Age-Related Macular Degeneration Risks Linked with Indian Dietary Fat Consumption Patterns
 , Renu Thakur2* and Shaikh Mohd Danish2
, Renu Thakur2* and Shaikh Mohd Danish2 1Lotus College of Optometry, Mumbai, Maharashtra, India.
2Chitkara School of Health Sciences, Chitkara University, Punjab, India.
Corresponding Author E-mail: renu.thakur@chitkara.edu.in
DOI : http://dx.doi.org/10.12944/CRNFSJ.11.2.23
Download this article as:
![]()
Background: The prevalence of age-related macular degeneration in India is lower than in America and Europe at 0.61 to 1.9%. Studies have shown that dietary patterns and consumption of certain food groups can influence the prevalence of age-related macular degeneration (ARMD) in a given population. Aim: This study's goal was to evaluate the impact of dietary fat and food consumption patterns in Indians with ARMD and compare it to age-matched healthy individuals. Methodology: 90 patients from a Mumbai ophthalmology outpatient clinic who were above 50 years were recruited to participate in the research. The participants were divided into groups of those with and without ARMD based on the fundus assessment. For each of the meals, a food frequency questionnaire was utilized to record the common foods that all of the individuals ate. They were asked to remember the foods they had just ingested. Based on consumption patterns, some were grouped as vegetarians who had only plant-based foods and others as non-vegetarians who consumed meat, fish and eggs. Using a conversion table created for Indian meals, the intake of monounsaturated fatty acids (MUFA) and polyunsaturated fatty acids was quantified. The information was then analyzed between those with and without ARMD. Results: 45/90 people were in the control group, and among the 45 cases. The amount of MUFA consumed was 44.29+26.00 and 40.53+17.18 and PUFA consumed was 35.57+26.34 and 43.61+ 27.27 by the cases and controls discretely. With regard to dietary fats, there was no statistically significant difference between them p=0.05. Further, the food types consumption was analysed and it showed that 13% of the cases were vegetarians whereas 47% of the controls were vegetarians. 12% of the servings consumed in the cases had meat whereas only 3% of the servings contained meat among the controls. The control group consumed 1.7% servings of fish whereas the cases consumed 0.59%. Conclusion: The present study results show that Indians consume foods rich in PUFA which could lower the risk of ARMD. The results further indicate that subjects who consumed more vegetarian foods and were lower on meat were at a reduced risk to develop ARMD.
KEYWORDS:Age-Related Macular Degeneration (ARMD); Monounsaturated Fatty Acids (MUFA); Polyunsaturated Fatty Acids (PUFA)
Introduction
Age-related macular degeneration is presently the second leading cause of blindness in the world, behind cataracts and untreated refractive errors1. The National Eye Institute recommends quitting smoking, engaging in regular exercise, maintaining healthy blood pressure, and controlling cholesterol levels to lower the risk factors that may lead to age-related macular degeneration (ARMD). Additionally, it has been suggested to keep a balanced diet that includes fish and leafy greens2. In India, ARMD prevalence has been estimated as 0.61 to 1.9%.3. The worldwide prevalence research revealed that Asians, notably the Indian population, had a lower prevalence of ARMD than did Europeans and Americans4. Chui CJ et. al. studied the American food consumption patterns and risks for ARMD. They identified two largely followed dietary patterns, one was Western with more red meat, dairy products, and processed foods and the second was the Oriental pattern which had more plant-based foods and sea foods. The study concluded that Western dietary consumption patterns had higher risks for developing ARMD.5 The Melbourne Collaborative cohort study group reported that the people who consumed red meat and processed foods were at higher risk to develop ARMD as compared to those who consumed plant-based foods.6 Preventive interventions are an excellent choice since there are currently few available treatments for ARMD that has extensive vision loss. Although some investigations disputed the results of the AREDS research, they did show the importance of supplements in the treatment of ARMD7. Consumption of certain food groups has demonstrated the relative risks to the development of ARMD and some food patterns have shown reduced risks.5,6 An analysis of Indian dietary habits revealed that the country’s cuisine is full of polyunsaturated fats, which have been linked to a decreased risk of developing ARMD8. Although located in Asia, Indian food and dietary patterns is quite different from the rest of the continent. The aim of this case-control study was to understand Indian dietary patterns, particularly the consumption of dietary fats and their association in patients with and without ARMD. The objective was to also identify dietary patterns that had lower risk as a preventive strategy and modify the risk to develop ARMD.
Material And Methodology
Study population
Patients from 2 tertiary care eye hospitals were invited to participate in the study after, receiving clearance from the local ethics council for the research. From historical records of the retina departments, participants were selected for this cross-sectional research. All subjects gave their informed consent before being included in the research. It is a case-control study and the sample size was determined as 90, using the prevalence rate of ARMD. 45 participants with age-related macular degeneration were included in the research. All patients who were 50 years of age or older were included. A reference group of 45 participants who were 50 years of age or older and did not show any indications or symptoms of ARMD in either of their two eyes was also included in the research. All participants who had previously had age-related macular degeneration therapy or any kind of retinal surgery were excluded from the study. Active uveitis, vitreoretinal disease, posterior subcapsular cataract, and other eye infections were eliminated from the list of other ocular disorders. Glaucoma was diagnosed with a 0.7 C.D (Cup-Disc) ratio and a spherical equivalent refractive error of 6.00D was also disregarded. Those with a history of diabetes were excluded from the research.
Grading of Age-Related Macular Degeneration
Each subject had testing for their best corrected visual acuity (BCVA), current refraction, intraocular pressure (IOP), slit lamp biomicroscopy, and dilated fundus examination. A Topcon TRC-50DX9 or a Zeiss Zeiss FF-45010 Plus camera from Carl Zeiss Meditec in Dublin, California was used for the non-stereoscopic, colour fundus photography of the seven fields on the recruited individuals. The obtained colour fundus picture served as the basis for the diagnosis and staging of ARMD. ARMD was diagnosed using definition11 from the age-related eye disease study 2 (AREDS2) classification. Study participants also underwent retinal scans using spectral-domain optical coherence tomography (Topcon 3D OCT-1 Maestro)12.
Assessment of Dietary patterns
In order to evaluate dietary fat intake, a food frequency questionnaire was also administered to each patient at the same appointment. It featured an open-ended part for every mealtime in addition to a food history questionnaire (FFQ) with specific questions about frequency and quantity size. A list of 100 frequently consumed foods for various meals like breakfast, lunch, and dinner was made and then later edited to add items that were on the FFQ recalls list. Portion sizes were calculated using the number of servings and units calculated. An excel sheet application with formulas and units was developed. The nutrition data tools was updated and built from a collection of existing foreign databases that include information on Indian foods and recipes, and using a validated tool My Food Data13. The information was gathered from each participant and was then keyed into this tool. Portion size and frequency of intake were then calculated using this information. Based on the quantity of food ingested, this application provides the precise value of monounsaturated and polyunsaturated fatty acids. The MUFA and PUFA levels were computed using the individuals’ portion sizes as a basis. The data were further categorized for individuals who were vegetarians or solely consumed plant-based diets and those who ingested red meat, fish, and eggs as non-vegetarians since India has a substantial population of vegetarians (almost 9%). The participants were subsequently divided into vegetarians and non-vegetarians based on their eating habits.
Statistical Analysis
SPSS statistics software version 25 was used for data analysis. Shapiro-Wilk tests were used to check the data for normal distribution. Paired T test was applied to find the significance. The data was also analysed to understand the change in fat intake to the grades of ARMD. Qualitative analysis was done to understand foods that were consumed among cases and controls and the dietary intake influence of ARMD.
Results
90 subjects consented to participate in all, 45 of whom were controls. 45 were diagnosed to have ARMD were cases. 25 of whom had early ARMD, 12 of who had intermediate ARMD, and 8 of whom had geographic atrophy ARMD. Tests for normality showed that the data were normally distributed. The mean age among the cases and control groups were 58.2+5.2 years and 59.1+5.4 years respectively, and the difference between the two groups was not statistically significant. Therefore, the groups were age-matched. Similarly, they were also gender-matched 31/45 males in the cases and 32/45 males among the controls and the rest were females. Overall study group had 70% males. 26% of the study population were vegetarians and the rest were non-vegetarians.
Food types consumption was analyzed and it showed that 13% of the cases were vegetarians whereas 47% of the controls were vegetarians. 12% of the servings consumed in the cases had red meat whereas only 3% of the servings contained meat among the controls. The control group consumed 1.7% servings of fish whereas the cases consumed 0.59%.
When the severity of ARMD was analysed using One-Way ANOVA, it showed that those who consumed non-vegetarian foods were at a higher risk for developing ARMD and the difference was statistically significant with a P = 0.001 as shown in figure 1.
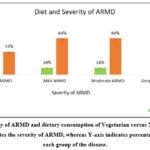 |
Figure 1: Severity of ARMD and dietary consumption of Vegetarian versus Non-Vegetarians, the x axis indicates the severity of ARMD, whereas Y-axis indicates percentage of subjects in each group of the disease. |
Despite the fact that the intake of MUFA, PUFA, and total fat in the control and ARMD patients did not vary statistically significantly from one another (P = 0.134). The mean value of dietary fatty acids, PUFA and total fats were higher in the age-matched control group as compared to ARMD cases as shown in (Table 1).
Table 1: Table showing mean values with a standard deviation of cases and control, separated by MUFA, PUFA and Total Group
|
|
Retinal Condition |
N |
Mean |
Std. Deviation |
Std. Error Mean |
Sig |
t |
df |
|
MUFA |
ARMD |
45 |
44.9274 |
26.00285 |
3.87628 |
.71 |
.944 |
88 |
|
Normal |
45 |
40.5390 |
17.18874 |
2.56235 |
|
.944 |
76.288 |
|
|
PUFA |
ARMD |
45 |
35.5786 |
26.34337 |
3.92704 |
.61 |
-1.422 |
88 |
|
Normal |
45 |
43.6179 |
27.27398 |
4.06577 |
|
-1.422 |
87.894 |
Independent T test also found no statistically significant difference in MUFA and PUFA between control and ARMD subjects. i.e., p>0.05
The distribution of grades of ARMD has been shown in the figure below where early ARMD was seen in 56%, intermediate ARMD in (24%), and geographic atrophy was diagnosed in 20% of participants. Table 2 shows the mean, standard deviation and P value of dietary fats.
Table 2: Characteristics of participants according to the stages of ARMD
|
|
Early |
Intermediate |
Geographic Atrophy |
P- value |
|
g/day |
N 56% |
N 24% |
N 20% |
– |
|
PUFA |
36.7 ± 5.2 |
37.0 ± 7.0 |
29.7 ± 11.2 |
0.48 |
|
MUFA |
44.2 ± 3.9 |
44.7 ± 6.6 |
47.2 ± 16.0 |
0.80 |
|
TOTAL |
69.1 ± 6.1 |
74.2 ± 11.4 |
71.9 ± 26.3 |
0.50 |
The mean value of dietary fats (MUFA, PUFA, and Total) was compared with the severity of ARMD. The difference was not statistically significant, the PUFA value consumed among the normal was to 43.6 g/day and for those with geographic atrophy was 29.7 g/day as shown in figure 2.
Relative risk was calculated for MUFA and PUFA consumptions per day to geographic ARMD and the normal groups and a value of <1.00 ( 0.752) was obtained, indicating that higher PUFA consumption was a protective factor. Similarly when relative risk score was calculated for those who were vegetarians or consumed plant based foods and those who had meat, consumption of meat showed a relative risk score of 2.8 indicating that consumption of non-vegetarian foods was a higher risk to developing ARMD.
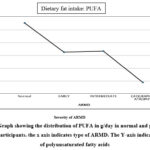 |
Figure 2: Graph showing the distribution of PUFA in g/day in normal and geographic atrophy participants. the x axis indicates type of ARMD. The Y-axis indicates Mean of polyunsaturated fatty acids |
Discussion
The study’s strength is the age-matched cases and controls, since there was no statistically significant difference between the groups (p>0.05). In a study by Roh M et. al., 14 , it was reported that the control group’s mean age was greater (70±37) than in the patients group(69±0.36). Reynolds R et.al., the subsequent investigation also found that the patients’ mean age was higher (63.2±7.9) than that of the controls (60.3±6.7)15. In the current investigation, there was a gender imbalance, with a larger percentage of males in the control group and patients. Reynolds R et.al., found that 61% of controls and 55% of cases were men. Women made up 39% of the control group14 and 45% of the cases. However, a study by Roh M et.al., discovered that cases made up 36.3% of the cases and 36.1% of the male population in the control group. According to the current research, the cases and control groups, respectively, had 68% and 71% men.
In the present study there was no statistically significant difference between the groups for intake of dietary fats (i.e., MUFA and PUFA). In a study in 2016, a total of 483 participants, 386 of whom had ARMD, and 97 controls were included in research by Roh M et.al.14. They claimed that increasing PUFA and MUFA consumption had a negative impact on ARMD (OR, 0.25; P for trend = 0.006 and 0.24; P for trend 0.001, respectively). This is supported by the present research, which found that the control group consumed more PUFA than the cases did. Greater quintiles of trans fat were shown to be both positively and negatively correlated with ARMD, according to a subgroup analysis of the aforementioned research15 (OR, 0.2; P for trend = 0.0013; OR, 0.17; P = 0.0001; OR, 2.26; P for trend = 0.02). However, the present analysis showed a similar tendency of a negative association of PUFA when compared to controls and throughout the phases of ARMD. The demographic group with geographic ARMD ate the fewest PUFA. Increased trans-fat consumption was linked to a greater incidence, presence, and development of ARMD, according to studies 16–17.
Most PUFA are composed of omega-3 FA and omega-6 FA. The control group in our research ingested more PUFA than the ARMD group. Participants in the control group’s mean PUFA value was 43.6, whereas those who had geographic atrophy had a mean value of 29.7. This illustrated the link between dietary supplementation with omega-3 fatty acids and the prevention of ARMD. Therefore, omega-3 supplements are advised since they reduce the risk of ARMD. Studies have shown that omega-3 fatty acids are associated with a decreased incidence of ARMD because of their anti-inflammatory properties 18-19. However, the AREDS2 trial indicated that supplementing with omega-3 fatty acids did not reduce episodes of advanced ARMD 20-21. The NAT2 study 22-23. discovered that individuals with consistently high blood levels of docosahexaenoic acid/eicosapentaenoic acid were substantially protected against the development of ARMD compared to those with consistently low levels, indicating that the quantity of omega-3 FA in the AREDS supplement may not be enough. Eating nuts, which are the major source of omega-6 fatty acids, may help lower the risk of ARMD development, claim Seddon et.al.,14. According to a 2009 study by Chong et.al., eating red meat increases your chance of developing ARMD24 The current research supports the conclusions since the cases ingested three times as much red meat and poultry as the control group did. Similar to this, a 2018 systematic analysis of the effect of food on ARMD by Chapman et.al., found that eating more vegetables and fish decreased the chance of developing ARMD25. In the current research, the controls had three times as many vegetarians as the controls did and ate 2.8 times more quantity of fish than the cases did. Compared to age-matched American and European populations, ARMD prevalence is lower among the Indian population.26-27. Additionally, it has been noted that Indian eating habits indicate a larger consumption of plant-based meals.8,28. According to research by Jaacks et.al., on vegetarianism and risk factors for cardiometabolic illness, the risk was reduced in those who followed a vegetarian diet 28. The present research results demonstrate a favourable correlation between non-vegetarian food intake and ARMD severity. On the chronic diseases.29 There is a need for additional research on obesity in India’s rural as well as urban households30,31.
Conclusion
Advancing age and increased life span are leading causes of ARMD, however, nutrients and nutritional supplements have been demonstrated to reduce risk factors associated with severity and vision impairment associated with ARMD. The present study results show that Indians consume foods rich in PUFA which could lower the risk. The results also revealed that vegetarians and those who consumed less red meat and more fish in their regular dietary intake were at a reduced risk. More research in the area of vegetarian food consumption and age-related disorders could be looked into.
Acknowledgment
We like to acknowledge Lotus eye hospital and Aastha Eye Hospital, management and staff for their cooperation’s.
Conflict of Interest
There is no conflict of interest
Funding Sources
The present study was not funded by any agency
References
- Bourne R.R.A, Flaxaman S.R, Braithwaite T, Cicinelli M.V, Das A. J. Vision loss expert group. Magnitude, temporal trends, and projections of the global prevalence of blindness and distance and near vision impairment: a systematic review and meta-analysis. Lancet Glob Health. 2017; 9: 88-97.
- Mares-Perlman J.A, Brady WE, Klein R, VandenLangenberg G.M, Klein B.E.K, Palta M. Dietary Fat and Age-Related Maculopathy. Arch Ophthalmol. 1995;113(6):743–748.
CrossRef - Nirmalan P.K, Katz J, Robin AL. Prevalence of vitreoretinal disorders in a rural population of southern India: the Aravind Comprehensive Eye Study. Arch Ophthalmol. 2004;122(4):581–586. 65.
CrossRef - Wong W.L, Su X, Li X, Cheung C.M.G, Klein R, Cheng C.Y, Wong T.Y, Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: a systematic review and meta-analysis, The Lancet Global. 2014; 2(2): 106-116.
CrossRef - Chiu CJ, Chang ML, Zhang FF, Li T, Gensler G, Schleicher M, Taylor A. The relationship of major American dietary patterns to age-related macular degeneration. Am J Ophthalmol. 2014 Jul;158(1):118-127.
CrossRef - Amirul Islam FM, Chong EW, Hodge AM, Guymer RH, Aung KZ, Makeyeva GA, Baird PN, Hopper JL, English DR, Giles GG, Robman LD. Dietary patterns and their associations with age-related macular degeneration: the Melbourne collaborative cohort study. Ophthalmology. 2014 Jul;121(7):1428-1434.
CrossRef - West S, Vitale S, Hallfrisch J. Are Antioxidants or Supplements Protective for Age-Related Macular Degeneration? Arch Ophthalmol. 1994;112(2):222–227.
CrossRef - Mani I, Kurpad A.V. Fats & fatty acids in Indian diets: Time for serious introspection. Indian J Med Res. 2016;144(4):507-514
- Tsikata E, Ines La, Gil J, Marque M, Brown K, Mesquita T, Melo P, Cachulo M.D.L, Ivana K. K, Vavvas D, Joaquim N. M, Miller J.B, Silva R, Miller J W, Teresa C. C, and Husainl D. Automated Brightness and Contrast Adjustment of Color Fundus Photographs for the Grading of Age-Related Macular Degeneration. TVST. 2017: 6(2): 1-13
CrossRef - Neubauer A.S, Rothschuh A, Ulbig M.W and Blum M. Digital fundus image grading with the non-mydriatic VisucamPRO NM versus the FF450plus camera in diabetic retinopathy. Acta Ophthalmol. 2008; 86: 177–182.
CrossRef - Domalpally A, Danis RP, Chew EY. Methods and reproducibility of grading optimized digital color fundus photographs in AREDS2 methods and grading procedures for AREDS2 image. Invest Ophthalmic Vis Sci.2013; 54, 4548-4554.
CrossRef - Chaglasian M, Fingeret M, Davey P.G, Huang W.C, Leung D, Edmund N, Charles A, R. The development of a reference database with the Topcon 3D OCT-1 Maestro. Clinical Ophthalmology. 2018:12: 849-857.
CrossRef - Paul House, Daisy Whitbread, Namibia Torres, Belle lee. My Food Data. USDA Food Data Central.2008.
- Roh M, Shin H.J, Hussain D. Higher Intake of Polyunsaturated Fatty Acid and Monounsaturated Fatty Acid is Inversely Associated with AMD. Invest Ophthalmic Vis Sci. 2016; 54: 318-322.
- Reynolds R, Rosner B, Seddon JM. Dietary omega-3 fatty acids, other fat intake, genetic susceptibility, and progression to incident geographic atrophy. Ophthalmology.2013; 29, 71-75.
CrossRef - Chong EW-T, Robman LD, Simpson J.A. Fat consumption and its association with age-related macular degeneration. Arch Ophthalmol.2009;127: 674-680.
CrossRef - Chua B, Flood V, Rochtchina E, Wang JJ, Smith W, Mitchell P. Dietary fatty acids and the 5-year incidence of age-related maculopathy. Arch Ophthalmol. 2006;124: 981-986.
CrossRef - SanGiovanni J.P, Chew E.Y, Argon E. The relationship of dietary omega-3 long chain polyunsaturated fatty acid intake with incident age-related macular degeneration: AREDS report no. 23. Arch Ophthalmology.2008;126:1274-1279.
CrossRef - Mukherjee P.K, Marcheselli V.L, Barreiro S, Hu J, Bok D, Bazan NG. Neurotrophins enhance retinal pigment epithelial cell survival through neuroprotection D1 signaling. Proc Natl Acad Sci USA. 2007;104, 13152-13157.
CrossRef - Mukherjee P.K, Marcheselli V.L, de Rivero Vaccari J.C, Gordon W.C, Jackson F.E, Banzan N.G. Photoreceptor outer segment phagocytes attenuates oxidative stree-induced apoptosis with concomitant neuroprotectin D1 synthesis. Proc Natl Acad Sci USA. 2007;104:13158-13163.
CrossRef - Merle B.M, Richard F, Benlian P, Puche N, Delcourt C, Souied EH. CFH Y402H and ARMS2 A69S polymorphisms and oral supplementation with docosahexaenoic acid in neovascular age-related macular degeneration participants: the NAT2 Study. PIoS One. 2015; 49:13-16.
CrossRef - Souied E.H, Delcourt C, Querques G. Oral docosahexaenoic acid in the prevention of exudative age-related macular degeneration: The Nutritional AMD Treatment 2 study. Ophthalmology. 2013;120:1619-1631.
CrossRef - Lawrenson J.G, Evans J.R, and Cochrane Eyes and Vision Group. Omega 3 fatty acids for preventing or slowing the progression of age-related macular degeneration. City University London, Division of Optometry and Visual Science, Northampton Square, London, EC1V 0HB. 2017
- Chong, E. W. T., Simpson, J. A., Robman, L. D., Hodge, A. M., Aung, K. Z., English, D. R., Guymer, R. H. Red meat and chicken consumption and its association with age-related macular degeneration. American journal of epidemiology. 2009;169(7):867-876.
CrossRef - Chapman, N. A., Jacobs, R. J., & Braakhuis, A. J. Role of diet and food intake in age‐related macular degeneration: a systematic review. Clinical & experimental ophthalmology. 2019; 47(1):106-127.
CrossRef - Kawasaki R, Yasuda M, Song SJ, Chen S-J, Jonas JB, Wang JJ. The Prevalence of Age-Related Macular Degeneration in Asians: A Systematic Review and Meta-Analysis. Ophthalmology. 2010;117(5):921–7.
CrossRef - Gupta SK, Murthy GV, Morrison N. Prevalence of early and late age-related macular degeneration in a rural population in northern India: the INDEYE feasibility study. Invest Ophthalmol Vis Sci. 2007;48(3):1007–1011.
CrossRef - Jaacks LM, Kapoor D, Singh K, et al. Vegetarianism and cardiometabolic disease risk factors: Differences between South Asian and US adults. Nutrition. 2016;32(9):975-984.
CrossRef - Boeing, Heiner. Critical review: vegetables and fruit in the prevention of chronic diseases. European journal of nutrition. 2012; 51(6):637-663.
CrossRef - Sims A, Pligt P, John P, Kaushal J, Kaur G, McKay F. Food Insecurity and Dietary Intake among Rural Indian Women: An Exploratory Study. Int. J. Environ. Res. Public Health 2021, 18, 4851.
CrossRef - McKay F, John P, Sims A, Kaur G, Kaushal J. Documenting the Food Insecurity Experiences and Nutritional Status of Women in India: Study Protocol. Int. J. Environ. Res. Public Health 2020, 17, 3769
CrossRef
Accepted on: 29 May 2023
Second Review by: Prabin Shrestha
Final Approval by: Dr. Neha Sanwalka





Web of Science Coverage
Emerging Sources Citation Index (ESCI)
2024 Journal Impact Factor: 1.1
Scopus Journal Metrics
CiteScore 2025: 2.6
CiteScore Details
Sustainable Nutrition: Food Systems, Nutrient Retention, and Public Health Impact
![]()
This journal is a member of, and subscribes to the principles of, the Committee on Publication Ethics (COPE)








