Vitamin D on COVID-19 Patients During The Pandemic, 2022. A systematic Review and Meta-Analysis
 , Asmaa Ahmed Nawar1, Esraa Elsayed2, Ramadan Abdelmoez Farahat5, Ayah Abdulgadir6, Mostafa Abdullah Alsharabasy1, Israa Mohamed Elshahawy7 and Samar A. Amer2, , 4*
, Asmaa Ahmed Nawar1, Esraa Elsayed2, Ramadan Abdelmoez Farahat5, Ayah Abdulgadir6, Mostafa Abdullah Alsharabasy1, Israa Mohamed Elshahawy7 and Samar A. Amer2, , 4* 1Faculty of Human Medicine, Zagazig University, Zagazig City, Sharkia, Egypt.
2Faculty of Medicine, Kafrelsheikh University, Kafrelsheikh, Egypt.
3Faculty of Medicine, University of Khartoum, Sudan.
4Faculty of Pharmacy, Zagazig University, Zagazig City, Sharkia, Egypt.
5Department of Public Health and Community Medicine, Faculty of Medicine, Zagazig University, Zagazig City, Sharkia, Egypt.
6Membership at the Royal Colleague of General Practitioners[INT], London, United Kingdom.
7Department of Mental Health Primary Care, Nova University, Lisbon
Corresponding Author E-mail: dr_samar11@yahoo.com
DOI : http://dx.doi.org/10.12944/CRNFSJ.11.1.3
Download this article as:
![]()
Numerous connections between the level of vitamin D (Vit-D) and the novel coronavirus disease -19 (COVID-19) have surfaced during the pandemic. So, we conducted this systematic review and meta-analysis to explore the effect of Vit-D deficiency and its supplementation on the clinical outcomes of COVID-19 patients. We looked for relevant articles in Cochrane Library, Scopus, Web Science, PubMed, and EBSCO up until the end of 2022. The Open Meta Analyst software was used to analyze the extracted data. We classified them into two main categories based on their objectives. First, the studies that evaluated the effects of Vit-D deficiency in patients, and lastly, the studies that evaluated Vit-D as a supplement, both on mortality rate, hospitalization duration, ICU admission rate, and mechanical ventilation rate. A total of 8001 COVID-19 patients from 42 studies were included. A high serum Vit-D concentration compared to those with lower levels was associated with a significantly lower mortality rate (RR = 1.5, 95% CI = 1.11: 2.02, p = 0.01). According to the estimated effect of 18 studies, those who took Vit-D supplements had a significantly lower mortality rate, hospitalization duration, ICU admission rate, and mechanical ventilation rate than those who did not. The group receiving Vit-D doses between 50 000 to 100 000 IU had a significantly better clinical outcome compared to lower and higher doses. COVID-19 patients with normal Vit-D levels had significantly lower death rates than those with hypovitaminosis. Vit-D supplements in COVID-19 significantly improved clinical outcomes. Vit-D supplementation between 50 000 to 100 000 IU, in patients with COVID-19 significantly outperformed other doses in terms of mortality.
KEYWORDS:Clinical Outcome; Efficacy; Vitamin D deficiency; Vitamin D supplements; SARS-CoV-2 virus
Introduction
The Coronavirus Disease 2019 (COVID-19) pandemic is a serious global threat resulting from the spread of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. SARS-CoV-2 had affected nearly 306 million cases and resulted in more than 5.4 million deaths as of early January 2022 1. The severity of the SARS-CoV-2 infection depends on the development of acute respiratory distress syndrome (ARDS), pneumonia, thrombosis, and vital organ failure.These complications arise from initiating a cytokine storm that involves an aggressive inflammatory response causing multi-system damage 2. Individuals with risk factors, including advanced age, hypertension, diabetes mellitus, cardiovascular diseases, and obesity, frequently experience more severe illness following COVID-19 infection 3–6. A lack of Vitamin D (Vit-D) has also been considered a possible risk factor for bad outcomes7,8.
Vitamin D is a fat-soluble vitamin obtained through diet, sunlight, and dietary supplements 9. Calcitriol (1,25-dihydroxy vitamin D3) is the active form of Vit-D that exhibits a potent immunomodulatory effect by enhancing innate and acquired immune responses. Vit-D improves innate immunity by activating antimicrobial peptides, including defensins and cathelicidin. Calcitriol also inhibits the expression of pro-inflammatory mediators and increases anti-inflammatory mediator production from macrophages10,11. Regarding acquired immunity, calcitriol suppresses T helper lymphocyte type 1, which produces inflammatory cytokines10. These anti-inflammatory effects of Vit-D contribute to alleviating the COVID-19 cytokine storm. Vit-D also increases the levels of T-regulatory lymphocytes, which protect against inflammation and viral infections 12.
In addition to the role of Vit-D in immunity, it exhibits anti-thrombotic actions that can interfere with the microvascular thrombosis caused by SARS-CoV-2 12,13. Moreover, Vit-D increases the genetic expression of enzymes related to antioxidant production, mainly glutathione12,14. This antioxidant effect protects the cells from the oxidative stress caused by the infection and lowers patients’ viral loads. All these beneficial actions promise that Vit-D supplementation should improve the outcomes of COVID-19 patients.
During the pandemic, numerous observational studies assessed the association between Vit-D insufficiency and patients’ prognosis. Other interventional studies aim to determine the effect of Vit-D supplementation on disease severity. For this reason, we hypothesize that Vit-D deficiency may be a risk factor in patients with COVID 19 and its supplementation would improve their clinical outcomes. Therefore, we conducted this systematic review and meta-analysis to explore the effect of vitamin D deficiency and its supplementation on the clinical outcomes of COVID-19 patients.
Methods
We conducted this meta-analysis and reported it following Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement guidelines and followed the criteria used in the Cochrane Handbook of Systematic Reviews and Meta-analyses 16.
Eligibility criteria
We came up with a PICOs strategy, which stands for population, intervention, comparison, outcome, and study design. We defined the PICOs as follows: P = COVID-19 patients; I = Vitamin D deficiency or supplementation; C = comparator or control group; O = mortality rate as the primary outcome and ICU admission or hospitalization duration as secondary outcomes; S: randomized controlled trials; cross-sectional, prospective, and retrospective cohort studies.
Eligibility requirements
Both observational (prospective or retrospective, cohort or case-control design) and randomized controlled trials (parallel or cross-over), blinded (single-blind, double-blind, or open-label) studies. 2) Studies including COVID-19 individuals. 3) At least one of the clinical outcomes of COVID-19 patients (mortality, ICU admission, ventilation, or hospitalization duration). 4) The clinical outcomes should be presented as the number of “events” in patients with COVID-19 who received Vit-D treatment compared to those who did not get Vit-D.
Exclusion criteria for clinical case series, review papers, book chapters, study procedures, critiques, editorials, comments, letters to the editor, studies without peer review, and finally, incompleteness in data.
Search strategy
We conducted a basic search independently through a systematic literature search across five different databases: PubMed, Cochrane Library, Scopus, Web of Science, and EBSCO, for relevant studies from 2019 up to the end of 2022. There were no limitations related to language or specific durations. The following keywords are interposed with “COVID-19” or “SARS-CoV-2” and “Vitamin D” (deficiency or supplementation). Searching relevant review references and retrieved documents for potentially qualifying articles. The corresponding authors of potentially eligible papers were contacted whenever possible for missing data.
Selection process
The study selection process consisted of two steps. First, two review authors (R.A.F. and E.E.) independently screened the titles and abstracts (TAs) of the retrieved records based on the PICOS strategy to exclude duplicate studies and those that did not meet the qualifying criteria. Secondly, the same reviewers assessed the full text of the selected ones. Any disagreement between the reviewers was resolved by discussion or with the senior author (M.M.A.).
The extracted data
Two authors (A.A.N. and A.A.) independently extracted required data from the included studies using a well-organized Excel sheet. The extracted data included: 1) baseline characteristics data, including age, gender, sample size, and health status. 2) The study characteristics, including setting and study design; 3) The reported serum vitamin D levels were classified into three groups based on a normal range (10-30 ng/mL): Group A (< 10 ng/mL, severe deficiency), Group B (< 20 ng/mL) and Group C (> 30 ng/mL, normal); 4) Vit-D supplementation-related data, including the dose and follow up duration, the formulation and method of Vit-D administration, the number of patients who received Vit-D, the number of COVID-19 patients who received Vit-D; and 5) The reported clinical outcome compared to those who did not receive Vit-D (ICU admission rate, mechanical ventilation, length of hospitalization, mortality rate).
A senior author (M.M.A.) reviewed the extraction sheet, and any disagreement was solved by discussion amongst the aforementioned investigators by debate, consensus, or arbitration. The included studies were divided into two main groups: those that evaluated Vit-D deficiency on clinical outcomes in people with COVID-19, and those that evaluated the effect of Vit-D supplementation on clinical outcomes.
Quality assessment
M.A.A. and I.M.E., two independent authors, assessed the risk of bias in the included studies using two validated tools: First, the tool for bias assessment, the Cochrane risk assessment for randomized controlled trials (RCTs), is in chapter 8.5 of the Cochrane Handbook of Systematic Reviews of Interventions, 5.1.0. This tool consists of six domains (selection bias, performance bias, detection bias, attrition bias, reporting bias, and any other bias). Bias is assessed as a judgment. Each domain’s risk of bias was graded as “low,” “unclear,” or “high.” Thus, a study with appropriate processes in all domains was classified as having a low risk of bias, whereas a study with deficient procedures in at least one category was rated as having a high risk of bias. In all other instances, studies were classified as having an uncertain risk of bias17.
Secondly, the Methodological Index for Non-Randomized Studies Scale (MINORS), which is a valid instrument to assess 12 items, the first eight of which are specifically for non-comparative and single-arm studies, a third reviewer settled any disagreements.
Data Synthesis
At a level of significance p-value was < 0.05. We pooled continuous data as the mean difference (MD) with a 95% Confidence Interval (C.I) and dichotomous data as the risk ratio (RR) with a 95% C.I. All data were analyzed using Open Meta Analyst software for Windows; an open-source, cross-platform software for advanced meta-analysis. Statistical heterogeneity between studies was assessed by the Chi-squared (x2) and I-squared tests. Heterogeneity was evaluated as low, moderate, or high, with upper limits for I2 of 25%, 50%, and 75%, respectively. When the I2 value was 50% and the p-value= 0.05, heterogeneity was considered significant in the current meta-analysis. Using the random-effects model, considerable heterogeneity was reanalyzed and reported for the outcomes. Subgroup analysis was performed based on Vit-D levels (< 50 000, 50 000 – 10 000, > 100 000 International Unit (IU), etc.) and Vit-D supplementation (doses, the timing of administration, etc.), to clarify how efficacy differed and to reduce heterogeneity among the included studies.
Ethical considerations
The data collection took place in accordance with the Bahrain Personal Data Protection Law (PDPL) and the European Data Protection Regulation. As it’s a systematic review and meta-analysis, we used secondary data from ethically approved studies, and the results were collected anonymously.
Results
Study selection
We found 5609 references in five different databases: Cochrane, Web of Science, PubMed, Scopus, and EBSCO. Only 126 references underwent a full-text screening phase. In the end, our analysis included 8001 COVID patients from 12 randomized control trials, 3 quasi-experimental trials, and 27 non-randomized control trials. [Fig. 1] illustrates the selection process through a PRISMA flowchart.
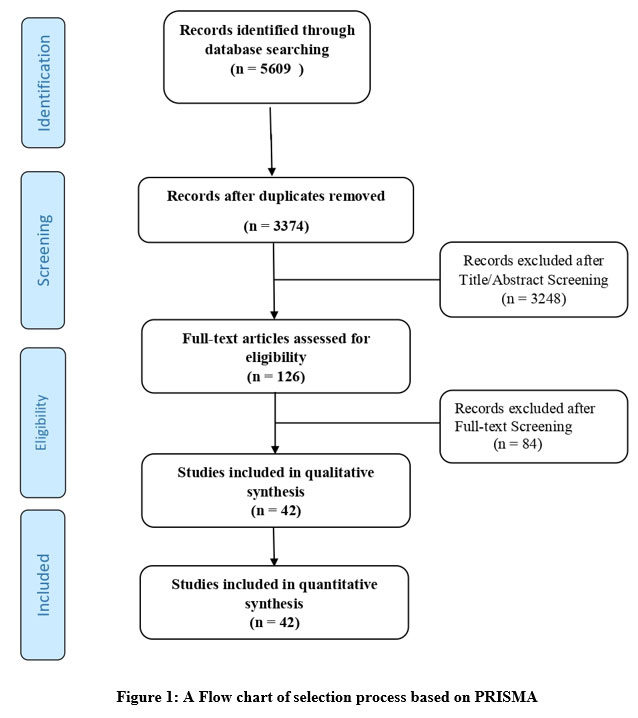 |
Figure 1: A Flow chart of selection process based on PRISMA |
Fundamental Characteristics
A summary of the baseline characteristics is shown in [Tables 1 and 2]. The included studies were classified into two groups.
The vitamin D deficiency group consisted of 22 studies that evaluated the correlation between serum Vit-D levels and various clinical outcomes. This group included 3979 patients with a mean age of 62 years, and the male-to-female ratio was four to three.
The vitamin D-supplemented group consisted of 20 studies that looked at how vitamin D supplementation affects different clinical outcomes. These studies included 4022 COVID patients with a mean age of 64 years, and the male-to-female ratio was six to five. The included studies took place in different countries with patients of different ethnicities.
Table 1: A summary of the baseline characteristics of included studies that assess the effect of serum Vitamin D levels on several clinical outcomes in Covid-19 patients.
| Study ID | Country/ Centers |
Year | Health status |
Total Sample size | Age (yr) | SexM/F | Design of the study | Main findings |
| Demir 2021 | Turkey | 2021 | Adult positive COVID-19 patients |
227 | 45.2 ± 17.6 | 98/129 | A Retrospective cohort | The risk of getting COVID-19 increased in vit-D deficient people. COVID-19 cases with sufficient vit-D levels significantly showed shorter |
| Lau 2020 | USA | 2020 | COVID-19 patients |
20 | 65.2 ± 16 | 44/15 | A Retrospective observational cohort | Vitamin D insufficiency was associated with COVID-19 severity and ICU admission rates. |
| Bianconi 2021 | Italy | 2021 | Mild, moderate, and severe COVID-19 patients |
250 | 74 ± 15 | 110/90 | A prospective cohort study | No association between serum vit-D level and COVID-19 patients prognosis. |
| Bennouar 2021 | Algeria | 2020 | severe to critical cases of this infection. | 120 | 62.3 ± 17.6 | 83/37 | A prospective cohort study | Severe COVID-19 cases showed low serum calcium and vit-D levels. |
| Reis 2021 | Brazil | 2020 | Moderate to severe COVID-19 |
220 | 55.1 ± 14.6 | 117/103 | A prospective cohort study | Patients with reduced 25OHD levels (<10 ng/mL) showed longer hospitalization duration than those with higher levels. |
| Baktash 2020 | UK | 2020 | COVID-19 patients |
70 | 81 ± 9.25 | 42/28 | A prospective cohort study | Worse COVID-19 prognosis was associated with hypovitaminosis D and older ages. |
| Ricci 2021 | Italy | 2021 | COVID-19 patients | 52 | 68.4 ± 16.2 | 25/27 | retrospective | COVID-19 cases with hypovitaminosis D exhibited attenuated inflammatory response and increased respiratory involvement. |
| Campi 2021 | Italy | 2020 | Mild and severe COVID-19 patients | 361 | 66.1 ± 14.1 | 101/54 | A prospective cohort study | An inverse correlation was found between reduced 25OHD and elevated IL-6 concentrations, both levels independently predicted the severity and mortality of COVID-19. |
| Orchard 2021 | UK | 2020 | critically ill COVID-19 | 50* | 9.4 ± 12 | 28/22 | A cohort study | This small sized study didn’t detected any difference in the prognosis of critical COVID-19 cases . |
| Herrera-Quintana 2021 | Granada (Spain) |
2021 | Severe ICU COVID-19 patients | 37 | 60.0 ± 10.2 | 26/11 | A prospective analytical study | High prevalence of vit-D deficiency in all critical patients at ICU admission, that increased after only three days of ICU stay. |
| Sulli 2021 | Italy | 2021 | severe respiratory failure and all patients needed hospitalization | 130 | 76 ± 13 | 60/70 | A prospective cohort study | Vitamin D deficiency was significantly associated with higher risk of respiratory complications and death in elderly COVID-19 cases. |
| ÖZGER 2021 | Turkey | 2021 | Uncomplicated, mild and severe COVID-19 infections. | 196 | 44.2 ± 21.2 | 87/109 | A cohort study | Vitamin D deficiency was associated with higher risk of COVID-19 positivity and wasn’t associated with the severity of the condition or the prognosis. |
| Maghbooli 2020 | Iran | 2020 | Severe COVID-19 infection |
235 | 58.7 ± 15.2 | 144/91 | A cohort study | Improving vitamin D status in the general population and in particular hospitalized patients has a potential benefit in reducing the severity of morbidities and mortality associated with acquiring COVID-19. |
| Jevalikar 2021 | India | 2021 | Hospitalized patients with COVID-19 infection | 409 | 52.4 ± 16.8 | 282/127 | A prospective, single-center, cross-sectional, observational study | No correlation between serum 25-OHD levels with COVID-19 prognosis or risk of death |
| Angelidi 2021 | USA | 2021 | Patients with COVID-19 infection | 144 | 65 ± 14.2 | 64/80 | A retrospective, observational, 2-center cohort study | An inverse correlation existed between 25OHD concentration and the rates of death and mechanical ventilation. |
| De Smet 2021 | Belgium | 2021 | Hospitalized patients with COVID-19 infection | 186 | 67 ± 21 | 109/77 | A retrospective observational study | Reduced serum 25OHD concentration was associated with higher risk of death. |
| Charoenngam 2021 | USA | 2021 | Hospitalized patients with COVID-19 | 287 | 61.9 ± 15.8 | 124/163 | A retrospective chart review cross-sectional study | Sufficient serum 25-OHD levels independently decrease the death risk in older hospitalized COVID-19 cases. |
| AlSafar 2021 | UAE | 2021 | Patients with COVID-19 infection | 464 | 46.6 ± 14.9 | 372/92 | A multicenter observational study | Low serum 25OHD levels were associated with the severity of COVID-19 and related mortality. |
| Carpagnano 2021 | Italy | 2020 | Hospitalized adult inpatients with COVID-19 |
42 | 65 ± 13 | 30/12 | A retrospective, observational study | Severe hypovitaminosis D was significantly associated with a higher risk of death. |
| Radujkovic 2020 | Germany | 2020 | Consecutive symptomatic COVID-19-positive patients |
185 | 59.6 ± 15.7 | 95/90 | A prospective non-interventional register | This study demonstrated an association between Vit-D deficiency and mortality. |
| Vassiliou 2021 | Greece | 2021 | Consecutive COVID-19 patients |
39 | 61.2 ± 13 | 31/8 | An observational, single-center study | Patients with vit-D deficiency had a higher death risk. |
| Vassiliou 2020 | Greece | 2020 | Consecutive, critically ill COVID-19 patients |
30 | 65 ± 11 | 24/8 | A prospective, observational study | Patients who died in the ICU within 28 days showed lower 25OHD levels on ICU admission compared to survivors. |
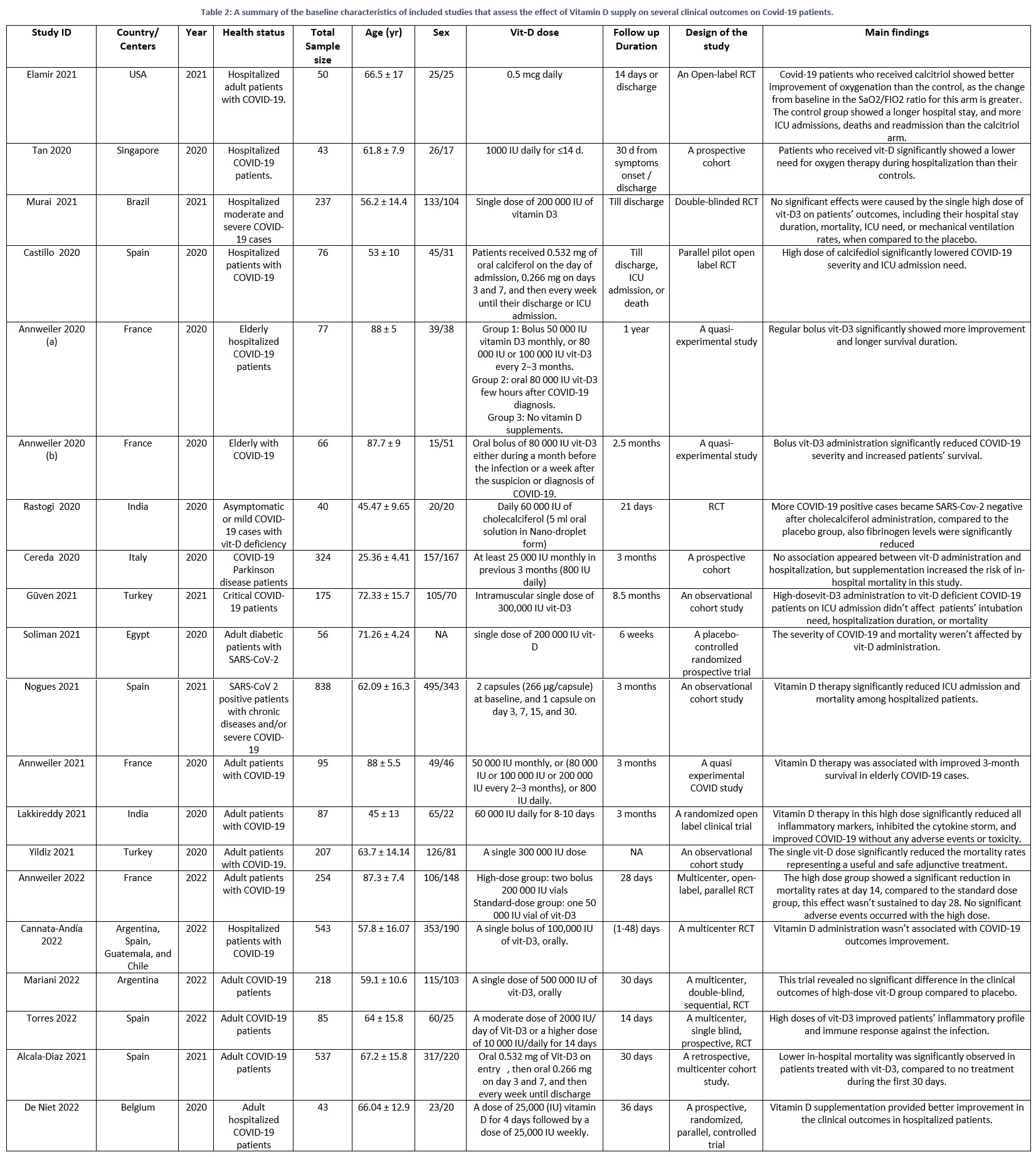 |
Table 2: A summary of the baseline characteristics of included studies that assess the effect of Vitamin D supply on several clinical outcomes on Covid-19 patients. |
Risk of bias in evaluation
Using the Cochrane risk of bias tool for Randomized Control Trials (RCTs), three studies: Castillo et al.20, Mariani et al.21, and Murai et al.22 were of good quality; De Niet 23 was of fair quality; and the rest of the studies were of low quality24–30. [Supplementary Fig. 1].
Based on the MINORS criteria for evaluating the quality of non-randomized studies, comparative studies had a range of 16 to 22 points, with a median of 20 points. Nogues et al.31 had the highest score (22 points), while Yildiz et al.32 had the lowest score (16 points). Non-comparative ones had a range of 6–13 points with a median of 10 points. Jevalikar et al.33, and Reis et al.34, had the highest score (13 points), while Vassiliou et al. 35, had the lowest score (6 points). [Sup. Table.1]
Outcomes
Outcomes pooled analysis in vitamin D-deficient COVID-19 patients
Regarding the mortality rate, the analysis of the pooled studies significantly favored the group with high serum Vit D levels (8.07%) over the group with low Vit D levels (14.09%) (RR = 1.54, 95% CI = 1.15: 2.05, p value = 0.01). Pooled results were homogeneous (p value = 0.37, I2 = 7.05%). [Fig.2a]. Concerning the rate of admission to the ICU (RR = 1.18, 95% CI = 0.97: 1.43, p value = 0.09; [Fig. 2b]); mechanical ventilation (RR = 1.06, 95% CI = 0.82: 1.37, p-value = 0.64; [Fig. 3a]); and length of hospitalization (MD = 0.05, 95% CI = -3.04: 3.14, SE = 1.58, p value = 0.97; [Fig. 3b]), pooled studies were heterogeneous.
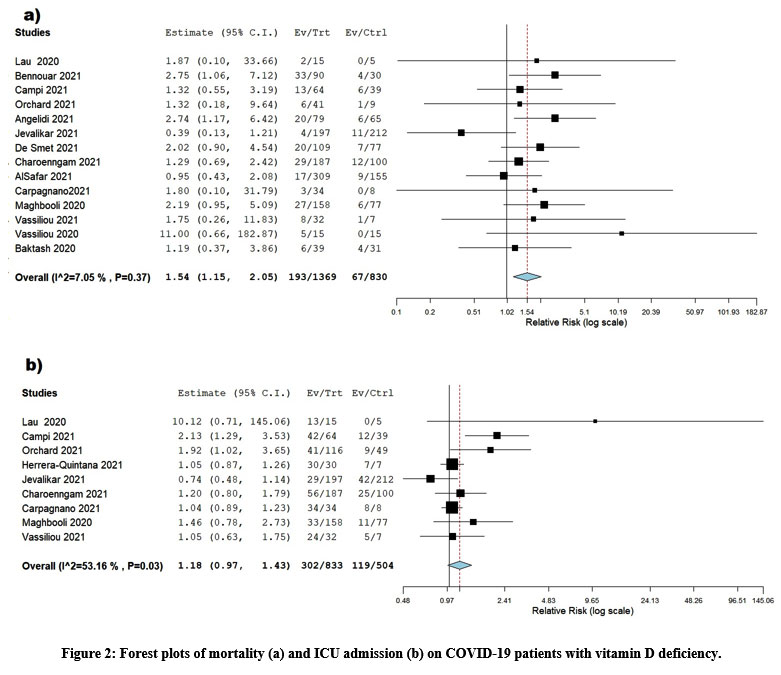 |
Figure 2: Forest plots of mortality (a) and ICU admission (b) on COVID-19 patients with vitamin D deficiency. |
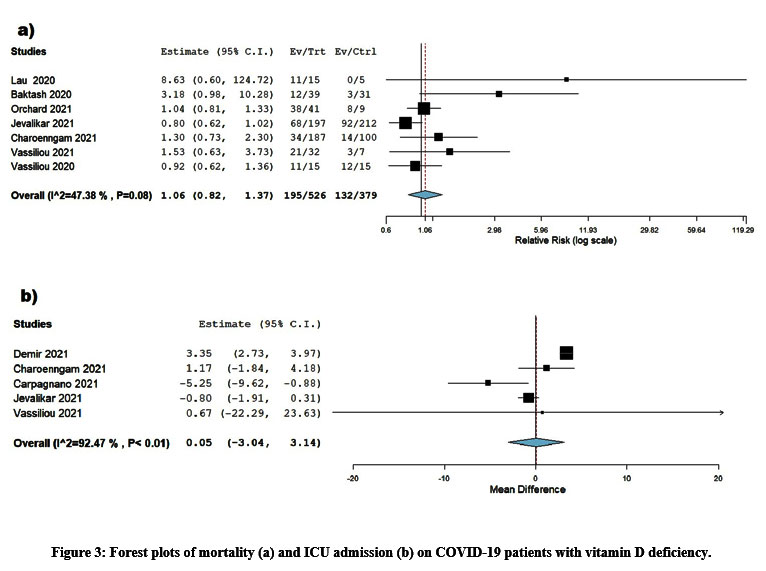 |
Figure 3: Forest plots of mortality (a) and ICU admission (b) on COVID-19 patients with vitamin D deficiency. |
Outcomes pooled analysis in COVID-19 patients who received Vit-D supplementation vs. COVID-19 patients without Vit-D supplementation
The analysis showed significant differences between the two groups. Regarding the mortality rate, the pooled effect estimate revealed that the Vit-D group had a significantly lower mortality rate (9.7%) than the control group (15.29%), and the results were statistically significant (RR = 0.64, 95% CI = 0.45: 0.92, p-value = 0.02). The studies were diverse (p-value = 0.01, I2 = 57.575%). [Fig.4a]
Regarding the rate of admission to the ICU and mechanical ventilation, the Vit-D receiving group had significantly (p-value = 0.01) fewer admission rates than the control group (RR = 0.48, 95% CI = 0.25: 0.85, p-value =0.01) and (RR = 0.70, 95% CI = 0.57: 0.87) [Fig. 4b, Fig. 5a], respectively.
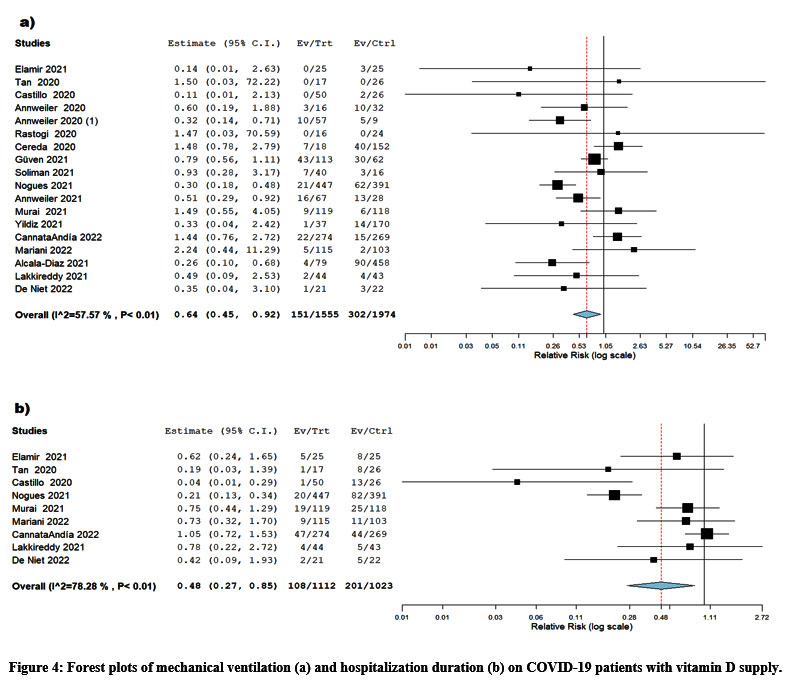 |
Figure 4: Forest plots of mechanical ventilation (a) and hospitalization duration (b) on COVID-19 patients with vitamin D supply. |
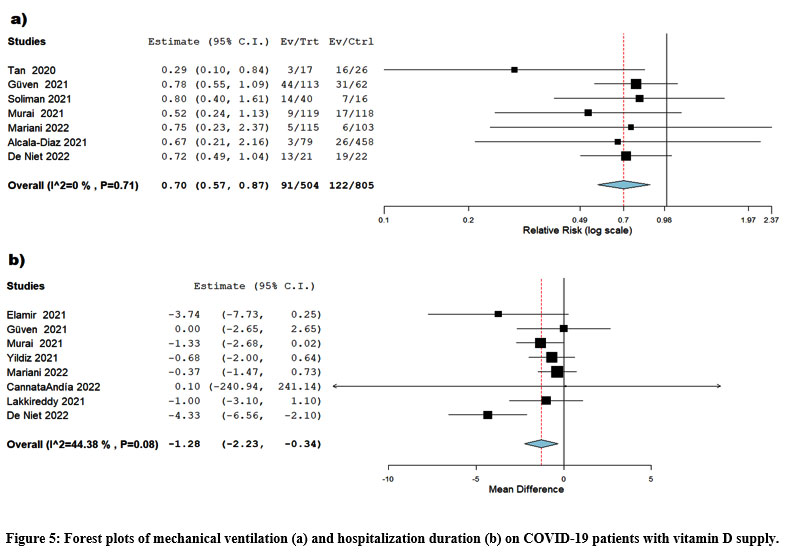 |
Figure 5: Forest plots of mechanical ventilation (a) and hospitalization duration (b) on COVID-19 patients with vitamin D supply. |
Concerning the length of hospitalization, vitamin D supplementation was significantly (p-value = 0.01) associated with shorter hospitalization duration (MD = -1.28, 95% CI). CI = -2.23, -0.34, SE = 0.48). The studies were homogenous (p-value = 0.08, I2 = 44.38%). [Fig.5b]
Subgroup and sensitivity analysis
The analysis of the subgroup of different Vit-D doses for mortality revealed a significant reduction in mortality in the group that received doses ranging from 50 000 to less than 100 000 IU compared to groups that received doses ranging from 50 000 IU to > 100 000 IU. The pooled data were homogeneous (p-value= 0.73, I2 = 0%) (RR = 0.42, 95% CI = 0.23: 0.76, p-value=0.005).
We conducted a subgroup analysis according to Vit-D levels in COVID patients. The results of the analysis didn’t show any clear differences in mortality or ICU admission rates among the groups with high and low levels of Vit-D.
We discovered a significant reduction in mortality rates of receiving Vit-D supplementation over placebo after excluding ICU admission rates after excluding Murai et al. (RR = 0.23, 95% CI = 0.09: 0.56, p-value= 0.01) and Nogues et al (RR = 0.67, 95% CI = 0.46: 0.98, p-value= 0.04)36,22.
We discovered that high Vit-D levels outperformed low Vit-D levels in ICU admission rates after excluding Campi et al.37 and mechanical ventilation rates after excluding Jevalikar et al.33, while low concentration levels outperformed high concentration levels in hospital duration outcomes after excluding Demir et al.38.
Discussion
Vitamin D deficiency and the clinical outcome among COVID-19 patients
As regards the clinical outcome, our analysis significantly favored the high serum Vit-D concentration group over the low concentration group as regards hospitalization duration, ICU admission rates, and the need for mechanical ventilation. In agreement with other studies that found evidence of a link between vitamin D deficiency and the severity of COVID-19 and associated deaths7,39,40. Moreover, other systematic reviews and meta-analyses revealed a negative correlation between serum vitamin D levels and the severity of COVID-19 patients 8, 41–43.
Concerning SARS-CoV-2 infection rates, numerous observational studies 44–47investigated the low levels of serum Vit-D as a risk factor for SARS-CoV-2 infection, including a previous retrospective observational study, which included 191,779 COVID-19 patients, that proved that the rates of SARS-CoV-2 positivity were independently associated with lower circulating 25-hydroxyvitamin D levels (25-OHD). Even though the 25-OHD level is important for all races and ethnicities, patients from predominantly black non-Hispanic zip codes had a higher SARS-CoV-2 positivity rate than patients from predominantly white non-Hispanic zip codes with the same 25-OHD level. This suggests that patients’ ethnicity may affect their risk of getting COVID-19.
This vitamin D deficiency might be attributed to several hypotheses that had been tested in order to determine the relationship between Vit-D and COVID-19. First, vitamin D activates cathelicidin (LL-37), and defLL-37 acts at various stages of viral infection, regardless of whether the virus is enveloped or not. Increased serum levels of OREL-37 are known to correlate with decreased expression of interleukin (IL-17), which is implicated in COVID-19 pathophysiology, including the development of thrombosis and acute respiratory distress syndrome (ARDS)48–51. As a result, the association between vitamin D and the severity and acute complications of COVID-19 may be explained by an increase in IL-17. Second, vitamin D modulates cytokine production by upregulating anti-inflammatory cytokines like IL-10 and downregulating pro-inflammatory cytokines like IL-1, IL-6, and tumor necrosis factor-alpha. This transition from pro-inflammatory to anti-inflammatory cytokines can minimize the danger of the cytokine storm induced by the COVID-19 infection. Finally, Vit-D stimulates the renin-angiotensin-aldosterone system and angiotensin-converting enzyme 2 (ACE2), which are important in lung protection against ARDS due to their anti-inflammatory and antioxidant properties. In fact, ACE2 is proven to protect against lethal avian influenza 53–55 and may protect against acute lung injury 7, 39, 40, 46, 47, 56.
Vitamin D supplementation and the clinical outcome among COVID-19 patients
As regards the clinical outcomes, this meta-analysis showed that Vit-D supplements significantly improved the clinical outcome (mortality rates, duration of hospitalization , ICU admission rates, and mechanical ventilation) in COVID-19 patients who received Vit-D supplements versus patients who did not receive any supplementation. In agreement with other studies that reported the beneficial effect of Vit-D supplements in improving the clinical outcomes of COVID-19 patients, especially mortality and ICU admission rates, this was confirmed in multiple observational and experimental investigations56–60, whether administered before or after a COVID-19 diagnosis.
Nevertheless, contradictory evidence suggests that there is no link between Vit-D administration and clinical outcomes 22, 33, 61. The majority of these studies did not give risk estimates for clinical outcomes that were adjusted for potential confounding factors 22, 33, 61. We believe that the present meta-analysis introduces comprehensive pooled data regarding the response of COVID-19 patients to Vit-D supplementation. However, only three trials were included in the meta-analysis. Moreover, the authors published only unadjusted risk estimates, omitting to account for potential confounding variables 22. In contrast, we combined data from 13 studies and offered both the adjusted and unadjusted risk estimates in order to draw more reliable and generalizable conclusions.
As regards the timing of administering Vit-D, the subgroup analysis revealed that administering Vit-D after a COVID-19 diagnosis is more beneficial than receiving it before the diagnosis, which is consistent with the other two studies that were included in the subgroup analysis and used a cumulatively high dose of cholecalciferol and calcifediol 57,58. On the other hand, detecting the optimum dose and duration of Vit-D administration as a possible adjuvant treatment for COVID-19 needs further exploration.
Except for Murai et al. and Lakkireddy et al.22-27, no study addressed the effect of vitamin D supplementation on increasing serum 25-OHD levels. Despite the inability to determine the precise dose of 25-OHD required to produce its immunomodulatory effect, levels of 25OHD greater than 30 ng/ml are thought to cause a significant reduction in COVID-19 severity and mortality62.
Relating to the number of doses of Vit-D administration, without detecting serum 25-hydroxyvitamin D levels, the most effective treatment plan, whether a single high-dose bolus or a daily modest dose of Vit-D, is still unknown. High-dose bolus vitamin D stimulates the long-term production of 24-hydroxylase and fibroblast growth factor 23 (FGF23). Increased production of 24-hydroxylase results in the conversion of 25-OHD to the inactive metabolite 24,25-dihydroxy Vit-D, and FGF23 results in the inactivation of the enzyme renal 1-hydroxylase, reducing the active metabolite calcitriol. A daily vitamin D intake, on the other hand, has a longer-lasting effect on 25-hydroxy vitamin D levels64.In this manner, receiving Vit-D maintenance doses after a single bolus dose is anticipated to maintain adequate vitamin D levels for an extended period.
Despite evidence of high heterogeneity among trials, Vit-D supplementation was safe and lowered the risk of COVID-19 outcomes. Protection was associated with daily 400-1000 IU vitamin D supplementation for up to 12 months. Unknown and requiring examination is the significance of these findings for COVID-19 68.
Doses of vitamin D supplements for mortality among COVID-19 patients
Two previous meta-analyses65, 66 revealed that daily low doses of vitamin D were effective in the prevention of acute respiratory tract infections. The purpose of our study was to examine whether the subgroup of different vitamin D doses was related to the mortality rate, and we found that the group that received doses between 50 000 to 100 000 IU, performed significantly better than the other groups. This may be because physiological doses of Vit-D supplementation manage to achieve commonly accepted levels of 25-OHD when compared to larger doses, as proposed by Binkley and colleagues67.
In this light, high doses of vitamin D could produce “drug-like” effects not found with “supplement” dosages. So that we would have the best chance of finding a good effect in patients with life-threatening COVID-19, the dosing schedule for our trial was set up to quickly reach and keep serum levels that were as high as could be done safely68. The risk of these adverse events increases when serum concentrations of 25-OHD are greater than 125 nmol/L.
Strength
This systematic review and meta-analysis search was carried out from PubMed, Cochrane Library, Scopus, Web of Science, and EBSCO, for relevant studies for the long period up to May 2022, targeting 8001 COVID-19 patients. We studied the association between four central clinical outcomes, the mortality rates, duration of hospitalization, ICU admission rates, and mechanical ventilation rates, related to vitamin D deficiency and its supplementation in patients affected by COVID-19, searching for the most adequate doses which improved the clinical outcomes in these patients. This systematic review may contribute to confirming the relationship between vitamin D deficiency and COVID-19, and it also provided strong indications on the role of Vit-D supplementation in improving patients and determining the most appropriate doses.
Limitations
Despite our strengths, the meta-analysis showed several flaws. First, some studies did not provide adjusted estimates, so we could not include them in the adjusted pooled analysis. Additionally, the covariates in the included research were inconsistent, and the OR/HR calculated from the studies was corrected for various factors. Second, vitamin D was administered to all patients regardless of their baseline 25-OHD levels in most studies, which limited the ability to detect the difference in the effect of receiving vitamin D on people with and without hypovitaminosis D. All studies rarely told us what the 25-OHD levels were at the start, so we couldn’t do a subgroup analysis based on the 25-OHD levels at the start.
Third, the time lag between the development of COVID-19 symptoms and the supplementation of Vit-D was insufficiently described, so conducting a subgroup analysis based on this time lag was not possible. Notably, vitamin D administration occurred 10.3 days (on average) after the onset of symptoms, which may have negated the positive effects of vitamin D if supplemented earlier in the disease course. Fourth, reporting the data on COVID-19 severity was infrequent and inconsistent across all studies, which limited performing a subgroup analysis depending on the severity of the underlying condition. In addition, conducting another subgroup study displaying the effect of vitamin D administration on men and women would have been beneficial in light of the abundance of evidence showing intersex variations in COVID-19 severity. However, this was not possible due to the absence of such data.
Conclusion
This systematic review and meta-analysis came to the conclusion that compared to COVID-19 cases with hypovitaminosis D, cases with normal vitamin D levels significantly showed lower mortality rates. Vitamin D supplementation greatly improved death rates, length of hospital stays, ICU admission rates, and the need for mechanical ventilation, especially when this vitamin was given to patients after their diagnosis of COVID-19. Vitamin D supplementation between 50 000 to 100 000 IU, showed among COVID-19 patients significantly outperformed other doses in terms of mortality.
Recommendations
The detection of COVID-19 and the optimization of the dose and duration of Vitamin D administration as a possible adjuvant treatment require further investigation.
Acknowledgments
The authors would like to express their gratitude to all of the nurses who took part in this study. and those helped in organizing for the intervention sessions from the infection control unit in the hospitals.
Competing Interests
The authors have declared no conflicts of interest.
Funding Sources
This work was not funded by any agencies.
References
- WHO. Coronavirus (COVID-19) dashboard. s. f.
- Ramasamy S, Subbian S. Critical Determinants of Cytokine Storm and Type I Interferon Response in COVID-19 Pathogenesis. Clinical Microbiology Reviews. 2021;34.
CrossRef - Zhou F. Y u T, Du R, Fan G, Liu Y, Liu Z, et al. Clinical course and risk factors for mortality of adult inpatients with COVID19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395:1054-62.
CrossRef - Li J, Huang DQ, Zou B, Yang H, Hui WZ, Rui F, et al. Epidemiology of COVID‐19: A systematic review and meta‐analysis of clinical characteristics, risk factors, and outcomes. Journal of Medical Virology. 2021;93:1449-58.
CrossRef - Gold MS, Sehayek D, Gabrielli S, Zhang X, McCusker C, Ben-Shoshan M. COVID-19 and comorbidities: a systematic review and meta-analysis. Postgraduate Medicine. 2020;132:749-55.
CrossRef - Petrilli CM, Jones SA, Yang J, Rajagopalan H, O’Donnell L, Chernyak Y, et al. Factors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: prospective cohort study. BMJ. 2020:m1966.
CrossRef - Munshi R, Hussein MH, Toraih EA, Elshazli RM, Jardak C, Sultana N, et al. Vitamin D insufficiency as a potential culprit in critical COVID‐19 patients. Journal of Medical Virology. 2021;93:733-40.
CrossRef - Pereira M, Dantas Damascena A, Galvão Azevedo LM, de Almeida Oliveira T, da Mota Santana J. Vitamin D deficiency aggravates COVID-19: systematic review and meta-analysis. Critical Reviews in Food Science and Nutrition. 2022;62:1308-16.
CrossRef - Holick MF. Vitamin D Deficiency. New England Journal of Medicine. 2007;357:266-81.
CrossRef - Grant W, Lahore H, McDonnell S, Baggerly C, French C, Aliano J, et al. Evidence that Vitamin D Supplementation Could Reduce Risk of Influenza and COVID-19 Infections and Deaths. Nutrients. 2020;12:988.
CrossRef - Gombart AF, Pierre A, Maggini S. A Review of Micronutrients and the Immune System–Working in Harmony to Reduce the Risk of Infection. Nutrients. 2020;12:236.
CrossRef - Weir EK, Thenappan T, Bhargava M, Chen Y. Does vitamin D deficiency increase the severity of COVID-19? Clinical Medicine. 2020;20:e107-8.
CrossRef - Mohammad, Mishra, Ashraf. Emerging Role of Vitamin D and its Associated Molecules in Pathways Related to Pathogenesis of Thrombosis. Biomolecules. 2019;9:649.
CrossRef - Lei G-S, Zhang C, Cheng B-H, Lee C-H. Mechanisms of Action of Vitamin D as Supplemental Therapy for Pneumocystis Pneumonia. Antimicrobial Agents and Chemotherapy. 2017;61.
CrossRef - Suhail S, Zajac J, Fossum C, Lowater H, McCracken C, Severson N, et al. Role of Oxidative Stress on SARS-CoV (SARS) and SARS-CoV-2 (COVID-19) Infection: A Review. The Protein Journal. 2020;39:644-56.
CrossRef - Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JPA, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Journal of clinical epidemiology. 2009;62:e1-34.
CrossRef - Higgins JPT, Sterne JAC, Savovic J, Page MJ, Hróbjartsson A, Boutron I, et al. A revised tool for assessing risk of bias in randomized trials. Cochrane database of systematic reviews. 2016;10:29-31.
- Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J. Methodological index for non‐randomized studies (MINORS): development and validation of a new instrument. ANZ journal of surgery. 2003;73:712-6.
CrossRef - Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. Bmj. 2003;327:557-60.
CrossRef - Castillo ME, Costa LME, Barrios JMV, Díaz JFA, Miranda JL, Bouillon R, et al. Effect of calcifediol treatment and best available therapy versus best available therapy on intensive care unit admission and mortality among patients hospitalized for COVID-19: A pilot randomized clinical study. The Journal of steroid biochemistry and molecular biology. 2020;203:105751.
CrossRef - Mariani J, Antonietti L, Tajer C, Ferder L, Inserra F, Cunto MS, et al. High-dose vitamin D versus placebo to prevent complications in COVID-19 patients: Multicentre randomized controlled clinical trial. PLoS ONE. 2022;17:1-16.
CrossRef - Murai IH, Fernandes AL, Sales LP, Pinto AJ, Goessler KF, Duran CSC, et al. Effect of a single high dose of vitamin D3 on hospital length of stay in patients with moderate to severe COVID-19: a randomized clinical trial. Jama. 2021;325:1053-60.
CrossRef - De Niet S, Trémège M, Coffiner M, Rousseau A-F, Calmes D, Frix A-N, et al. Positive effects of vitamin D supplementation in patients hospitalized for COVID-19: a randomized, double-blind, placebo-controlled trial. Nutrients. 2022;14:3048.
CrossRef - Torres M, Casado G, Vigón L, Rodríguez-Mora S, Mateos E, Ramos-Martín F, et al. Changes in the immune response against SARS-CoV-2 in individuals with severe COVID-19 treated with high dose of vitamin D. Biomedicine & Pharmacotherapy. 2022;150:112965.
CrossRef - Cannata-Andía JB, Díaz-Sottolano A, Fernández P, Palomo-Antequera C, Herrero-Puente P, Mouzo R, et al. A single-oral bolus of 100,000 IU of cholecalciferol at hospital admission did not improve outcomes in the COVID-19 disease: the COVID-VIT-D—a randomised multicentre international clinical trial. BMC medicine. 2022;20:1-13.
CrossRef - Annweiler C, Beaudenon M, Gautier J, Gonsard J, Boucher S, Chapelet G, et al. High-dose versus standard-dose vitamin D supplementation in older adults with COVID-19 (COVIT-TRIAL): A multicenter, open-label, randomized controlled superiority trial. PLoS Medicine. 2022;19:1-18.
CrossRef - Lakkireddy M, Gadiga SG, Malathi RD, Karra ML, Raju ISSVPM, Ragini, et al. Impact of daily high dose oral vitamin D therapy on the inflammatory markers in patients with COVID 19 disease. Scientific Reports. 2021;11:1-8.
CrossRef - Soliman AR, Abdelaziz TS, Fathy A. Impact of Vitamin D Therapy on the Progress COVID-19: Six Weeks Follow-Up Study of Vitamin D Deficient Elderly Diabetes Patients. Proceedings of Singapore Healthcare. 2021;0:1-5.
CrossRef - Rastogi A, Bhansali A, Khare N, Suri V, Yaddanapudi N, Sachdeva N, et al. Short term, high-dose vitamin D supplementation for COVID-19 disease: A randomised, placebo-controlled, study (SHADE study). Postgraduate Medical Journal. 2022;98:87-90.
CrossRef - Elamir YM, Amir H, Lim S, Rana YP, Lopez CG, Feliciano NV, et al. A randomized pilot study using calcitriol in hospitalized COVID-19 patients. Bone. 2022;154.
CrossRef - Nogues X, Ovejero D, Pineda-Moncusí M, Bouillon R, Arenas D, Pascual J, et al. Calcifediol treatment and COVID-19–related outcomes. The Journal of Clinical Endocrinology & Metabolism. 2021;106:e4017-27.
CrossRef - Yildiz M, Senel MU, Kavurgaci S, Ozturk FE, Ozturk A. The prognostic significance of vitamin D deficiency in patients with COVID-19 pneumonia. Bratislavske Lekarske Listy. 2021;122:744-7.
CrossRef - Jevalikar G, Mithal A, Singh A, Sharma R, Farooqui KJ, Mahendru S, et al. Lack of association of baseline 25-hydroxyvitamin D levels with disease severity and mortality in Indian patients hospitalized for COVID-19. Scientific reports. 2021;11:1-8.
CrossRef - Reis BZ, Fernandes AL, Sales LP, Santos MD, Dos Santos CC, Pinto AJ, et al. Influence of vitamin D status on hospital length of stay and prognosis in hospitalized patients with moderate to severe COVID-19: a multicenter prospective cohort study. American Journal of Clinical Nutrition. 2021;114:598-604.
CrossRef - Vassiliou AG, Jahaj E, Pratikaki M, Keskinidou C, Detsika M, Grigoriou E, et al. Vitamin D deficiency correlates with a reduced number of natural killer cells in intensive care unit (ICU) and non-ICU patients with COVID-19 pneumonia. Hellenic Journal of Cardiology. 2021;62:381.
CrossRef - Nogues X, Ovejero D, Pineda-Moncusí M, Bouillon R, Arenas D, Pascual J, et al. Calcifediol treatment and COVID-19–related outcomes. The Journal of Clinical Endocrinology & Metabolism. 2021;106:e4017-27.
CrossRef - Campi I, Gennari L, Merlotti D, Mingiano C, Frosali A, Giovanelli L, et al. Vitamin D and COVID-19 severity and related mortality: a prospective study in Italy. BMC Infectious Diseases. 2021;21:1-13.
CrossRef - Demir M, Demir F, Aygun H. Vitamin D deficiency is associated with COVID-19 positivity and severity of the disease. Journal of Medical Virology. 2021;93:2992-9.
CrossRef - Radujkovic A, Hippchen T, Tiwari-Heckler S, Dreher S, Boxberger M, Merle U. Vitamin D deficiency and outcome of COVID-19 patients. Nutrients. 2020;12:2757.
CrossRef - Mariani J, Giménez VMM, Bergam I, Tajer C, Antonietti L, Inserra F, et al. Association between vitamin D deficiency and COVID-19 incidence, complications, and mortality in 46 countries: an ecological study. Health security. 2021;19:302-8.
CrossRef - Bassatne A, Basbous M, Chakhtoura M, El Zein O, Rahme M, Fuleihan GE-H. The link between COVID-19 and VItamin D (VIVID): a systematic review and meta-analysis. Metabolism. 2021;119:154753.
CrossRef - Teshome A, Adane A, Girma B, Mekonnen ZA. The impact of vitamin D level on COVID-19 infection: systematic review and meta-analysis. Frontiers in public health. 2021;9:624559.
CrossRef - Akbar MR, Wibowo A, Pranata R, Setiabudiawan B. Low serum 25-hydroxyvitamin D (vitamin D) level is associated with susceptibility to COVID-19, severity, and mortality: a systematic review and meta-analysis. Frontiers in nutrition. 2021;8:660420.
CrossRef - Kaufman HW, Niles JK, Kroll MH, Bi C, Holick MF. SARS-CoV-2 positivity rates associated with circulating 25-hydroxyvitamin D levels. PloS one. 2020;15:e0239252.
CrossRef - Heaney RP. Guidelines for optimizing design and analysis of clinical studies of nutrient effects. Nutrition reviews. 2014;72:48-54.
CrossRef - Pal R, Ram S, Zohmangaihi D, Biswas I, Suri V, Yaddanapudi LN, et al. High prevalence of hypocalcemia in non-severe COVID-19 patients: a retrospective case-control study. Frontiers in medicine. 2021;7:590805.
CrossRef - Meltzer DO, Best TJ, Zhang H, Vokes T, Arora V, Solway J. Association of vitamin D status and other clinical characteristics with COVID-19 test results. JAMA network open. 2020;3:e2019722-e2019722.
CrossRef - Grant WB, Lahore H, Rockwell MS. The benefits of vitamin D supplementation for athletes: better performance and reduced risk of COVID-19. Nutrients. 2020;12:3741.
CrossRef - Brice DC, Diamond G. Antiviral activities of human host defense peptides. Current medicinal chemistry. 2020;27:1420-43.
CrossRef - Raucci F, Mansour AA, Casillo GM, Saviano A, Caso F, Scarpa R, et al. Interleukin-17A (IL-17A), a key molecule of innate and adaptive immunity, and its potential involvement in COVID-19-related thrombotic and vascular mechanisms. Autoimmunity Reviews. 2020;19:102572.
CrossRef - Pacha O, Sallman MA, Evans SE. COVID-19: a case for inhibiting IL-17? Nature Reviews Immunology. 2020;20:345-6.
CrossRef - Bilezikian JP, Bikle D, Hewison M, Lazaretti-Castro M, Formenti AM, Gupta A, et al. Mechanisms in endocrinology: vitamin D and COVID-19. European journal of endocrinology. 2020;183:R133-47.
CrossRef - Malek Mahdavi A. A brief review of interplay between vitamin D and angiotensin‐converting enzyme 2: Implications for a potential treatment for COVID‐19. Reviews in medical virology. 2020;30:e2119.
CrossRef - Pal R, Bhansali A. COVID-19, diabetes mellitus and ACE2: the conundrum. Diabetes research and clinical practice. 2020;162.
CrossRef - Zou Z, Yan Y, Shu Y, Gao R, Sun Y, Li X, et al. Angiotensin-converting enzyme 2 protects from lethal avian influenza A H5N1 infections. Nature communications. 2014;5:1-7.
CrossRef - Baktash V, Hosack T, Patel N, Shah S, Kandiah P, Van den Abbeele K, et al. Vitamin D status and outcomes for hospitalised older patients with COVID-19. Postgraduate medical journal. 2021;97:442-7.
CrossRef - Giannini S, Passeri G, Tripepi G, Sella S, Fusaro M, Arcidiacono G, et al. Effectiveness of in-hospital cholecalciferol use on clinical outcomes in comorbid COVID-19 patients: a hypothesis-generating study. Nutrients. 2021;13:219.
CrossRef - Ling SF, Broad E, Murphy R, Pappachan JM, Pardesi-Newton S, Kong M-F, et al. High-dose cholecalciferol booster therapy is associated with a reduced risk of mortality in patients with COVID-19: a cross-sectional multi-centre observational study. Nutrients. 2020;12:3799.
CrossRef - Annweiler C, Hanotte B, de l’Eprevier CG, Sabatier J-M, Lafaie L, Célarier T. Vitamin D and survival in COVID-19 patients: A quasi-experimental study. The Journal of steroid biochemistry and molecular biology. 2020;204:105771.
CrossRef - Annweiler G, Corvaisier M, Gautier J, Dubée V, Legrand E, Sacco G, et al. Vitamin D supplementation associated to better survival in hospitalized frail elderly COVID-19 patients: the GERIA-COVID quasi-experimental study. Nutrients. 2020;12:3377.
CrossRef - Cereda E, Bogliolo L, Lobascio F, Barichella M, Zecchinelli AL, Pezzoli G, et al. Vitamin D supplementation and outcomes in coronavirus disease 2019 (COVID-19) patients from the outbreak area of Lombardy, Italy. Nutrition (Burbank, Los Angeles County, Calif). 2021;82:111055.
CrossRef - Maghbooli Z, Sahraian MA, Ebrahimi M, Pazoki M, Kafan S, Tabriz HM, et al. Vitamin D sufficiency, a serum 25-hydroxyvitamin D at least 30 ng/mL reduced risk for adverse clinical outcomes in patients with COVID-19 infection. PloS one. 2020;15:e0239799.
CrossRef - Griffin G, Hewison M, Hopkin J, Kenny RA, Quinton R, Rhodes J, et al. Perspective: Vitamin D supplementation prevents rickets and acute respiratory infections when given as daily maintenance but not as intermittent bolus: implications for COVID-19. Clinical Medicine. 2021;21:e144.
CrossRef - Ketha H, Thacher TD, Oberhelman SS, Fischer PR, Singh RJ, Kumar R. Comparison of the effect of daily versus bolus dose maternal vitamin D3 supplementation on the 24, 25-dihydroxyvitamin D3 to 25-hydroxyvitamin D3 ratio. Bone. 2018;110:321-5.
CrossRef - Jolliffe DA, Camargo Jr CA, Sluyter JD, Aglipay M, Aloia JF, Ganmaa D, et al. Vitamin D supplementation to prevent acute respiratory infections: a systematic review and meta-analysis of aggregate data from randomised controlled trials. The lancet Diabetes & endocrinology. 2021;9:276-92.
CrossRef - Iversen HH, Bjertnæs ØA, Skudal KE. Patient evaluation of hospital outcomes: an analysis of open-ended comments from extreme clusters in a national survey. BMJ open. 2014;4:e004848.
CrossRef - Binkley N, Ramamurthy R, Krueger D. Low vitamin D status: definition, prevalence, consequences, and correction. Endocrinology and Metabolism Clinics. 2010;39:287-301.
CrossRef - Rake C, Gilham C, Bukasa L, Ostler R, Newton M, Wild JP, et al. High-dose oral vitamin D supplementation and mortality in people aged 65-84 years: the VIDAL cluster feasibility RCT of open versus double-blind individual randomisation. Health Technology Assessment (Winchester, England). 2020;24:1.
CrossRef - Bandeira L, Lazaretti-Castro M, Binkley N. Clinical aspects of SARS-CoV-2 infection and vitamin D. Reviews in Endocrine and Metabolic Disorders. 2021:1-5.
CrossRef
Abbreviations
25-hydroxyvitamin D (25-OHD)
Acute respiratory distress syndrome (ARDS)
Angiotensin-converting enzyme 2 (ACE2)
Confidence interval (CI)
Hazard ratio (HR)
International Unit (IU)
Mean difference (MD)
Odds ratio (OR)
Population, Intervention, Comparison, Outcome, and Study Design(PICOs)
Randomized Control Trials (RCTs (
Randomized controlled trial (RCT)
Renin-angiotensin–aldosterone system (RAAS)
Risk ratio (RR)
The Coronavirus disease 2019 (COVID-19)
The Methodological Index for Non-Randomized Studies scale (MINORS)
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)
Titles and abstracts (TAs)
Vitamin D (Vit.D)
Scopus Citation(s): 5
Accepted on: 16 Mar 2023
Second Review by: Marlene Escobedo Monge Spain
Final Approval by: Dr Shih-Min Hsia





Web of Science Coverage
Emerging Sources Citation Index (ESCI)
2024 Journal Impact Factor: 1.1
Scopus Journal Metrics
CiteScore 2025: 2.6
CiteScore Details
Sustainable Nutrition: Food Systems, Nutrient Retention, and Public Health Impact
![]()
This journal is a member of, and subscribes to the principles of, the Committee on Publication Ethics (COPE)








