeping with the results of the meta-analysis re-ported by Ricci et al. 32 Placental lactogens, estrogen, progesterone, tumor necrosis factor, leptin, and maternal adrenocorticotropic hormone, which are all synthesized by the placenta, have antagonistic effects on insulin, making maternal tissues less sensitive to insulin. 34 Studies have shown that preoperative oral CHO loading activates the insulin path-way on key enzymes (P13K and PKB) to some extent, which increases surgical and postoperative insulin sensitivity and promotes Glu T4 in-version in peripheral tissues, thus increasing glucose utilization by peripheral tissues and ultimately reducing postoperative insulin resistance. 35 The differences in the maternal insulin sensitivity results may be due to the wide variation in subjects, while only one study included diabetic women. Concerning neonatal glucose levels, some trials had problems setting the time points for monitoring, resulting in neo-natal glucose results that were not significant in this study. According to neonatal data, 10,12,36 high-risk neonates should have their blood glucose measured within half an hour to one hour after birth, and normal neo-nates should have their blood glucose measured within one hour to two hours after birth. If the evidence for the effect of CHOs on maternal and neonatal glycemia is insufficient, it may lead to a change in the direction of our study. However, we also lack suitable preoperative beverages for pregnant women with diabetes. Some low GI sugars are ideal for diabetic patients and are used as preoperative beverage sugars. Low-GI diets effectively lower glycosylated hemoglobin (HbA1c), leading to more stable blood glucose concentrations. Such personalized preoperative beverage customization should be pursued in the future.
Although the use of CHOs before cesarean delivery has shown a relative improvement in breastfeeding rates, this can only be explained by the fact that the sugar in CHOs improves mothers’ moods, which affects their breast milk. This is because sugar has no significant effect on the release of prolactin. A high-protein diet regulates prolactin and the release of ACTH by providing synthetic substrates for catecholamine and serotonin. It may indirectly affect the function of the hypothalamic-pituitary system by altering cholecystokinin.37 Mid-gestation involves the accumulation of colostrum through milk follicles,38 and in late gestation, the ductal system continues to dilate, expand and fill 39 with colostrum. Cesarean section is a common risk factor for different immune-related diseases, including asthma and leukemia. 40-44 Further research has shown that some cytokines are only present in colostrum, such as stem cell generation factor and tumor necrosis factor b. Breast milk contains various cytokines, which may even affect infants’ long-term prognosis and disease.37 Breast milk contains various cytokines, which may even affect infants’ long-term prognosis and disease. The prolonged interruption of breastfeeding during the perioperative period of a cesarean section and the inability of the infant to suckle during the operation is one of the reasons for the relative inadequacy of supplemental milk after a cesarean section. Now there is a kind of hydrolyzed Whey protein, which is easy to digest and can be used before a cesarean section. Therefore, by preloading protein before the operation to increase colostrum storage in the breast duct and increasing prolactin level early after the operation, it is helpful to regulate colostrum deficiency after a cesarean section. Our preoperative beverages should be more functional and targeted.
The limitations of meta-analysis
This study has some potential limitations. Most of the included studies were studies of moderate quality, and some needed to be better formulated in a blinded manner. Although we excluded some low-quality literature, there was significant heterogeneity, and no funnel plot was used for publication bias analysis, which affected the reliability of the findings. The search language was limited to English, which may have led to publication bias.
Implications for Future Research
Protein preloading may be required prior to cesarean delivery to in-crease maternal postoperative colostrum production. In addition, our preoperative drinks can be more personalized to accommodate diabetic women. Thus, our preoperative beverages can be targeted to promote and improve function. This may be beneficial to increase mothers’ confidence in breastfeeding after Caesarean section and even promote pure breastfeeding after Caesarean section. Furthermore, the perioperative period of cesarean delivery is an indivisible whole, and optimal nutritional support for the mother is as uninterrupted a process as possible. The types and concentrations of proteins that can be added to CHOs and are suitable for use before and after cesarean delivery deserve further exploration in future studies.
Conclusions
In summary, CHO loading before cesarean delivery reduced insulin resistance and improved maternal glucose levels. However, it did not affect neonatal blood glucose levels, and there is insufficient evidence regarding the improvement of other measures. This preoperative beverage containing sugar can be used in pregnant women with gestational diabetes. We are trying to move toward such personalization in providing treatment. It is recommended that protein should be preloaded before cesarean delivery and used early in the postoperative period to reduce the duration of the nutritional interruption, as well as to stimulate prolactin and reduce the incidence of locational deficiency after cesarean delivery.
Conflict of Interest
There are no conflict of interest.
Funding Sources
The funding for this study comes from the Hangzhou Medical and Health Technology Project “Research on the Effect of Perioperative Application of Hydrolyzed Whey Protein on Postoperative Prolactin in Women Undergoing Selective Cesarean Section.” The grant no. is A20231026.
References
- Maltby J.R., Sutherland A.D., Sale J.P., Shaffer E.A. Preoperative oral fluids: Is a five-hour fast justified prior to elective surgery? Anesth. Analg. 1986;65(11):1112-1116.
CrossRef - Gustafsson U.O., Scott M.J. Schwenk W., et al. Guidelines for perioperative care in elective colonic surgery: Enhanced Recovery After Surgery (ERAS(®)) Society recommendations. World J. Surg. 2012;31(6):783-800.
CrossRef - Pogatschnik C., Steiger E. Review of preoperative carbohydrate loading. Nutr. Clin. Pract. 2015;30(5):660-664.
CrossRef - Landau B.R., Wahren J., Chandramouli V., Schumann W.C., Ekberg K., Kalhan S.C. Contributions of gluconeogenesis to glucose production in the fasted state. J. Clin. Invest. 1996;98(2):378-385.
CrossRef - Soeters M.R., Soeters P.B., Schooneman M.G., Houten S.M., Romijn J.A. Adaptive reciprocity of lipid and glucose metabolism in human short-term starvation. Am. J. Physiol. Endocrinol. Metab. 2012;303(12):E1397-E1407.
CrossRef - Van Cromphaut S.J. Hyperglycaemia as part of the stress response: The underlying mechanisms. Best Pract. Res. Clin. Anaesthesiol. 2009;23(4):375-386.
CrossRef - Kotfis K., Szylińska A., Listewnik M., Brykczyński M., Ely E.W., Rotter I. Diabetes and elevated preoperative HbA1c level as risk factors for postoperative delirium after cardiac surgery: An observational cohort study. Neuropsychiatr. Dis. Treat. 2019;15:511-521. Published 2019 Feb 20.
CrossRef - Awad S., Constantin-Teodosiu D., Macdonald I.A., Lobo D.N. Short-term starvation and mitochondrial dysfunction – a possible mechanism leading to postoperative insulin resistance. Clin. Nutr. 2009;28(5):497-509.
CrossRef - Czyż-Szypenbejl K., Mędrzycka-Dąbrowska W.; Kwiecień-Jaguś K., Lewandowska K. The occurrence of postoperative cognitive dysfunction (POCD) – a systematic review. Psychiatr. Pol. 2019;53(1):145-160.
CrossRef - Wu S.M. Neonatal Nutrition. Beijing: People’s Medical Publishing House; 2003.
- Lv Y., Zhu L.L.; Shu G.H. Relationship between blood glucose fluctuation and brain damage in the hypoglycemia neonates. Am. J. Perinatol. 2018;35(10):946-950.
CrossRef - Shao X., Ye H., Qiu X. Practical Neonatology; Beijing:People’s Medical Publishing House; 2011.
- Wilson R.D., Caughey A.B., Wood S.L., et al. Guidelines for antenatal and preoperative care in cesarean delivery: Enhanced recovery after surgery society recommendations (Part 1). Am. J. Obstet. Gynecol. 2018;219(6):523.e1-523.e15.
CrossRef - Caughey A.B., Wood S.L., Macones G.A., et al. Guidelines for intraoperative care in cesarean delivery: Enhanced recovery after surgery society recommendations (Part 2). Am. J. Obstet. Gynecol. 2018;219(6):533-544.
CrossRef - World Health Organization. The Global Prevalence of Anaemia in 2011; World Health Organization: Geneva, 2015.
- Popivanov P., Irwin R., Walsh M., Leonard M., Tan T. Gastric emptying of carbohydrate drinks in term parturients before elective caesarean delivery: an observational study. Int J Obstet Anesth. 2020;41:29-34.
CrossRef - Sada F., Krasniqi A., Hamza A., Gecaj-Gashi A., Bicaj B., Kavaja F. A randomized trial of preoperative oral carbohydrates in abdominal surgery. BMC Anesthesiol. 2014;14:93. Published 2014 Oct 17.
CrossRef - Vermeulen M. A., Richir M. C., Garretsen M. K., et al. Gastric emptying, glucose metabolism and gut hormones: evaluation of a common preoperative carbohydrate beverage. Nutrition. 2011;27(9):897-903.
CrossRef - Dock-Nascimento D. B., de Aguilar-Nascimento J. E., Magalhaes Faria M. S., Caporossi C., Slhessarenko N., Waitzberg D.L. Evaluation of the effects of a preoperative 2-hour fast with maltodextrine and glutamine on insulin resistance, acute-phase response, nitrogen balance, and serum glutathione after laparoscopic cholecystectomy: a controlled randomized trial. JPEN J Parenter Enteral Nutr. 2012;36(1):43-52.
CrossRef - Braga M., Bissolati M., Rocchetti S., Beneduce A., Pecorelli N., Di Carlo V. Oral preoperative antioxidants in pancreatic surgery: a double-blind, randomized, clinical trial. Nutrition. 2012;28(2):160-164.
CrossRef - Marquini G. V., Pinheiro F. E. D. S., Vieira A. U. D. C., et al. Preoperative Fasting Abbreviation and its Effects on Postoperative Nausea and Vomiting Incidence in Gynecological Surgery Patients. Efeitos da abreviação de jejum préoperatório na incidência de náuseas e vômitos em pacientes cirúrgico-ginecológicas. Rev Bras Ginecol Obstet. 2020;42(8):468-475.
CrossRef - Sutanto L., Bardosono S., Aziz, M. F. et al. PP003-mon oral nutritional supplements before surgery reduced the post-operative metabolic stress factors in cesarean section. Clin. Nutr. 2013; 32:S124.
CrossRef - Yi HC, Ibrahim Z, Abu Zaid Z, et al. Impact of Enhanced Recovery after Surgery with Preoperative Whey Protein-Infused Carbohydrate Loading and Postoperative Early Oral Feeding among Surgical Gynecologic Cancer Patients: An Open-Labelled Randomized Controlled Trial. Nutrients. 2020;12(1):264. Published 2020 Jan 20.
CrossRef - PRISMA. Available online: http://www.prisma-statement.org/Protocols/ (accessed on 19 March 2020).
- Wendling A. L., Byun S. Y., Koenig M., Vasilopoulos T. Impact of oral carbohydrate consumption prior to cesarean delivery on preoperative well-being: a randomized interventional study. Arch Gynecol Obstet. 2020;301(1):179-187.
CrossRef - Yang C., Cheng Y., Liu S., Huang S., Yu X. Effect of Preoperative Oral Carbohydrate Loading on Body Temperature During Combined Spinal-Epidural Anesthesia for Elective Cesarean Delivery. Anesth Analg. 2021;133(3):731-738.
CrossRef - Clark A., Litchfield K., Hannah S., et al. Pre-operative carbohydrate loading prior to elective caesarean delivery: a randomised controlled trial. Int J Obstet Anesth. 2021;45:21-27.
CrossRef - He Y., Liu C., Han Y., Huang Y., Zhou J., Xie Q. The impact of oral carbohydrate-rich supplement taken two hours before caesarean delivery on maternal and neonatal perioperative outcomes — a randomized clinical trial. BMC Pregnancy Childbirth. 2021;21(1):682. Published 2021 Oct 7.
CrossRef - Liu N., Jin Y., Wang X., Xiang Z., Zhang L., Feng S. Safety and feasibility of oral carbohydrate consumption before cesarean delivery on patients with gestational diabetes mellitus: A parallel, randomized controlled trial. J Obstet Gynaecol Res. 2021;47(4):1272-1280.
CrossRef - Fard R. K., Tabassi Z., Qorbani M., Hosseini S. The Effect of Preoperative Oral Carbohydrate on Breastfeeding After Cesarean Section: A Double-Blind, Randomized Controlled Clinical Trial. J Diet Suppl. 2018;15(4):445-451.
CrossRef - Shi Y., Dong B., Dong Q., Zhao Z., Yu Y. Effect of Preoperative Oral Carbohydrate Administration on Patients Undergoing Cesarean Section with Epidural Anesthesia: A Pilot Study. J Perianesth Nurs. 2021;36(1):30-35.
- Ricci C., Ingaldi C., Alberici L., et al. Preoperative carbohydrate loading before elective abdominal surgery: A systematic review and network meta-analysis of phase II/III randomized controlled trials. Clin Nutr. 2022;41(2):313-320.
CrossRef - Kotfis K., Jamioł-Milc D., Skonieczna-Żydecka K., Folwarski M., Stachowska E. The Effect of Preoperative Carbohydrate Loading on Clinical and Biochemical Outcomes after Cardiac Surgery: A Systematic Review and Meta-Analysis of Randomized Trials. Nutrients. 2020;12(10):3105. Published 2020 Oct 12.
CrossRef - Xu, C.; Hua, K. Applied Obstetrics and Gynecology; Beijing: People’s Medical Publishing House;2018.
- Ge L. N., Wang L., Wang F. Effectiveness and Safety of Preoperative Oral Carbohydrates in Enhanced Recovery after Surgery Protocols for Patients with Diabetes Mellitus: A Systematic Review. Biomed Res Int. 2020;2020:5623596. Published 2020 Feb 18.
CrossRef - Queensland Clinical Guidelines. Guideline: New born hypo-glycaemia [EB/OL].
- Li J. Endocrinology in Gynecology and Obstetrics; People’s Military Medical Press: Beijing, 2010.
- Jones J.L. Breast. In Underwood’s Pathology: A Clinical Approach, Cross, S., Ed. Elsevier: Edinburgh, 2019; pp. 416–437.
- Alex A., Bhandary E., McGuire K. P. Anatomy and Physiology of the Breast during Pregnancy and Lactation. Adv Exp Med Biol. 2020;1252:3-7.
CrossRef - Sevelsted A., Stokholm J., Bønnelykke K., Bisgaard H. Cesarean section and chronic immune disorders. Pediatrics. 2015;135(1):e92-e98.
CrossRef - MacArthur A. C, McBride M. L., Spinelli J. J., Tamaro S., Gallagher R.P., Theriault G.P. Risk of childhood leukemia associated with vaccination, infection, and medication use in childhood: the Cross-Canada Childhood Leukemia Study. Am J Epidemiol. 2008;167(5):598-606.
CrossRef - Prescott S. L, Macaubas C., Smallacombe T., Holt B.J., Sly P.D., Holt P.G. Development of allergenspecific T-cell memory in atopic and normal children. Lancet. 1999;353(9148):196-200.
CrossRef - Følsgaard N. V, Chawes B. L., Rasmussen M. A., et al. Neonatal cytokine profile in the airway mucosal lining fluid is skewed by maternal atopy. Am J Respir Crit Care Med. 2012;185(3):275-280.
CrossRef - Chang J. S., Zhou M., Buffler P. A., Chokkalingam A.P., Metayer C., Wiemels J. Profound deficit of IL10 at birth in children who develop childhood acute lymphoblastic leukemia. Cancer Epidemiol Biomarkers Prev. 2011;20(8):1736-1740.
CrossRef
Accepted on: 29 Jul 2023
Second Review by: Amany A Salama
Final Approval by: Dr Aly al shiekha





Web of Science Coverage
Emerging Sources Citation Index (ESCI)
2024 Journal Impact Factor: 1.1
Scopus Journal Metrics
CiteScore 2025: 2.6
CiteScore Details
Sustainable Nutrition: Food Systems, Nutrient Retention, and Public Health Impact
![]()
This journal is a member of, and subscribes to the principles of, the Committee on Publication Ethics (COPE)








